HEM ONC ACQUIRED HEMOLYTIC ANEMIA CLOTTING DISORDERS THROMBOTICS

HEM ONC ACQUIRED HEMOLYTIC ANEMIA CLOTTING DISORDERS THROMBOTICS AND ANTITHROMBOTICS EMERGENCY COMPLICATIONS OF MALIGNANCY

QUIZ

QUIZ

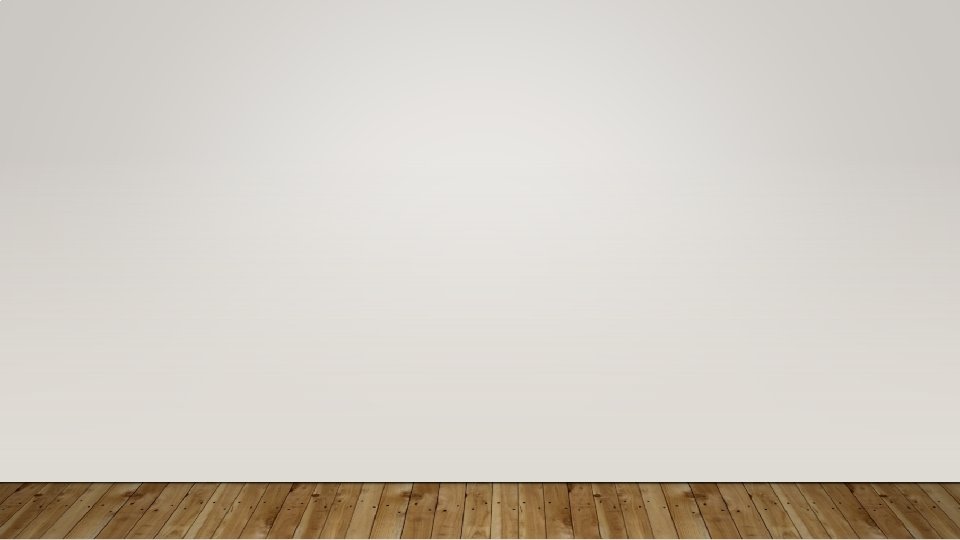
• PRBCs – 10 ml/kg

• What drugs doses do you want to know? Epinephrine – 0. 01 mg/kg Atropine - 0. 02 mg/kg Bicarb – 1 -2 m. Eq/kg Etomidate – 0. 3 mg/kg Ketamine – 0. 5 -2 mg/kg Rocuronium – 1 -1. 5 mg/kg PRBCs – 10 -20 ml/kg FFP – 10 -20 ml/kg Platelets – 5 -10 ml/kg Dextrose – 1 ml/kg D 50

• What drugs doses do you want to know? Epinephrine – 0. 01 mg/kg Atropine - 0. 02 mg/kg Bicarb – 1 -2 m. Eq/kg Etomidate – 0. 3 mg/kg Ketamine – 0. 5 -2 mg/kg Rocuronium – 1 -1. 5 mg/kg PRBCs – 10 -20 ml/kg FFP – 10 -20 ml/kg Platelets – 5 -10 ml/kg Dextrose – 1 ml/kg D 50

• What drugs doses do you want to know? Epinephrine – 0. 01 mg/kg Atropine - 0. 02 mg/kg Bicarb – 1 -2 m. Eq/kg Etomidate – 0. 3 mg/kg Ketamine – 0. 5 -2 mg/kg Rocuronium – 1 -1. 5 mg/kg PRBCs – 10 -20 ml/kg FFP – 10 -20 ml/kg Platelets – 5 -10 ml/kg Dextrose – 1 ml/kg D 50

• What drugs doses do you want to know? Epinephrine – 0. 01 mg/kg Atropine - 0. 02 mg/kg Bicarb – 1 -2 m. Eq/kg Etomidate – 0. 3 mg/kg Ketamine – 0. 5 -2 mg/kg Rocuronium – 1 -1. 5 mg/kg PRBCs – 10 -20 ml/kg FFP – 10 -20 ml/kg Platelets – 5 -10 ml/kg Dextrose – 1 ml/kg D 50

• What drugs doses do you want to know? Epinephrine – 0. 01 mg/kg Atropine - 0. 02 mg/kg Bicarb – 1 -2 m. Eq/kg Etomidate – 0. 3 mg/kg Ketamine – 0. 5 -2 mg/kg Rocuronium – 1 -1. 5 mg/kg PRBCs – 10 -20 ml/kg FFP – 10 -20 ml/kg Platelets – 5 -10 ml/kg Dextrose – 1 ml/kg D 50

ACQUIRED HEMOLYTIC ANEMIA

BIGGEST TAKEAWAY If you can’t explain an anemia, consider hemolytic

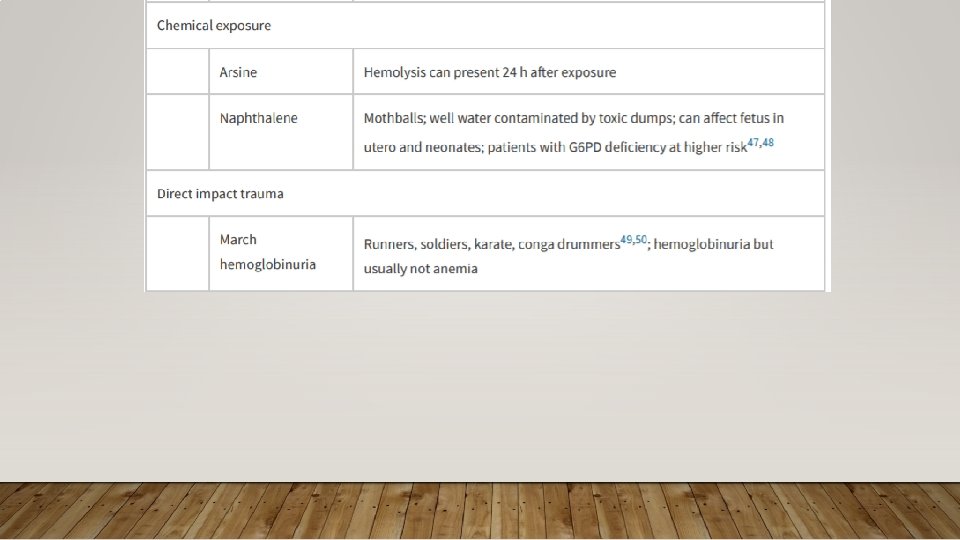
ACQUIRED HEMOLYTIC ANEMIA • Immune Mediated • Microangiopathic Syndromes • Macrovascular Hemolysis

