Heart Failure Management From the Emergency Department to


 patients by their clinical profiles and phenotypes")









 ◆Tachypnea ◆Tachycardia ◆Altered")



 Hypertensive AHF ACS and HF Pulmonary edema Cardiogenic shock")
 Sensitivity Specificity")







 Cutoff")
 ◆Higher")


: 1861")






 – Typical infusion range: 10 -20 mcg/min (waste of time) –")
 push is not enough – author")






 – Improve symptoms – Balance")




: 24 -37.")


- Slides: 54
Heart Failure Management: From the Emergency Department to Hospital Admission and Discharge Provided by In collaboration with Support made possible through an educational grant from Novartis Pharmaceuticals Corporation
Faculty Co-Chairs Muhammad Waqas Athar, MD, MBBS Assistant Professor Johns Hopkins Bayview Medical Center Baltimore, MD Phillip D. Levy, MD, MPH Professor of Emergency Medicine Department of Emergency Medicine and Cardiovascular Research Institute Wayne State University School of Medicine Detroit, MI Presenting Faculty: Darren A. Manthey, MD Avera Medical Group Emergency Medicine Mitchell, SD Faculty disclosure information provided in handout.
Learning Objectives ◆ Identify heart failure (HF) patients by their clinical profiles and phenotypes and assess comorbid conditions ◆ Produce the diagnosis of acute heart failure (AHF) based on clinical presentation, history, laboratory assessment, and radiographic findings ◆ Integrate the data of related clinical trials and the evidence to support the use of current therapies as well as novel therapies that are in development for AHF ◆ Collaborate with the interdisciplinary team to properly assess when HF patients need to be admitted to the hospital, placed in observation status, or discharged ◆ Distinguish the importance of early re-initiation of guideline-directed medical therapy, including beta blockers, and discuss the initiation or continuation of newer FDA-approved treatments for patients admitted to the hospital or placed in observation status ◆ Describe evidence-based practices, including methods to improve care transitions for AHF patients once they are ready for discharge from the hospital
Introduction to the Epidemic
AHA Statistical Update—Heart Disease and Stroke Statistics 2014 Update ◆825, 000 new HF cases annually ◆At 40 years of age, the lifetime risk of developing HF for both men and women is 1 in 5 ◆The lifetime risk for people with BP >160/90 mm Hg is double that of those with BP <140/90 mm Hg AHA=American Heart Association. Go AS, et al. Circulation. 2014; 129(3): e 28 -e 292.
Median Survival A. Male 20 Years 16 US population Heart failure patients 15, 3 11, 8 12 8, 8 8 3, 8 4 2, 9 6, 4 2, 1 4, 7 1, 6 0, 9 0 B. Female 20 18, 6 14, 6 Years 15 11 8 10 5 4, 8 3, 5 2, 6 5, 6 2, 2 1, 5 0 65 -70 Ko DT, et al. Am Heart J. 2008; 155: 324 -331. 70 -75 75 -80 Age group 80 -85 85 -90
AHA Statistical Update—Heart Disease and Stroke Statistics 2014 Update Hospital discharges for heart failure by sex (United States: 1980 -2010) 700 Discharges in Thousands 600 500 Male Female 400 300 200 100 0 1985 Mozaffarian D, et al. Circulation. 2015; 131(4): e 29 -e 322. 1990 1995 Year 2000 2005 2010
Evaluating Acute Heart Failure Patients in the ED—Initial Approach
CHF ◆What are the chief complaints that make you think of CHF?
