Heart failure Prepared by Maha islami Supervised by

Heart failure Prepared by: Maha islami. Supervised by : Majda Al-Attas.

outline v. Definition. v. Epidemiology. v. Etiology. v. Pathophysiology. v. Symptoms. v. Classification. v. Management.

Definition. Heart failure is defined as a syndrome in which the heart fails to pump sufficient blood to meet the needs of the body. Ejection fraction = % of the end-diastolic volume that is ejected during systole (normal > 50 % ).

Epidemiology • Heart failure is most commonly diagnosed at ages > 65 yo , more frequent in men than women. • Approximately 400, 000 new cases each year.

Etiology v Systolic Dysfunction : Ø Ischemic disease myocardial ischemia, and MI. Ø Non-Ischemic disease: I. 1 ry myocardial muscle dysfunction (idiopathic , drug induced , familial). II. Valvular abnormalities. III. Structural damage +/- damage to myocardial walls (e. g. ventricular septal defects). IV. Hypertension (pulmonary).

Etiology cont…. . v. Diastolic Dysfunction: ØHypertrophy cardiomyopathy. I. Hypertension. II. Myocardial Ischemia. Ø Restrictive cardiomyopathy. I. Amyloidosis. II. Sarcoidosis.

Other precipitating causes v. Infection: fever, tachycardia, hypoxemia, and increased metabolic demand place further strain on heart. v. Anemia: lack of oxygenating RBC demands heart to increase output-failing heart unable to do so. v. Pregnancy: for tissue to be adequately perfused, increased output is needed. v. Arrythmias: erratic cardiac output. v. Dietary , and emotional excesses.
. v.")
Drugs that may exacerbate HF. v. Negative inotropic effect: - anti-arrythmics, CCB (non-DHP). v. Cardiotoxic : - Doxorubicin, cyclophosphamide. v. Na+/H 2 O retention: - Glucocorticoids, androgens, estrogens, NSAIDs.

pathophysiology

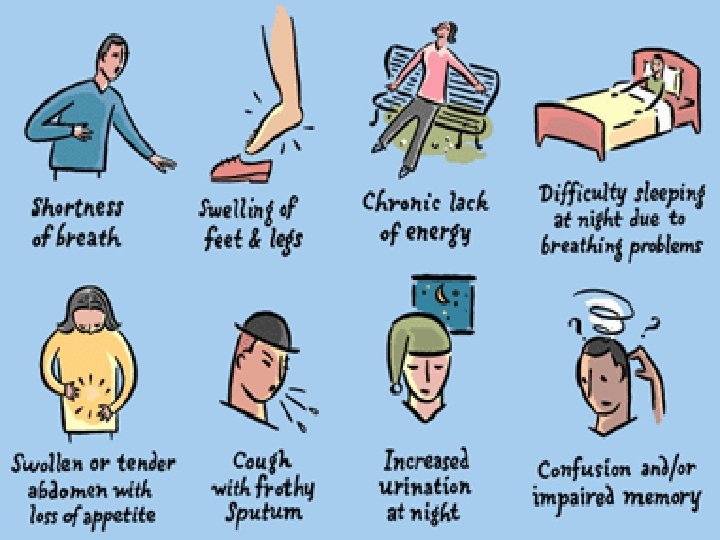
What Are The Symptoms of Heart Failure? v. Think FACES. . . • Fatigue. • Activities limited. • Chest congestion. • Edema or ankle swelling. • Shortness of breath.

Right-sided vs Left-sided HF. Right-sided Abd. pain, anorexia, nausea , constipation, peripheral edema, JVD, Hepatojugular reflex. Left-sided Dyspnea on exertion, Prenight dyspnea, orthopnea, cough, pulmonary edema, pleural effusion, (+) S 3 Gallop. Fatigue, Weakness, Cardiomegaly, Pallor. Non-specific symptoms

HF Classification system v. New York Heart Association Functional classification: - Class I: NO Limitation of physical activity. - Class II: ordinary activity result in symptoms of HF. - Class III: marked limitation of physical activity. - Class IV: symptoms of HF at rest.