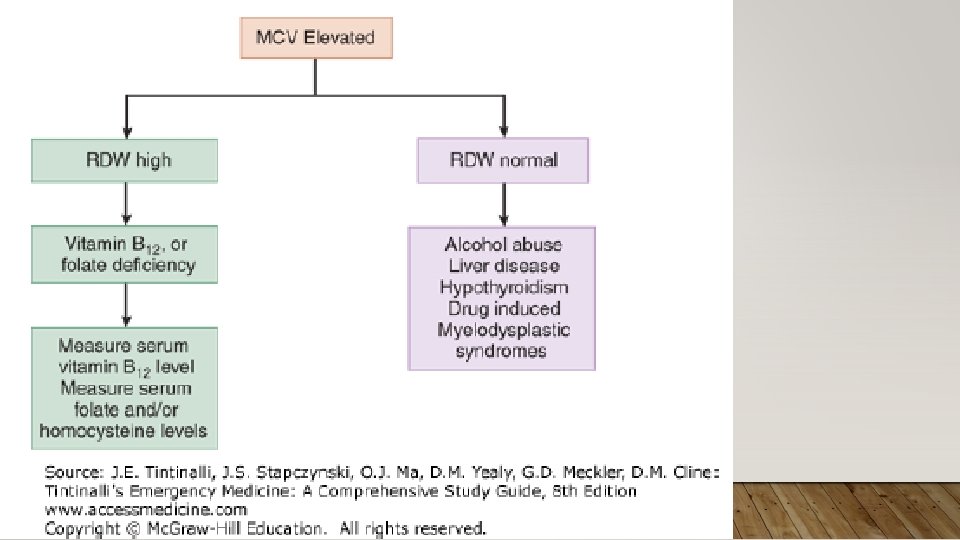
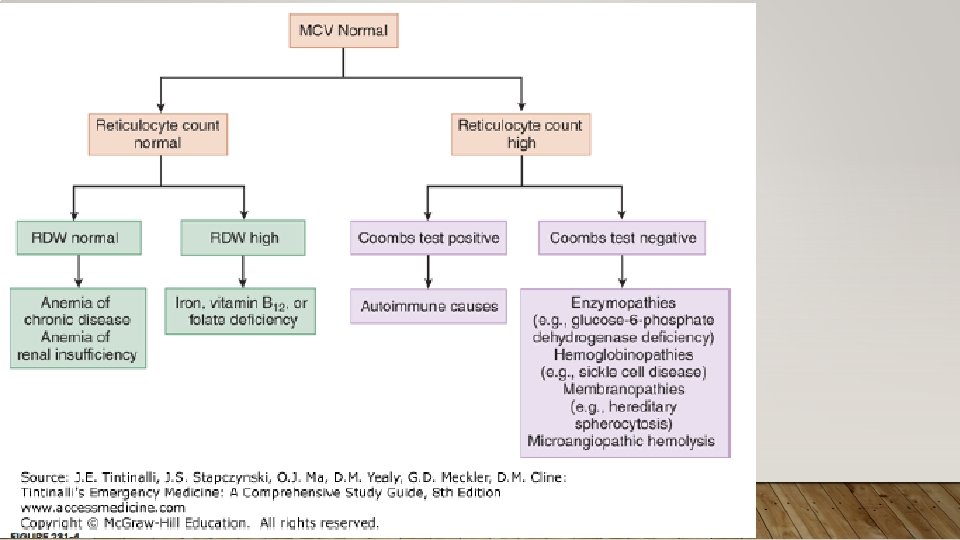
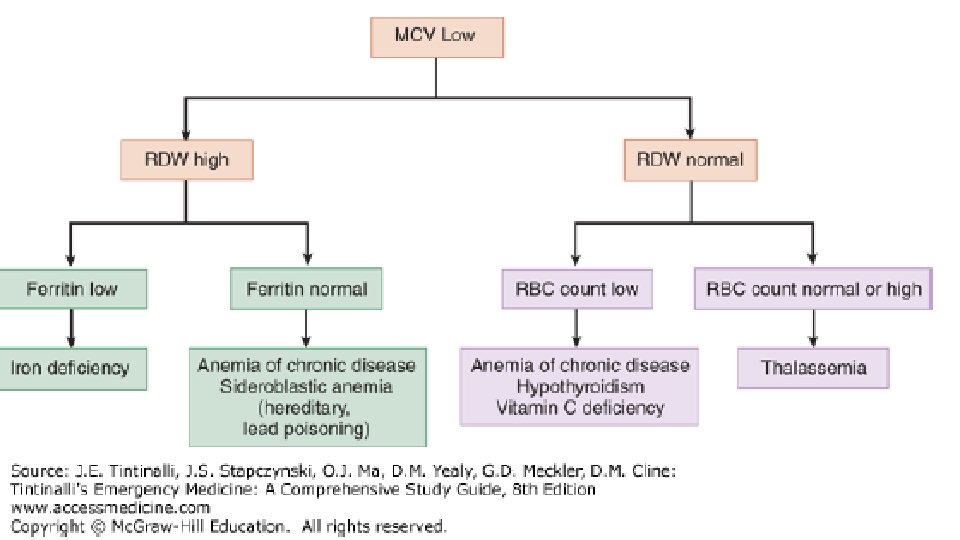
ACQUIRED HEMOLYTIC ANEMIA • Hemolysis of RBCs not due to congenital or inherited disorders • Can intravascular or extravascular (spleen, liver) • Symptomatic hemolytic anemia: weakness, fatigue, dizziness, SOB, DOE, tachycardia, cardiac murmur, pallor, jaundice, darkened urine, *splenic enlargement • Lab Findings:

QUIZ

REVIEW • Decreased • Hgb/Hct • Haptoglobin • Increased • Retic Count • LDH • Total & Indirect Bilirubin • Potassium • Present • Schistocytes (intravascular) • Spherocytes (extravascular) • Hemoglobinuria • Urobilinogen

ACQUIRED HEMOLYTIC ANEMIA • Immune Mediated • Microangiopathic Syndromes • Macrovascular Hemolysis

ACQUIRED HEMOLYTIC ANEMIA • Immune Mediated • Microangiopathic Syndromes • Macrovascular Hemolysis

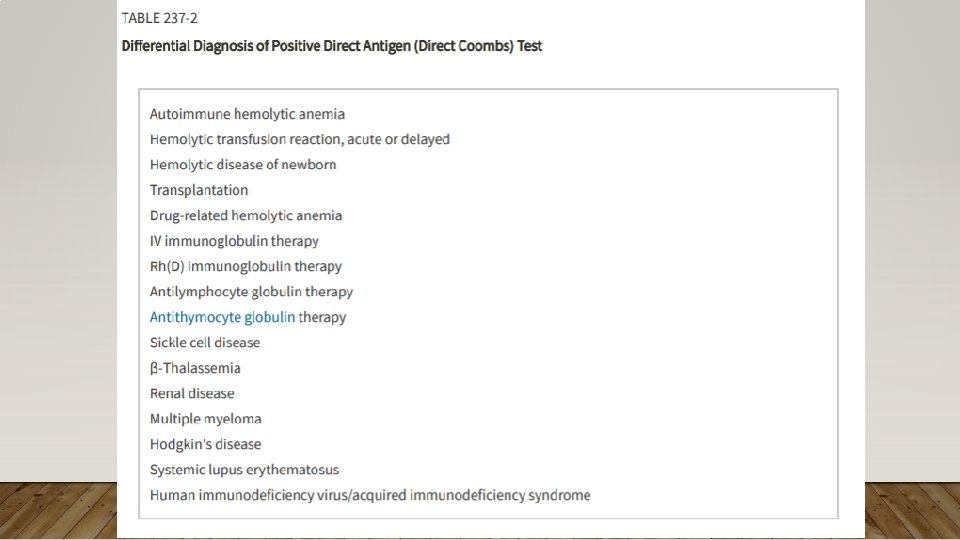
IMMUNE-MEDIATED ACQUIRED HEMOLYTIC ANEMIA • Occurs when antibodies are made against a patient’s own RBCs • Primary vs. Secondary (common= viral, pregnancy) • Warm vs. Cold vs. Mixed • Alloimmune – e. g. Rh(D) neg pregnant females • Drug-Induced

QUIZ

IMMUNE-MEDIATED ACQUIRED HEMOLYTIC ANEMIA • Treatment: Treatment of Underlying Cause; High Dose Corticosteroids 1 -2 mg/kg, Monclonal Abx (rituxima), Immunosuppressives (e. g. cyclosporine), semisynthetic androgens (danazol), splenectomy; PRBC transfusions with careful screening of antibodies • Rhogam for Rh(D)- after maternal bleeding/hemorrhage

ACQUIRED HEMOLYTIC ANEMIA • Immune Mediated • Microangiopathic Syndromes • Macrovascular Hemolysis