Chief Complaints ◆Shortness of Breath ◆Fatigue ◆Chest Pain ◆Palpitations ◆Weight gain ◆others: cough, dizzy, weakness
Causes of CHF ◆MI ◆HTN ◆Metabolic derangements/Dysrhythmias ◆Dietary indiscretion ◆Drugs/Meds ◆Myocarditis ◆Endocarditis/Valve abnormalities ◆Trauma: myocardial contusion
CHF: classification ◆Right Heart Failure ◆Peripheral edema ◆Fatigue ◆HTN ◆JVD ◆Orthopnea
CHF: classification ◆Left Sided Heart Failure ◆Pulmonary Edema ◆Hypertension ◆Hypotension (late/severe) ◆Tachypnea ◆Tachycardia ◆Altered Mental Status ◆Paroxysmal Nocturnal Dyspnea
CHF: classification ◆Systolic Heart Failure ◆Weak heart/weak squeeze ◆Less blood pumped out
CHF: classification ◆Diastolic Heart Failure ◆stiff heart ◆less blood fills the ventricles
CAUTION ◆GOING TO FOCUS MOSTLY ON LEFT SIDED HEART FAILURE LEADING TO PULMONARY EDEMA
Recognizing Acute Heart Failure (AHF) Hypertensive AHF ACS and HF Pulmonary edema Cardiogenic shock ACS=acute coronary syndrome. Pang PS, et al. Eur Heart J. 2010; 31: 784 -793. Acutely decompensated chronic HF Right HF
Is Clinical Examination Really Useful? Pooled Finding Summary Likelihood Ratio (95% CI) Sensitivity Specificity Positive Negative 0. 61 0. 86 4. 4 (1. 8 -10. 0) 0. 45 (0. 28 -0. 73) Third heart sound (ventricular filling gallop) 0. 13 0. 99 11 (4. 9 -25. 0) 0. 88 (0. 83 -0. 94) Abdominojugular reflux 0. 24 0. 96 6. 4 (0. 81 -51. 0) 0. 79 (0. 62 -1. 0) Jugular venous distension 0. 39 0. 92 5. 1 (3. 2 -7. 9) 0. 66 (0. 57 -0. 77) Rales 0. 60 0. 78 2. 8 (1. 9 -4. 1) 0. 51 (0. 37 -0. 70) Any murmur 0. 27 0. 90 2. 6 (1. 7 -4. 1) 0. 81 (0. 73 -0. 90) Lower-extremity edema 0. 50 0. 78 2. 3 (1. 5 -3. 7) 0. 64 (0. 47 -0. 87) Valsalva maneuver 0. 73 0. 65 2. 1 (1. 0 -4. 2) 0. 41 (0. 17 -1. 0) Systolic blood pressure <100 mm Hg 0. 06 0. 97 2. 0 (0. 60 -6. 6) 0. 97 (0. 91 -1. 0) Fourth heart sound (atrial gallop) 0. 05 0. 97 1. 6 (0. 47 -5. 5) 0. 98 (0. 93 -1. 0) Systolic blood pressure ≥ 150 mm Hg 0. 28 0. 73 1. 0 (0. 69 -1. 6) 0. 99 (0. 84 -1. 2) Wheezing 0. 22 0. 58 0. 52 (0. 38 -0. 71) 1. 3 (1. 1 -1. 7) Ascites 0. 01 0. 97 0. 33 (0. 04 -2. 9) 1. 0 (0. 99 -1. 1) Initial clinical judgment Physical examination Wang S, et al. JAMA. 2005; 294: 1944 -1956.
S 3 Heart Sound
Exam: ◆Vital signs ◆Frequently hypertensive ◆unless in cardiogenic shock ◆JVD ◆Heart Sounds: S 3 ◆Lung sounds: crackles ◆Peripheral edema
Diagnostics ◆EKG ◆CXR ◆U/S ◆LABS
EKG ◆TACHY? ◆BRADY? ◆ISCHEMIA?
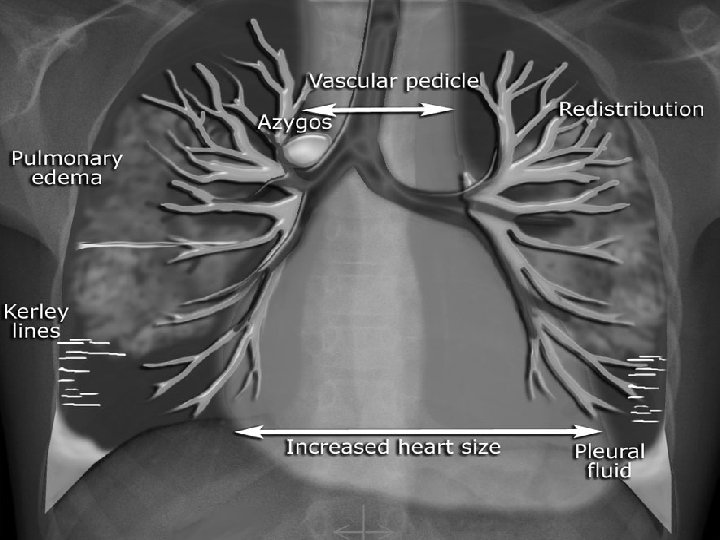
PULMONARY EDEMA
Chest Ultrasonography: Another Useful Adjunct? Midaxillary Anterior axillary Midclavear Parasternal Intercostal s pace 2 3 4 5 Gargani L, et al. Eur J Heart Fail. 2008; 10: 70 -77. Parasternal Midclavear Anterior axillary Midaxillary
Ultrasound Lung Comets Pleura Normal Soldati G, et al. Intern Emerg Med. 2008; 3: 37 -41. Acute Heart Failure
Diagnosing Acute Heart Failure in the ED: A Systematic Review and Meta-Analysis (cont’d) Cutoff (pg/m. L) N n % AHF (95% CI) Specificity % (95% CI) LR+ (95% CI) LR– (95% CI) 100 19 9143 44. 7 (43. 7 -45. 8) 93. 5 (92. 6 -94. 2) 52. 9 (51. 6 -54. 2) 2. 2 (1. 8 -2. 7) 0. 11 (0. 07 -0. 16) 200 11 3279 50. 4 (48. 7 -52. 1) 85. 9 (84. 2 -87. 6) 72. 2 (69. 9 -74. 4) 3. 1 (2. 3 -4. 0) 0. 18 (0. 12 -0. 27) 500 8 3. 915 46. 7 (45. 1 -48. 3) 67. 7 (65. 5 -69. 9) 89. 8 (88. 5 -91. 1) 9. 1 (4. 1 -20. 2) 0. 34 (0. 26 -0. 45) Ax. Sym 100 4 684 52. 3 (48. 6 -56. 1) 93. 3 (90. 