Stages of HF based on evolution and progression of clinical findings. stage description examples A Pts at ↑risk of developing HF because of the presence of conditions that are strongly associated with the development of HF. such pts have no identified structural abnormalities and have never shown signs or symptoms of HF. HTN, CAD, DM, Hx of cardiotoxic drug therapy, Hx of rheumatic fever, family Hx of cardiomyopathy. B Pts who have developed structural heart disease that is strongly associated with the development of HF but who have never shown signs or symptoms of HF. Left ventricular hypertrophy or fibrosis, left ventricular dilation or hypocontractility, asymptomatic valvular heart disease, previous myocardial infarction.

Stages of HF based on evolution and progression of clinical findings cont… stage description Examples C pts who have current symptoms of HF associated with underlying structural heart disease, Dyspnea or fatigue duo to left ventricular systolic dysfunction. D Pts with advanced structural heart disease and marked symptoms of HF at rest despite maximal medical therapy and who require specialized interventions. Pts who are frequently hospitalized for HF and cannot be safely discharged from the hospital receiving continuous IV support for symptom relief or being supported with a mechanical circulatory assist device.

Evaluation of HF A. Assign stage of HF based on evaluation and progression of clinical finding( Guidelines ). B. Obtain LVEF and dimensional echocardiogram. C. Ventricular hypertrophy and chest congestion can be provided by chest X-ray(cardiomegaly, plural effusion). D. ECG. E. Liver enzyme elevation (hepatomegaly). F. Assess fluid status: -weight. -peripheral edema. -JVD. -hepato/splenomegaly. - Rales.

Management of HF v. Non-pharmacologic /Adjunct therapy. 1. Minimize sodium intake (< 3 gm daily). 2. Weight loss. 3. Smoking cessation. 4. A form of exercise. 5. Surgical : correction of valvular disease, revascularization, heart transplant. 6. Avoid NSAIDs.

Management of HF cont…. v. Pharmacological treatment: ü Most pts with symptomatic should be managed with combination of 4 types of drugs: - ACEI +B-B(improve EF duo to effecting remodling)+ Diuretics, +/- Digitals. (basic core ). ü Hydralazine and isosorbide for pt who can’t take ACEI. ü Oxygination. ü Anticoagulation: is not recommended only in HF pts at risk with : AF, DVT, PE, and EF≤ 25% may give Warfarin.

Management of HF cont…. üAnti-arrhythmic: is the mode of death in up to 50% of HF cases. class 1 antiarrhythmic not recommended. (Amiodarone 1 st line agent and Dofetilide appear to be safe , does not appear to increase mortality.

HF Treatment options v. ACEI: Ø ↓Preload and afterload, and ↑CO. Ø 1 st line agents in the Tx. Showing a beneficial effect on cardiac remodeling. Ø Start at low dose and titrate , dose can be ↑q 3 -7 days. Ø Elderly pts >75 YO should start ½ recommended starting dose.

ACEI cont…. . Ø Dose: drug §Captopril. §enalapril. §Cilazapril. Starting dose 6. 25 -12. 5 mg tid. 2. 5 -5 mg qd. 0. 5 mg bid. Target dose 50 mg tid. 10 mg bid. 1 -2. 5 mg bid. Max dose 100 mg tid. 20 mg bid. 5 mg bid. ØSE: Dry cough, angioedema, neutropenia, skin rash, proteinuria, hyperkalemia.

HF Treatment options cont…. v. B-B: Ø ↓sympathetic stimulation by ↓plasma NE peripheral vasoconstriction and cell death (apoptosis). Ø Dose: drug Initial dose Target dose Bisoprolol. 1. 25 mg once daily. 10 mg once daily. Carvidolol. 3. 125 mg twice daily. 25 mg twice daily , 50 mg twice daily for pts >85 kg.