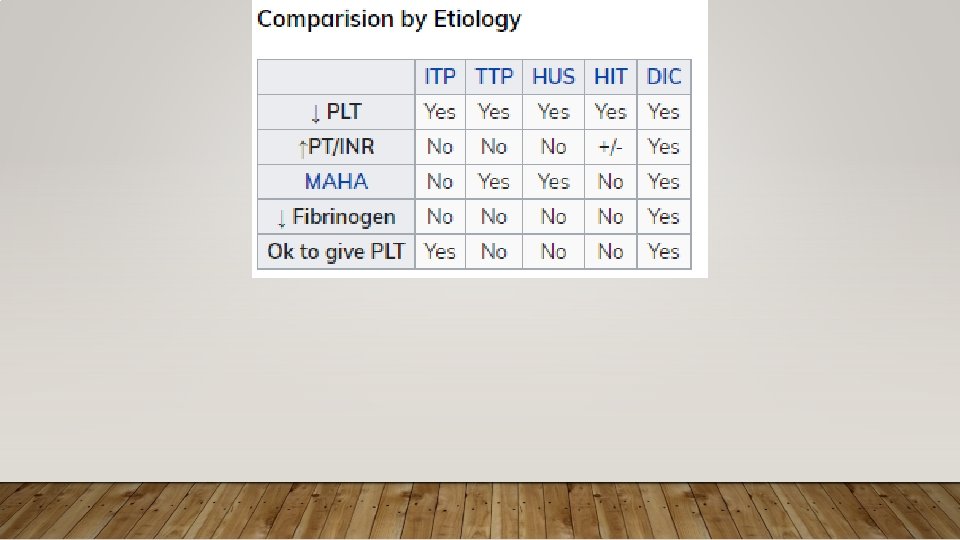
MICROANGIOPATHIC HEMOLYTIC ANEMIA • TTP • HUS • Characteristics of Both • v. WF mediated platelet aggregation, schistocyte forming hemolysis

 of ADAMTS-13 results increase in v.")
THROMBOTIC THROMBOCYTOPENIC PURPURA • Pathophys: Low levels (<10%) of ADAMTS-13 results increase in v. WF activity, leading to intravascular microthrombi • Common Precipitating Causes: Pregnancy (hard to distinguish from HELLP), HIV, Influenza vaccination, drugs • Clinical Features: MAHA, thrombocytopenia (<20 k), AMS, fever, renal dysfunction Normal coags (DIC = abnl coags, fibrinogen)

QUIZ

QUIZ • ADAMTS-13 = a disinterin and metalloproteinase with a thrombospondin type 1 motif, member 13 • Aka v. WF cleaving protease

THROMBOTIC THROMBOCYTOPENIC PURPURA • Treatment: identify underlying cause; Plasma Exchange (removal/replacement of defective or insufficient ADAMTS-13, autobodies, and large v. WF multimers); in the interim = FFP, Corticosteroids/Rituximab/Cyclosporine, • +/- Aspirin for CVA/MI if nl platelets • ******Avoid platelet transfusion*******
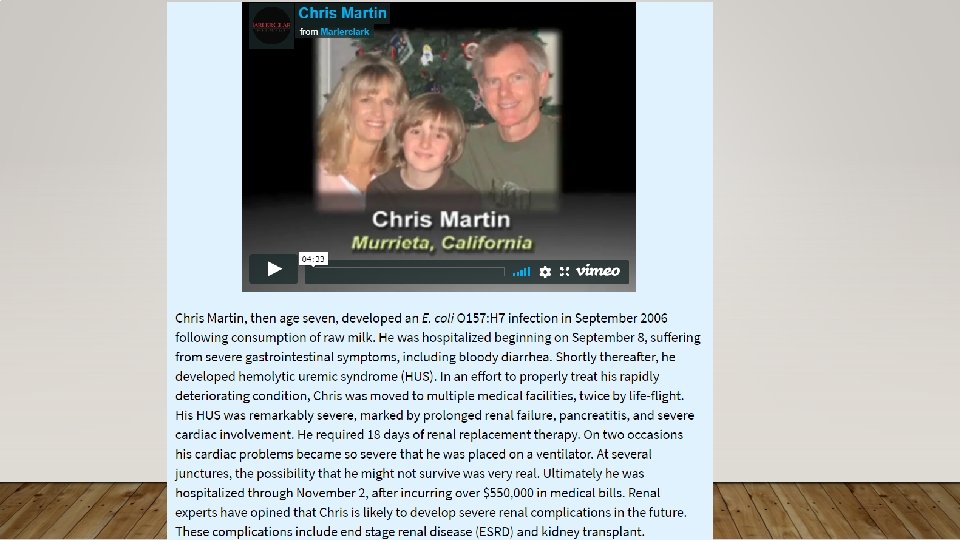

HUS • Pathophys: shiga toxin-producing E. coli O 157: H 7 from uncooked meats, spinach, cookie, dough, unpasteurized milk causing infectious diarrhea • Typically children • Toxin-mediated microvascular injury promotes platelet aggregation, thrombus formation at injury site, platelet consumption • Clinical Features: abdominal cramps, diarrhea +/- bloody, +/- fever, renal dysfunction, MAHA, thrombocytopenia • Treatment: supportive care, hydration, analgesics, RBCs for severe anemia, hemodialysis for severe renal failure • Platelets? , Antibiotics? ; Eculizumab

ACQUIRED HEMOLYTIC ANEMIA • Immune Mediated • Microangiopathic Syndromes • Macrovascular Hemolysis

MACROVASCULAR HEMOLYTIC ANEMIA • Prosthetic Heart Valve • Intracardiac Patch Repair • Aortofemoral Bypass • Coarctation of the Aorta • Severe Aortic Valve Disease • Ventricular Assist Device • Extracoporal Therapy: Bypass, Plasma Exchange, HD

CLOTTING DISORDERS

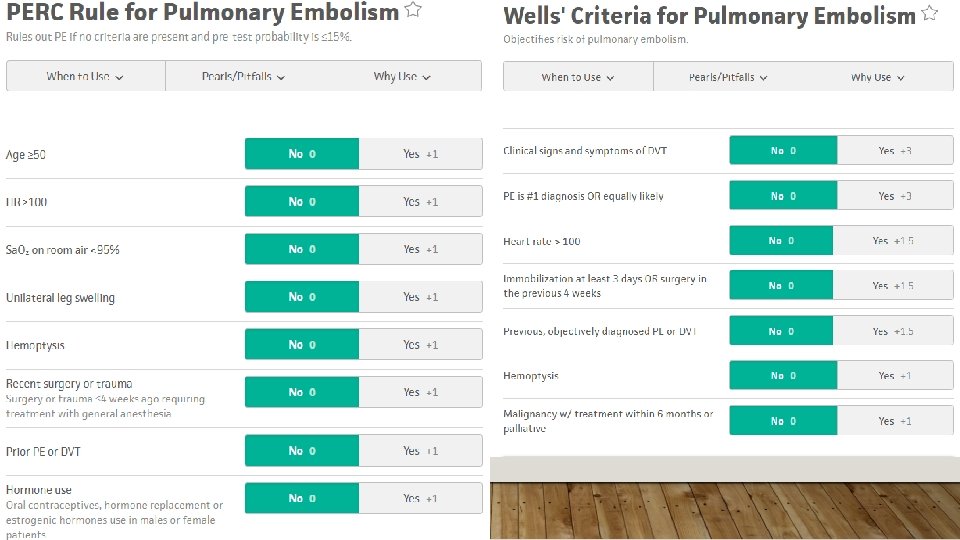
BIGGEST TAKEAWAY Doesn’t matter that the Wells is 0, these patients need to be considered for VTE

CLOTTING DISORDERS • General Approach • Specific Conditions • Inherited • Acquired

CLOTTING DISORDERS • General Approach • Specific Conditions • Inherited • Acquired

