Healthy Newborn Objectives Identify key physical differences between

Healthy Newborn


Objectives • Identify key physical differences between the preterm infant and full term infant • Identify normal vital signs for a newborn • What are key signs of resp distress?

Newborn facts • Neonatal period- 1 st 28 days of life • 1 st 24 hours after birth is the most hazardous time • 2/3’s of infant deaths that occur during the 1 st year of life happen during this time and ½ of those occurs in the 1 st 24 hours

Physiologic Adjustment • Periods of reactivity 1 st 6 hours of life, all newborns go thru periods of irregularity prior to their body systems stabilizing 1 st period of reactivity (1 st ½ hour) Quiet resting period (sleeps for 1 ½ hours)
 • This")
Physiologic Adjustment • Second period of reactivity (b/t 2 & 6 hours) • This typical reactivity pattern demonstrates that the newborn is adjusting well to extrauterine life

Dubowitz Maturity Scale Gestational Assessment • • • Observation of sole creases Breast nodule diameter Scalp hair Ear lobe Testes and scrotum Skin

• Ballard’s assessment of gestational age • Score is determined and “matches” weeks gestation Gestational Age

Nursing Care • • Vital Statistics Weight Length Head circumference Abd circumference Temp, Pulse, Respirations BP only if cardiac defect suspected

Weight • Establish a baseline • Is infant small or large for gestational • • • age? IUGR? Preterm? Post dates? Average weight at term for infant = 7. 5 lbs Newborns of non-white women in USA weight 0. 5 lbs less Loses 5 -10% of birth weight (6 -10 oz) during first few days of life
 female to 54 cm (21. 3")
Length • Average 53 cm (20. 9 in) female to 54 cm (21. 3 in) male • 46 cm to 57. 3 cm (18 -24 in) • All data points need to be plotted on graph

Head and Chest Circumference • The chest circumference of a newborn should be about two cm’s less than head circumference • Average 34 -35 cm. • Any >37 or < 33 needs to be investigated

Vital Signs • Temperature – range 36. 5 to 37 axillary Heat loss in newborns occurs by • • Convection Conduction Radiation Evaporation

Temperature • If chilling is prevented the neonates’ temperature will stabilize within 4 hours after delivery and be 98. 6 F or 37 C • Infection may not cause an increase in temperature and subnormal temperatures need to be investigated

Etiology/Precipitating Factors for Temperature Changes • • • Hypothermia Prematurity Asphyxia Sepsis Neurologic conditions Inadequate drying and warming • Exposure to cold environmental conditions

Etiology/Precipitating Factors for Temperature Changes • Hyperthermia • Excessive environmental temperature • • Dehydration Infection Phototherapy CNS damage from trauma or drugs

Pulse • Range 120 -160 bpm • May be as low as 100 bpm while sleeping to 180 bpm when crying • Color pink with acrocyanosis • May be irregular with crying

Signs of Distress • Heart murmurs - all murmurs should be followed up and referred for medical evaluation • Faint sound • Central cyanosis

Respirations • Range 30 – 60 breaths per minute • Nose breathers • Moist breath sounds may be present shortly after birth • Bronchial breath sounds bilateral

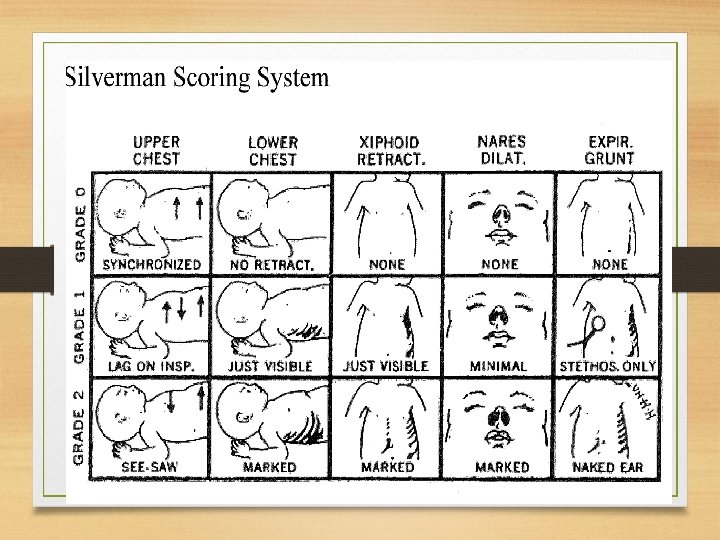
Respiratory Distress • • • Asymmetrical chest movements Apnea >15 seconds Diminished breath sounds Grunting, Nasal flaring, Retractions Persistent irregular breathing Persistent fine crackles Tachypnea- >60 Excessive mucus Stridor

Blood Pressure • Not done routinely • Average newborn 65/40 in both upper and lower extremities • Varies with change in activity level • Must use appropriate size cuff accurate reading

Eyes and Ears • Acuity takes 6 months but able to track mom’s face, no peripheral vision, loves complex patterns • Ears-hearing acute

Preventing “Shaken Baby Syndrome” • • • P=Peak of crying U=Unexpected R=Resists soothing P=Pain like face L=long lasting E=Evening • Step back, take 5.
 • Transcutaneous Bilirubin meter done at 24 hours (a touch")
What’s New? (AAP 2012) • Transcutaneous Bilirubin meter done at 24 hours (a touch on the forehead) • Pulse Ox test done at 24 hours ( on hand right wrist and leg) CCHD screening • No rectal temps after birth • No use of bulb syringes in cribs (VVMC)

In delivery room • Delay blow by O 2 Observe infant closely by using O 2 sat monitoring New standard of practice in all hospitals
- Slides: 26