2 -95. 7) 53. 1 (47. 5 -58. 6) 1. 9 (1. 5 -2. 4) 0. 15 (0. 08 -0. 29) i. STAT 100 2 585 42. 6 (38. 6 -46. 6) 94. 4 (90. 7 -96. 9) 64. 6 (59. 2 -69. 7) 3. 0 (1. 2 -7. 4) 0. 05 (0. 02 -1. 23) 300 10 3498 45. 0 (43. 4 -46. 7) 90. 4 (88. 9 -91. 8) 38. 2 (36. 0 -40. 4) 1. 8 (1. 4 -2. 2) 0. 09 (0. 03 -0. 34) 1000 8 2988 44. 8 (43. 0 -46. 6) 84. 8 (82. 8 -86. 7) 65. 5 (63. 2 -67. 8) 2. 7 (1. 9 -3. 9) 0. 20 (0. 12 -0. 33) 1550 9 3043 37. 3 (35. 6 -39. 0) 75. 5 (73. 4 -77. 9) 72. 9 (70. 6 -75. 0) 3. 1 (2. 3 -4. 3) 0. 32 (0. 20 -0. 51) 300 1 401 30. 4 (26. 0 -35. 2) 95. 9 (90. 7 -98. 6) 48. 0 (42. 0 -54. 1) 1. 9 (1. 6 -2. 1) 0. 09 (0. 04 -0. 20) Assay BNP Triage NT-pro. BNP Elecsys Dimension AHF, acute heart failure; BNP, brain (or B-type) natriuretic peptide; LR+, likelihood ratio of a positive test; LR−, likelihood ratio of a negative test; NT-pro. BNP, N-Terminal pro-BNP. Martindale JL. Acad Emerg Med. 2016; 23: 223 -242.
BNP Caveats ◆Relative increase in women ◆Inverse relationship with body mass index (BMI) ◆Higher with renal dysfunction ◆If you know they have acute CHF this is a wasted test
Triggers and Treatment for the Failing Heart
Overview of Acute Therapy 1 6 Ultrafiltration: Aqua/natriuresis 5 2 Dobutamine, dopamine, milrinone: Increased inotropy Nitrates, nitroprusside, dobutamine: Arterial vasodilation 3 Bilevel or continuous positive airway pressure: Preload reduction Nitrates, morphine: Venodilation Allen LA, O’Connor CM. CMAJ 2007; 176: 797 -805. 4 Furosemide: Natriuresis
The Pathophysiology of Acute Heart Failure Viau DM, et al. Heart. 2015; 101(23): 1861 -1867.
Treatment ◆Based on the exam ◆Spectrum of illness from mild fluid overload to cardiogenic shock ◆Think: Inlet, Pump, Outlet ◆Think: donkeys…wait what?
Basic CHF Heart = Donkey Preload/afterload = cart
Treatment Priorities ◆#1: BIPAP ◆start at IPAP of 6 cm H 2 O ◆increase to 10 -15 ◆#2: med: Nitroglycerin ◆#3 med: Furosemide
Nitro drip ◆works to decrease preload and afterload ◆no change in mortality ◆pts feel better faster
Math…really quick…
Nitro dosing ◆chest pain pts: NTG 400 mcg tablet every 5 min. This about 30% bioavailable. ◆400/5 = 80 mcg/min (x 30%) = 24 mcg/min equivalent ◆DON’T start gtt at 5 or 10 mcg/min ◆DON’T start gtt at 40 mcg/min ◆START AT 200 mcg/min
Nitro ◆Nitroglycerin (NTG) – Typical infusion range: 10 -20 mcg/min (waste of time) – Increase by 5 mcg/min every 5 min as needed up to 400 mcg/min (takes too long) ◆High dose – Repeat 2 mg bolus HD=high-dose; ICU=intensive care unit; LOS=length of stay; NSTEMI=non-ST-elevation myocardial infarction; BP=blood pressure. Levy P, et al. Ann Emerg Med. 2007; 50: 144 -152. HD NTG Controls P Value Mechanical vent 20. 7% 46. 7% 0. 023 ICU admit 37. 9% 80. 0% <0. 001 Hospital LOS (days) 4. 1± 3. 4 6. 2± 7. 3 0. 171 NSTEMI 17. 2% 28. 9% 0. 254 Low BP 3. 4% 0% 0. 210
Diuretic Dosing ◆Furosemide – 40 -mg intravenous (IV) push is not enough – author gives 200 mg IV. Pts get better faster and have no increase in adverse outcomes. – no advantage to a lasix drip BUN=blood urea nitrogen.
Cardiogenic Shock ◆the severe end of the spectrum ◆less than 5% of CHF pts ◆usually due to MI or valve rupture ◆need to be in the cath lab/CV surgery ◆we provide only supportive care