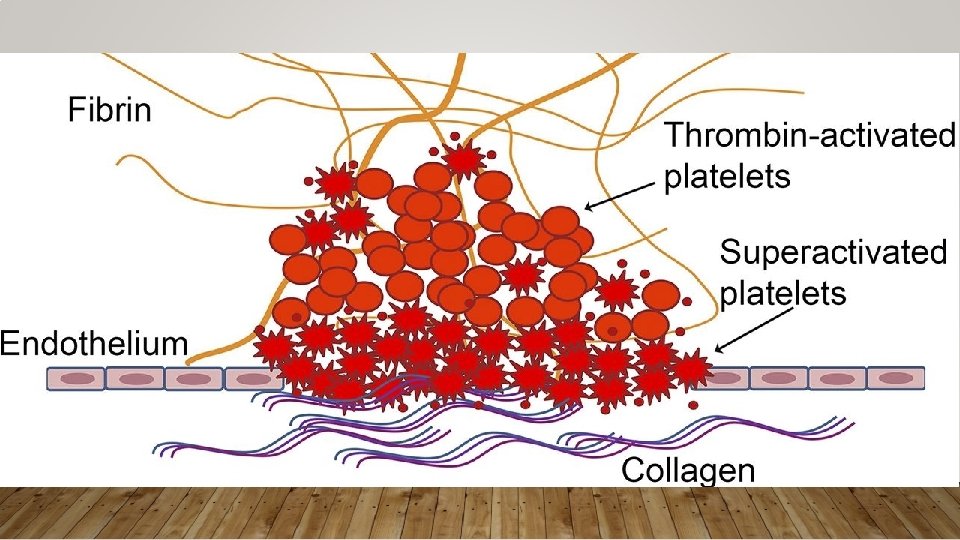
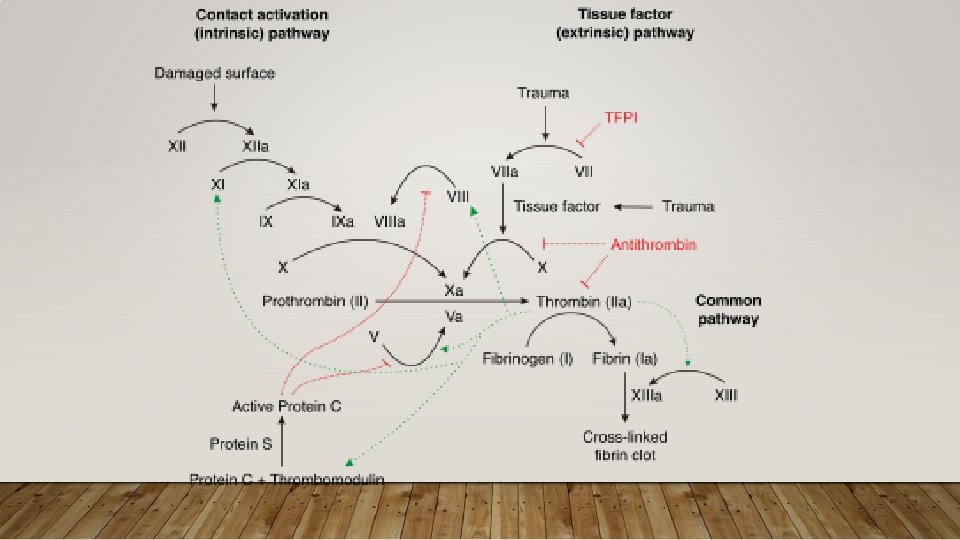
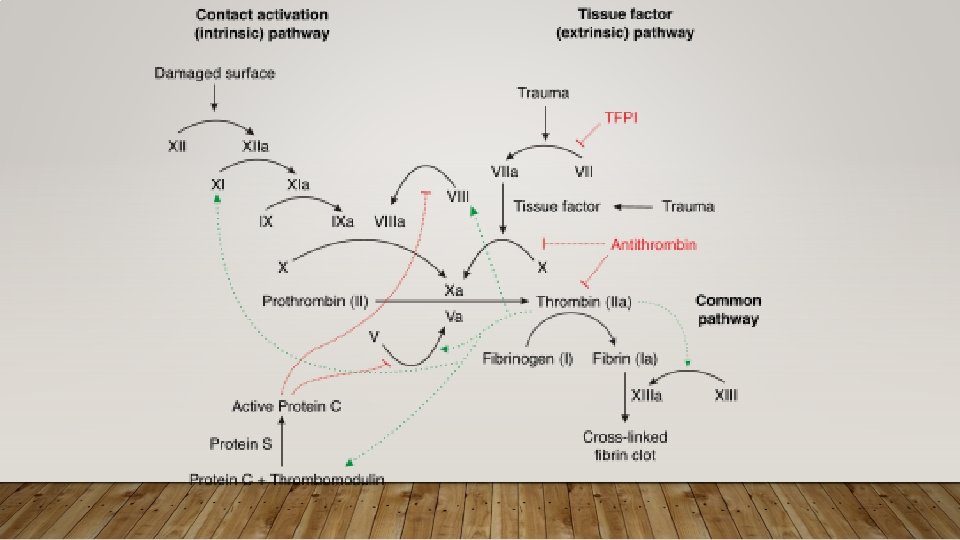
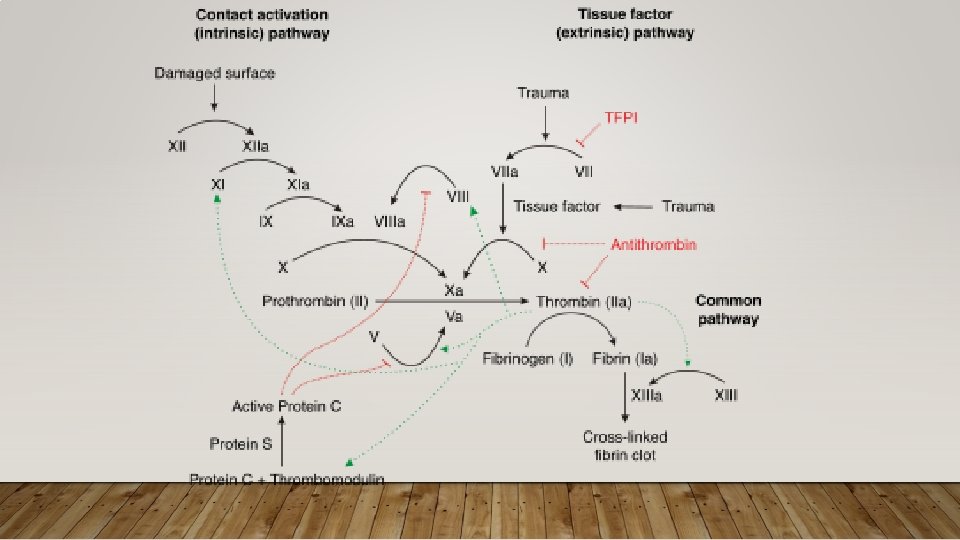
APPROACH TO CLOTTING CONDITIONS • Pathophys: Key pathways • Antithrombin – promotes anticoagulation by inhibiting several coagulation factors; its activity is increased by Heparin, LMWH • Protein C – cleaves factors in common and intrinsic pathway; is Vit K dependent • Protein S – cofactor, of Protein C • Diagnostics: Typically do not make diagnosis of thrombophilia in ED • Make diagnosis of acute thrombosis, refer if suspected thrombophilia • Treatment:
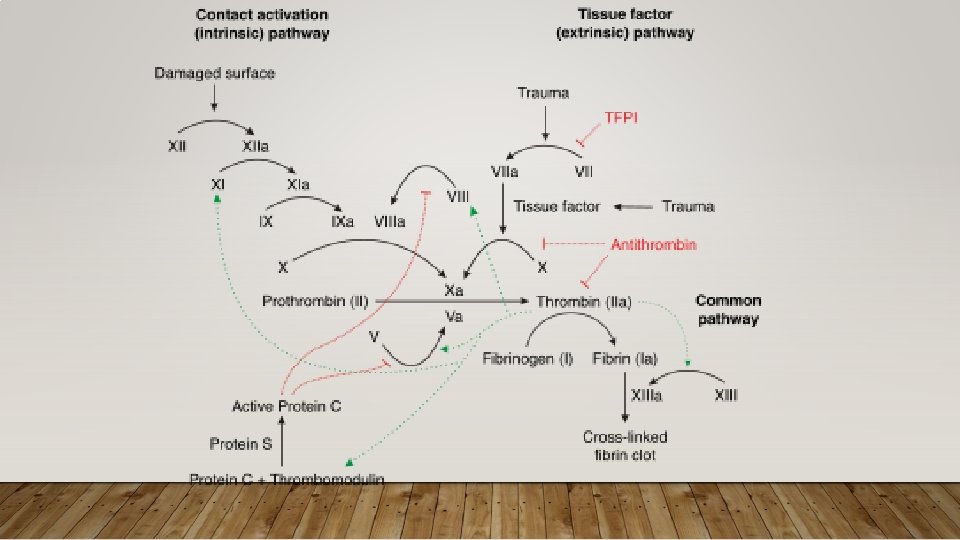