HF Treatment options cont…. Ø SE: depression , nightmares , insomnia , bronchospasm , dizziness. v. Diuretics: Ø ↓edema and congestion (↓preload). Ø IV for pulmonary edema. Ø Oral doses are titrated according to symp and body wt. Ø Thiazid are weak diuretics and are used infrequently in HF.
most widely used. Ø Dose: drug Starting dose Max")
Diuretics cont…. Ø Loop diuretics (furosemide)most widely used. Ø Dose: drug Starting dose Max dose furosemide 20 -40 mg qd. 240 mg bid. HCTZ 25 mg qd. 50 mg qd. Metalazone 2. 5 mg qd. 10 mg qd. Ø SE: ↓K , ↓Mg , DM , HA , jundice , arrythmia.
inotrope , ↑CO , May")
HF Treatment options cont…. v digoxin: Ø (+ ve )inotrope , ↑CO , May have beneficial effect on vagal tone and ↓SNS. Ø Used as second line therapy in pt not responding to conventional therapy. Ø Dose: initial dose 0. 125 -0. 25 mg once daily. Ø Target dose : 0. 125 -0. 25 mg once daily. Ø Digitalis Toxicity: Symptoms of toxicity: nausea , vomiting , headache , dizziness , chills , fever, diarrhea , restlessness.

Digitalis Toxicity cont…. § Treatment of the toxicity : 1. Hold the medications. 2. Observation. 3. In case of A/V block or severe bradycardia → atropine followed by temporary PM if needed. 4. In life threatening arrhythmia → digoxinspecific fab antibodies. 5. Lidocaine and phenytoin could be used.

HF Treatment options cont…. v. CCB: Ø Possible ↓in afterload. Ø Amlodipine and Felodipine may have some benefit in HF Pts with angina or HTN. v. Hydralazine and nitrates combination: Ø Hydralazine : ↓afterload. Ø Nitrates: ↓ preload. Ø This combination the 1 st to ↑survival in sever HF. Ø 1 st Tx in mild-moderate systolic HF.

Hydralazine and Nitrates combination cont …. Ø Not studied diastolic HF. Ø Dose: drug Starting dose Hydralazin and 10 mg tid. Isosorbide dinitrate 10 mg tid. Target dose 75 mg tid-qid. 40 mg tid-qid. Ø SE: Postural hypotension , sever HA , flushing , SLE.

HF Treatment options cont…. v. Spironolactone: Ø Block aldosterone chronically. Ø Consider in pts with recent or current class IV symptoms. Ø Dose: Drug Starting dose spironolactone 25 mg qd. Target dose 25 -5 o mg qd. Ø SE: Gynecomastia , agranulocytosis , N/V , Hyperkalemia. Max dose 100 mg.

Stage A Stage B Stage C Stage D High risk of developing HF but no structural heart disease or symptoms of HF Structural heart disease but without symptoms of HF. Structural heart disease with prior or current symptoms of HF. Therapy Treat HTN , encourage smoking cessation , treat lipid disorders , encourage regular exercise, v. ACEI in appropriate pts. All measures under stage A. v. ACEI in appropriate pts. v. B-adrenergic blockers in appropriate pts. All measures under stage A. Drugs for routine use: v. Diuretics. v. ACEI. v. B-B. v+/-Digitalis. All measures under stages A, B, and C. v. Mechanical assist devices. v. Heart transplantation. v. Continuous IV inotropic infusions. Refractory HF requiring specialized interventions.

New Methods: v. Implantable ventricular assist devices.
.")
New Methods cont… • Biventricular pacing (only in patient with left bundle branch block).

References. • http: //www. nlm. nih. gov/mdlineplus/heartfailur e. htm. • http: //www. emedicinehealth. com/congestive_ heart_failure/article_em. htm.

Thank you
- Slides: 35