Cardiogenic Shock ◆need inotropic support ◆Dobutamine is probably the best ◆increases cardiac contractility but also is a vasodilator (1/3 of pts get hypotensive) ◆Norepinephrine ◆add if pt gets hypotensive ◆probably benefit from intubation
Other meds: ◆ACE inhibitors ◆Enalaprilat 1. 25 mg IV ◆Captopril 25 mg SL ◆add if you are at very high dose NTG drip ◆Morphine ◆Waste of Time ◆doesn’t help much with venous dilation or arterial dilation. ◆poor anxiolytic
Disposition
Sample Observation Unit Protocol • SBP >160 mm Hg • Duration of symptoms: 24 -48 h • Euvolemic/mild hypervolemic Observation unit monitoring • Continuous-pulse oxygen and ECG • Weigh patient • Intake & output • Fluid restriction (2000 m. L/d) • 2 -g sodium diet • Place on home dose of ACEI/ARB and β-blocker • Consider echocardiogram • Vasodilator NTG 0. 4 mg, SL q 5 min x 3 doses then NTP 1"-2" • Diuretic (moderate dose) Treatment • SBP 100 -160 mm Hg • Duration of symptoms: days to weeks • Hypervolemic • Diuretic (aggressive dose) • Consider vasodilator if hypertensive Reassess every 4 to 6 hours Improved • Good urine output • SBP normalized at 100 -120 mm Hg • Improved symptoms • Serum sodium >135 m. Eq/L Partial response • Consider repeat diuretic • Consider IV vasodilator Discharge, prescribe, and document • ACEI/ARB (LVEF <40%) • β-blocker • Education • Aftercare Fermann GJ, Collins SP. Curr Heart Fail Rep. 2010; 7: 125 -133. Worse • Poor urine output • SBP <90 mm Hg or >160 mm Hg • Increased symptoms • Serum sodium <135 m. Eq/L Admit to hospital
Inpatient Management
Therapeutic Goals ◆ Stabilization phase (first 24 -48 hours) – Improve symptoms – Balance hemodynamics – Achieve euvolemia – Avoid harm! ▪ Myocyte injury ▪ Renal damage ◆ Implementation phase (>48 hours) – Initiate lifesaving interventions ▪ Angiotensin-converting enzyme (ACE) inhibitors, β-blockers, etc Gheorghiade M, et al. Am J Cardiol. 2005; 96(suppl): 11 G-17 G.
Inpatient Meds B-blockers Digoxin
Stabilization Phase ◆Identify trigger of exacerbation – Nonadherence to diet – Nonadherence to medications – Progression of disease – Ischemia – Arrhythmia
If Not Improving, Reassess Diagnosis 10 Most Common Pairs of Discrepant Admission and Primary Discharge Diagnosis Codes Admission Diagnosis Code Description Principal Discharge Diagnosis Code Description 786. 05 Shortness of breath 428. 08 Congestive heart failure, unspecified 786. 50 Chest pain, unspecified 786. 59 Chest pain, other 786. 05 Shortness of breath 486 Pneumonia, organism unspecified 780. 6 Fever 996. 62 Infection and inflammatory reaction due to other vascular device, implant, or graft 789. 00 Abdominal pain, unspecified site 577. 0 Acute pancreatitis 780. 6 Fever 599. 0 Urinary tract infection, site not specified 786. 05 Shortness of breath 491. 21 Obstructive chronic bronchitis with acute exacerbation 786. 05 Shortness of breath 415. 19 Pulmonary embolism and infarction, other 786. 05 Shortness of breath 493. 22 Chronic obstructive asthma with acute exacerbation Johnson TM, et al. J Hosp Med. 2009; 4(4): 234 -239.
Discharge Planning Is this patient medically ready for discharge today?
Discharge Medication Reconciliation Martin D, et al. J Gerontol Nurs. 2012; 38(6): 24 -37.
Summary ◆CHF is an epidemic ◆CHF is a disease spectrum ◆For the sickest: ◆BIPAP immediately ◆High dose NTG drip ◆Lasix (late) but in bigger doses ◆Work with admitting team to coordinate care
Tired of this? Any questions?