APPROACH TO CLOTTING CONDITIONS • Pathophys: Key pathways • Antithrombin – promotes anticoagulation by inhibiting several coagulation factors; its activity is increased by Heparin, LMWH • Protein C – cleaves factors in common and intrinsic pathway; is Vit K dependent • Protein S – cofactor, of Protein C • Diagnostics: Typically do not make diagnosis of thrombophilia in ED • Make diagnosis of acute thrombosis, refer if suspected thrombophilia • Treatment:

CLOTTING DISORDERS • General Approach • Specific Conditions • Inherited • Acquired
 • Prothrombin Gene")
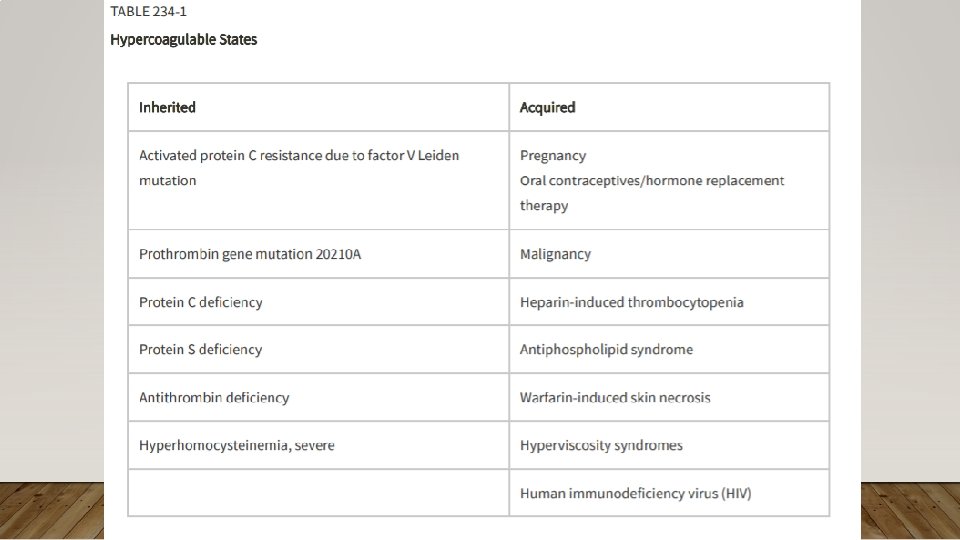
INHERITED CLOTTING DISORDERS • Factor V Leiden (Activated Protein C resistance) • Prothrombin Gene Mutation • Antithrombin Deficiency • Protein C and S Deficiencies • Hyperhomocysteinemia

FACTOR V LEIDEN • Most prevalent inherited hypercoagulable disorder 5% US/European • Resistant to Activated Protein C, leads to increased conversion of prothrombin to thrombin • ** x 7 risk of DVT/PE, accounts for 21% of first time DVTs** • Associated with pregnancy complications: severe pre-eclampsia, placental abruption, fetal growth restriction, stillbirth
 • Prothrombin Gene")
INHERITED CLOTTING DISORDERS • Factor V Leiden (Activated Protein C resistance) • Prothrombin Gene Mutation • Antithrombin Deficiency • Protein C and S Deficiencies – at risk of warfarin skin necrosis • Hyperhomocysteinemia
 • Prothrombin Gene")
INHERITED CLOTTING DISORDERS • Factor V Leiden (Activated Protein C resistance) • Prothrombin Gene Mutation • Antithrombin Deficiency • Protein C and S Deficiencies • Hyperhomocysteinemia – associated with skeletal, ocular problems, developmental delays

CLOTTING DISORDERS • General Approach • Specific Conditions • Inherited • Acquired

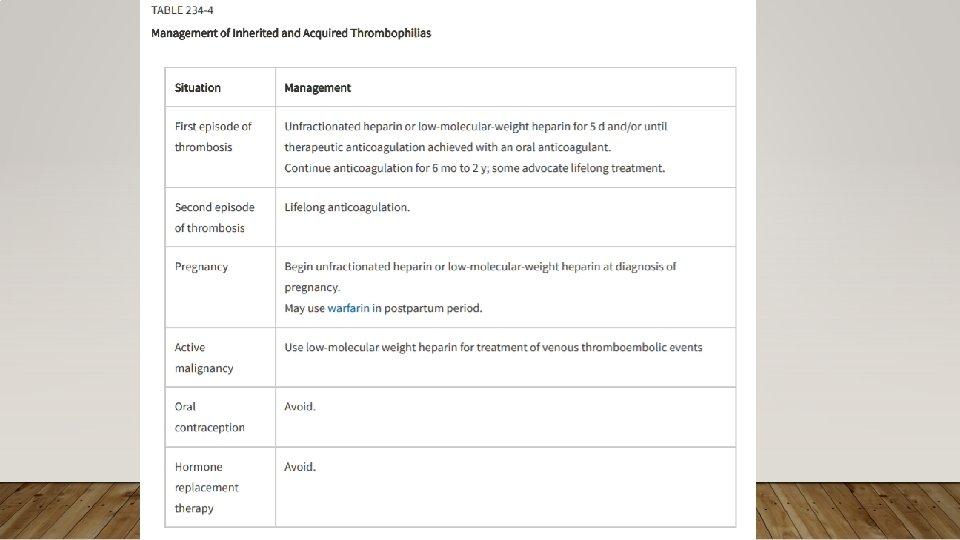
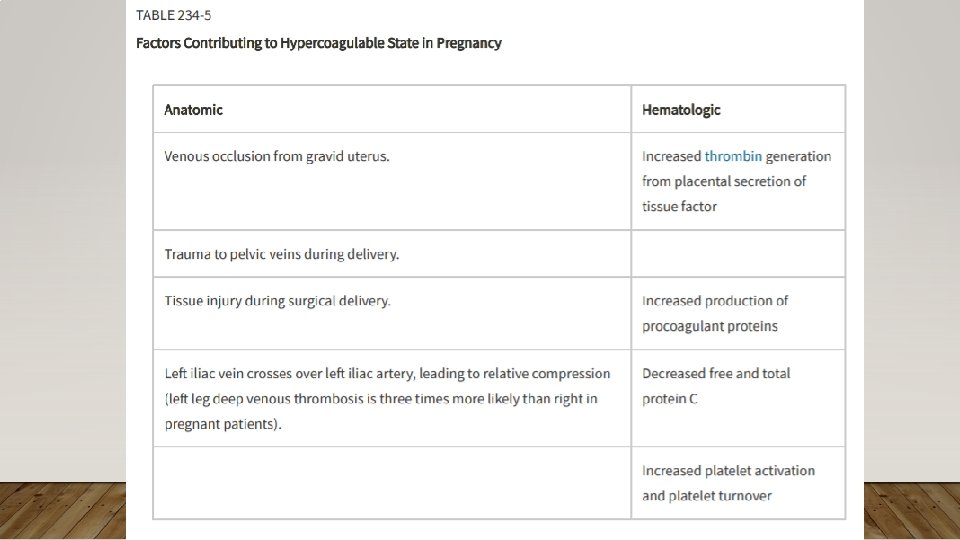
ACQUIRED CLOTTING DISORDERS • Pregnancy and Estrogen Use • Malignancy • Heparin-Induced Thrombocytopenia • Warfarin-Induced Skin Necrosis • Antiphospholipid Syndrome

ACQUIRED CLOTTING DISORDERS • Pregnancy and Estrogen Use • Malignancy • Heparin-Induced Thrombocytopenia • Warfarin-Induced Skin Necrosis • Antiphospholipid Syndrome

QUIZ

• Treatment of choice for VTE in Malignancy = LMWH

ACQUIRED CLOTTING DISORDERS • Pregnancy and Estrogen Use • Malignancy – more likely types: pancreatic, brain, AML, gastric, esophageal, gynecologic, kidney, lung • Chemo can also worsen (down regulate protein C/S, tissue factor production, cell damage) LMWH x 6 months • Heparin-Induced Thrombocytopenia • Warfarin-Induced Skin Necrosis • Antiphospholipid Syndrome

ACQUIRED CLOTTING DISORDERS • Pregnancy and Estrogen Use • Malignancy • Heparin-Induced Thrombocytopenia – consumptive coagulopathy, inappropriate activation of clotting cascade components leading to platelet activation and arterial/venous thrombus • Plts 50 -60 K (or drop 50% baseline value) within 5 -15 d after starting heparin • Treatment: stop heparin/LMWH, avoid Vit K antagonist (Warfarin), start AC with direct thrombin inhibitors (Lepirudin [unless renal failure], Argatroban [unless liver disease], Bivalirudin) or direct Xa inhibitor (Fondaparinux, Danaparoid) • Warfarin-Induced Skin Necrosis • Antiphospholipid Syndrome

ACQUIRED CLOTTING DISORDERS • Pregnancy and Estrogen Use • Malignancy • Heparin-Induced Thrombocytopenia • Warfarin-Induced Skin Necrosis – due to Protein C reduction first and hypercoagulopathy • Painful red lesions over extremities, breasts, trunk, penis • Antiphospholipid Syndrome


ACQUIRED CLOTTING DISORDERS • Pregnancy and Estrogen Use • Malignancy • Heparin-Induced Thrombocytopenia • Warfarin-Induced Skin Necrosis • Antiphospholipid Syndrome – antibodies not just against phospholipids but proteins that interact with phospholipids (i. e. Protein C/S); abs = B 2 glycoprotein and lupus anticoagulant (due to prolonged PTT, is actually pro-thrombotic) • Catastrophic APS – accelerated, widespread small-vessel occlusion in mutiple organs • Treatment: lifelong AC, if pregnant than Heparin/LMWH; for Catastrophic APS AC, steroids, plasmapheresis, IVIG

HYPERCOAGULABILITY ASSOCIATED WITH OTHER DISORDERS • Nephrotic Syndrome • Vasculitis • Hyperviscositiy Syndrome –thrombocythemia, polycythemia, macroglobinemia, mutltiple myelome, sickle cell disease • Diabetes • Smoking • HIV

THROMBOTICS AND ANTITHROMBOTICS

BIGGEST TAKEAWAY Be ready to throw the kitchen sink (and know what the kitchen sink is)

THROMBOTICS AND ANTITHROMBOTICS • Anticoagulants • Antiplatelets • Fibrinolytics/Anti-fibrinolytics

THROMBOTICS AND ANTITHROMBOTICS • Anticoagulants • Antiplatelets • Fibrinolytics/Anti-fibrinolytics

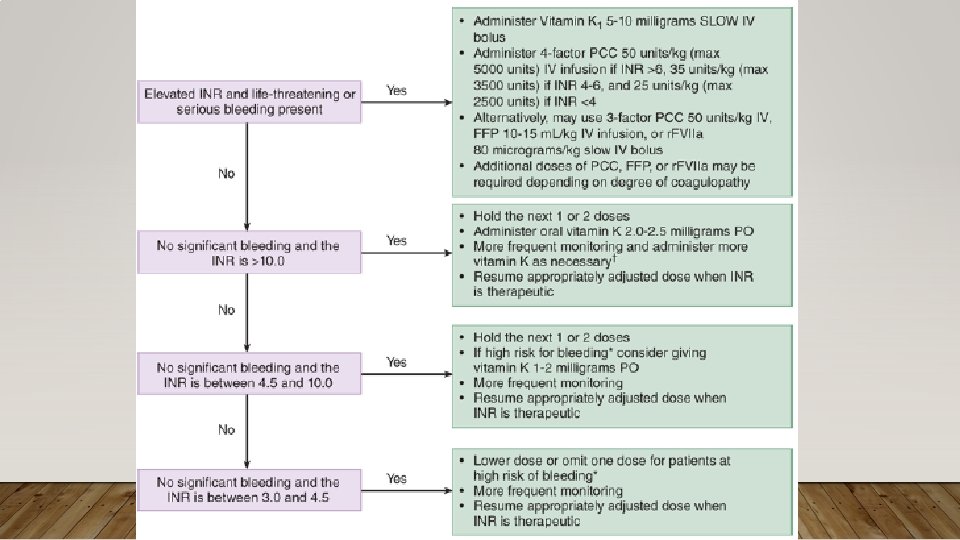
WAFARIN/COUMADIN • Vitamin K Antagonist, affects extrinsic and common pathway • 4 Key Points • 1) Has pro-thrombotic effects (via Protein C/S) • 2) Has many drug-drug interactions • 3) Always look up reversal guidelines when overdosed or serious bleeding • 4) Caution over-correcting prosthetic valve replacement

WAFARIN/COUMADIN • Vitamin K Antagonist, affects extrinsic and common pathway • 4 Key Points • 1) Has pro-thrombotic effects (via Protein C/S) • 2) Has many drug-drug interactions • 3) Always look up reversal guidelines when overdosed or serious bleeding • 4) Caution over-correcting prosthetic valve replacement

WAFARIN/COUMADIN • Vitamin K Antagonist, affects extrinsic and common pathway • 4 Key Points • 1) Has pro-thrombotic effects (via Protein C/S) • 2) Has many drug-drug interactions • 3) Always look up reversal guidelines when overdosed or serious bleeding • 4) Caution over-correcting prosthetic valve replacement

WAFARIN/COUMADIN • Vitamin K Antagonist, affects extrinsic and common pathway • 4 Key Points • 1) Has pro-thrombotic effects (via Protein C/S) • 2) Has many drug-drug interactions • 3) Always look up reversal guidelines when overdosed or serious bleeding • 4) Caution over-correcting prosthetic valve replacement

WAFARIN/COUMADIN • Vitamin K Antagonist, affects extrinsic and common pathway • 4 Key Points • 1) Has pro-thrombotic effects (via Protein C/S) • 2) Has many drug-drug interactions • 3) Always look up reversal guidelines when overdosed or serious bleeding • 4) Caution over-correcting prosthetic valve replacement

QUIZ

• AB+ is the universal donor for FFP • Has no antibodies against AB type

OTHER ORAL ANTICOAGULANTS • Direct Thrombin Inhibitors • Dabigatran • Factor Xa Inhibitors • Rivaroxaban, apixaban, etc Hemodialysis can help remove for overdoses

HEPARIN AND POLYSACCHARIDES • Can be UFH and LMWH • Binds to anti-thrombin • Effects extrinsinic and common pathways via thrombin ans FXa • Assess via a. PTT • Fondaparinux • Another polysaccharide AC that effects anti-thrombin (effects Fxa but not thrombin) • Complications/Reversal Heparin • HIT • Bleeding Reversal Agent: Protamine (reserved for major bleeding due to side effects)

HEPARIN AND POLYSACCHARIDES • Can be UFH and LMWH • Binds to anti-thrombin • Effects extrinsinic and common pathways via thrombin ans FXa • Assess via a. PTT • Fondaparinux • Another polysaccharide AC that effects anti-thrombin • Complications/Reversal Heparin • HIT • Bleeding Reversal Agent: Protamine (reserved for major bleeding due to side effects)

OTHER ANTICOAGULANTS – HIRUDIN/ANALOGUES • Hirudins • Hirudin, Lepirudin • Hirudin Analogues • Bivalirudin, Argatroban • Parenteral Direct Thrombin Inhibitors • Advantages over heparin – inhibits both cloth and circulating thrombin, doesn’t inhibit other coagulation pathways or fibrinolytic enzyms, doesn’t require Antithrombin cofactor, doesn’t interact with platelet factor 4

ACQUIRED CLOTTING DISORDERS • Pregnancy and Estrogen Use • Malignancy • Heparin-Induced Thrombocytopenia – consumptive coagulopathy, inappropriate activation of clotting cascade components leading to platelet activation and arterial/venous thrombus • Plts 50 -60 K (or drop 50% baseline value) within 5 -15 d after starting heparin • Treatment: stop heparin/LMWH, avoid Vit K antagonist (Warfarin), start AC with direct thrombin inhibitors (Lepirudin [unless renal failure], Argatroban [unless liver disease], Bivalirudin) or direct Xa inhibitor (Fondaparinux, Danaparoid) • Warfarin-Induced Skin Necrosis • Antiphospholipid Syndrome

THROMBOTICS AND ANTITHROMBOTICS • Anticoagulants • Antiplatelets – covered last week • ASA • Adenosine Diphosphate Receptor Agents (Clopidogrel, Prasugrel, Ticagrelor, Ticlopidine) • Phosphodiesterase Inhibitors (Dipyridamlole) • Glycoprotein Iib/IIIa Antagonist (Abciximab, Eptifibatide, Tirofiban) • Fibrinolytics/Anti-fibrinolytics

QUIZ

• Tissue Plasminogen Activator

THROMBOTICS AND ANTITHROMBOTICS • Anticoagulants • Antiplatelets • Fibrinolytics/Anti-fibrinolytics

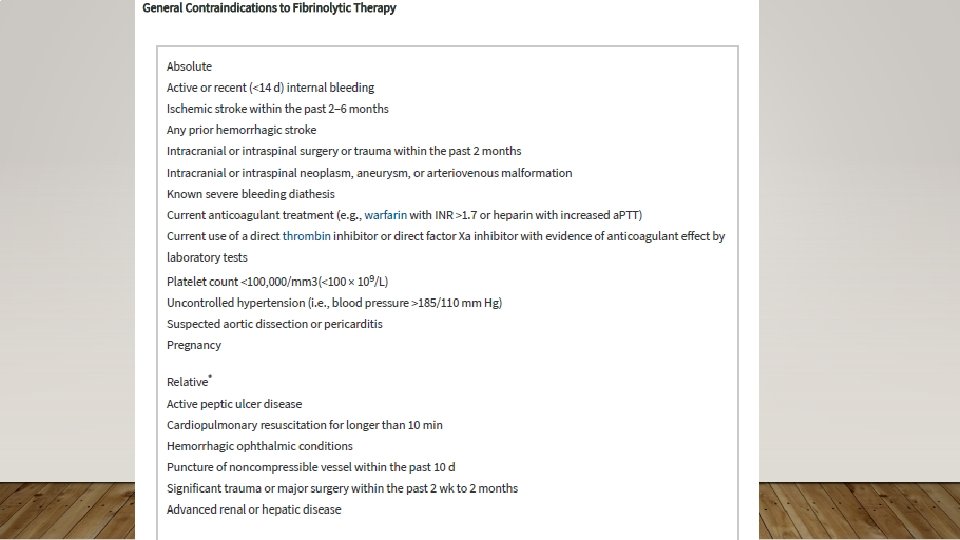
FIBRINOLYTICS • 1 st Generation – Streptokinase, Anistreplase • 2 nd Generation – Alteplase (TPA) Fewer allergic reactions • 3 rd Generation – Reteplase, Tenecteplase not infusion Can be given as just boluses, • Promotes conversion of plasminogen to plasmin which attacks fibrin • Indications: • You can (and should) look up contraindications
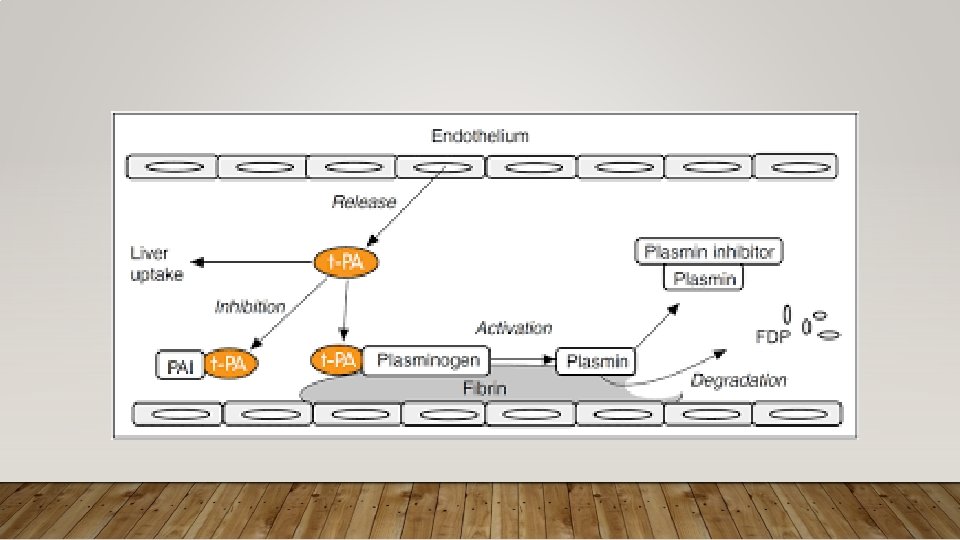

FIBRINOLYTICS • 1 st Generation – Streptokinase, Anistreplase • 2 nd Generation – Alteplase (TPA) Fewer allergic reactions • 3 rd Generation – Reteplase, Tenecteplase not infusion Can be given as just boluses, • Promotes conversion of plasminogen to plasmin which attacks fibrin • Indications: • You can (and should) look up contraindications

FIBRINOLYTICS - WHOOPSIES • Allergic Reaction – standard treatments: antihistamines, steroids, IM epi, etc. • Massive Bleeding – empiric coagulation factor replacement with Cryoprecipitate (rich fibrinogen), FFP, Antifibrinolytics, +/- Platelets, +/- Protamine
 and Aminocaproic Acid (ACA) • More oftenly used in")
ANTIFIBRINOLYTICS • Tranexamic Acid (TXA) and Aminocaproic Acid (ACA) • More oftenly used in ED after CRASH-2 Study 2011 for trauma • Other (potential) uses: postpartum hemorrhage, hemoptysis, UGIB, nasal bleeding, dental bleeding (hemophilia), traumatic hyphema, heavy menstrual bleeding, ? ICH • Potential cause for vascular thrombosis

EMERGENCY COMPLICATION OF MALIGNANCY

BIGGEST TAKEAWAY Always find out if they are on chemo
 • On")
EMERGENCY COMPLICATION OF MALIGNANCY • With or Without Chemo (Mass Effect, Coagulopathy) • On Chemo
 • On")
EMERGENCY COMPLICATION OF MALIGNANCY • With or Without Chemo (Mass Effect, Coagulopathy) • On Chemo

MASS EFFECT • Malignant Airway Obstruction • Bone Metastases, Pathologic Fractures • Pericardial Effusion with Tamponade • SVC Syndrome • Malignant Spinal Cord Compression • Up to 20% of all CA patients, 3 -6% will develop spinal cord compression • Most from solid organ tumors • 10% do not have back pain; 20% do not have prior diagnosis of CA • MRI – imaging modality of choice, consider imaging entire spine; alternative = CT +/Myelography • Treatment: Steroids, Radiotherapy
 • On")
EMERGENCY COMPLICATION OF MALIGNANCY • With or Without Chemo (Mass Effect, Coagulopathy) • On Chemo

QUIZ

BIOCHEMICAL DERANGEMENTS • Tumor Lysis Syndrome • Massive cytolysis from chemo • Leads to increased K, P, Uric Acid; binding) • AKI, arrhythmias, seizures • Adrenal Insufficiency • Hyponatremia (SIADH) • Hypercalcemia Ca released (but you see Hypo. Ca due to Ca-Phos

BIOCHEMICAL DERANGEMENTS • Tumor Lysis Syndrome • Massive cytolysis from chemo • Leads to increased K, P, Uric Acid; binding) • AKI, arrhythmias, seizures • Adrenal Insufficiency • Hyponatremia (SIADH) • Hypercalcemia Ca released (but you see Hypo. Ca due to Ca-Phos

HEMATOLOGIC DERANGEMENT • Febrile Neutropenia and Infection • Avoid DRE • Evaluate Chemoport, Tunneled Catheters for infection • Empiric Abx when ANC <500 • Hyperviscosity Syndrome • Thromboembolism

HEMATOLOGIC DERANGEMENT • Febrile Neutropenia and Infection • Hyperviscosity Syndrome • Waldenstrom Macroglobulinemia, Immuno. Globinulin A, Polycythemia • Roluleaux formation • Treatment: Intravascular volume repletion, Plasmapheresis/Leukapheresis, Phlebotomy + replacement crystalloids • Thromboembolism

QUIZ • Blood-letting

HEMATOLOGIC DERANGEMENT • Febrile Neutropenia and Infection • Hyperviscosity Syndrome • Thromboembolism • LMWH

SUMMARY OF BIGGEST TAKEWAYS • Acquired Hemolytic Anemias • If you can’t explain the anemia, consider hemolytic • Clotting Disorders • Doesn’t matter if the Wells Score is 0, these patients should be considered for VTE • Thrombotics and Antithrombotics • Be ready to throw the kitchen sink (and know what the kitchen sink is) • Emergency Complications of Malignancy • Always find out if they are on chemo

LAST ACTIVITY

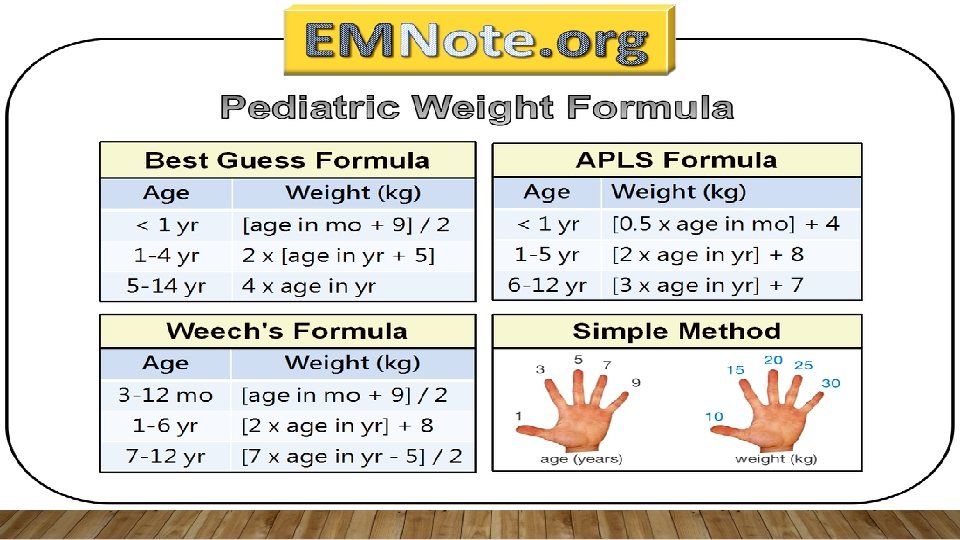
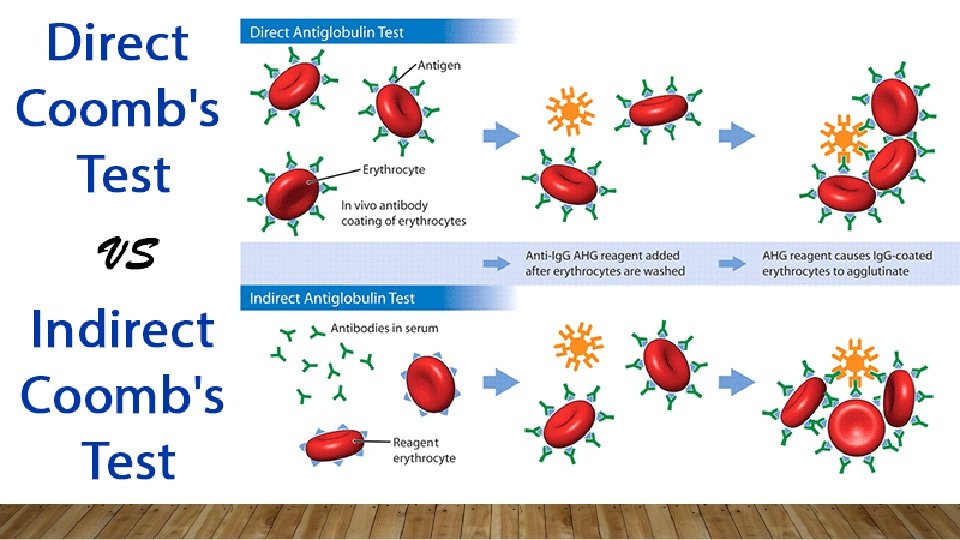
SUMMARY OF QUIZZES • Angicoagulation of Choice for Cancer? • LMWH • Emergent peds medication doses? • Epinephrine – 0. 01 mg/kg Atropine – 0. 02 mg/kg • Na Bicarb – 1 -2 m. Eq/kg D 50 Dextrose – 1 ml/kg of • Weight based dosing for PRBC transfusion? • 10 ml/kg • Tests that help diagnose hemolytic anemia? • Hgb/Hct, Retic Count, Potassium, LDH, Total & Indirect Bilirubin, Haptoglobin, Smear (Schistocytes, Spherocytes), UA (urobilinogen, hemoglobinuria), Indirect & Direct Coombs • What does ADAMTS-13 stand for? • a disinterin and metalloproteinase with a thrombospondin type 1 motif, member 13 • What is the universal donor type for FFP • AB+ • What does TPA stand for? • Tissue Plasminogen Activator • What electrolyte abnormalities would you see with tumor lysis syndrome? • Hyper. K, Hyper. P, Hyper. Uricemia • Hypo. Ca

RESOURCES
- Slides: 120