HEALTHY MOMS STRONG BABIES St Joseph Community Health

HEALTHY MOMS. STRONG BABIES. St. Joseph Community Health Foundation Prenatal and Infant Care Luncheon Thursday, November 21 Jeena Siela, MPH; Director, Maternal-Child Health and Government Affairs

OUR MISSION MARCH OF DIMES LEADS THE FIGHT FOR THE HEALTH OF ALL MOMS AND BABIES.

MOMS AND BABIES ARE FACING AN URGENT HEALTH CRISIS The U. S. has one of the WORST RATES of maternal death in the developed world. African American women are significantly more likely to die. Women of color are up to 50% more likely to give birth prematurely. Their children can face a 130 percent higher infant death rate. 1 IN 7 women are treated for depression some time between the year before or after pregnancy. Over half of the cases of postpartum depression go undiagnosed. . Premature birth and its complications are the largest contributors to INFANT DEATH in the U. S. and globally.

MARCH OF DIMES… SUPPORTS RESEARCH toward solutions that ensure every baby is born healthy. ADVOCATES for policies that prioritize the health of moms and babies. PROVIDES RESOURCES and programs to help moms before, during and after pregnancy. EDUCATES medical professionals on known solutions to improve the care that moms and babies receive. UNITES local communities across the nation through events and collaboratives. PARTNERS with organizations and companies committed to helping moms and their families.

MARCH OF DIMES HAS AN 80 YEAR LEGACY OF IMPACT AND INNOVATION Pioneered vaccine research leading to the eradication of POLIO in the U. S. , one of the great scientific achievements of the 20 th century. (MOD) Led the advocating for state implementation of universal NEWBORN SCREENING for rare but serious conditions, leading to earlier life-saving treatment and intervention for at least 3, 400 additional newborns each year. (CDC) Launched the nation's first PREMATURITY RESEARCH Centers dedicated to solving the mysteries of premature birth Advocated for folic acid fortification in the U. S. and leader of a FOLIC ACID public education campaign, contributing to a reduction of neural tube defects in newborns of 30%. (MOD)

MATERNAL MORTALITY

700 WOMEN DIE EACH YEAR IN THE US FROM PREGNANCYRELATED COMPLICATIONS 7

DEFINITIONS Maternal Death Maternal death while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management but not from accidental or incidental causes. Pregnancy-related death Maternal death while pregnant or within 1 year of the end of a pregnancy as a complication of pregnancy, aggravation of an unrelated condition by the physiology of pregnancy or chain of events initiated by the pregnancy, Excludes accidental or incidental causes

TREND IN MATERNAL MORTALITY Pregnancyrelated death has more than doubled over the past 25 years. Pregnancy-related mortality ratio is the number of pregnancy-related deaths per 100, 000 live births. A pregnancy-related death is the death of a woman during pregnancy or within one year of the end of pregnancy from a pregnancy complication, a chain of events initiated by pregnancy, or the aggravation of an unrelated condition by the physiologic effects of pregnancy. Source: CDC, 1987 -2013 (https: //www. cdc. gov/reproductivehealth/maternalinfanthealth/pmss. html) Prepared by March of Dimes Perinatal Data Center, March, 2018.

DISPARITIES IN MATERNAL DEATH Pregnancy-related mortality ratio is the number of pregnancy-related deaths per 100, 000 live births. A pregnancy-related death is the death of a woman during pregnancy or within one year of the end of pregnancy from a pregnancy complication, a chain of events initiated by pregnancy, or the aggravation of an unrelated condition by the physiologic effects of pregnancy. Source: CDC, 2011 -2013 (https: //www. cdc. gov/reproductivehealth/maternalinfanthealth/pmss. html) Prepared by March of Dimes Perinatal Data Center, February 2018.

MATERNAL MORTALITY AMONG VERY HIGH HUMAN DEVELOPMENT INDEX COUNTRIES

TIMING OF DEATH Source: Creanga, A. Syverson, C. Callaghan, W. M. Pregnancy-Related Mortality in the United states, 2011 -2013. (2017). Obstetrics and Gynecology, 130(2). 12

PREGNANCY-RELATED MORTALITY BY RACE UNITED STATES, 2011 -2013 * The pregnancy-related mortality ratio is defined as the number of pregnancy-related deaths per 100, 000 live births. A pregnancy-related death is defined as the death of a woman during pregnancy or within one year of the end of pregnancy from a pregnancy complication, a chain of events initiated by pregnancy, or the aggravation of an unrelated condition by the physiologic effects of pregnancy. Source: CDC (https: //www. cdc. gov/reproductivehealth/maternalinfanthealth/pmss. html )

DEMOGRAPHIC RISK FACTORS • Persistent racial and ethnic disparities for more than 20 years • Increased maternal age – 3 in 10 women who died between 2011 -2013 were over the age of 35. • About 30% of maternal deaths had no prenatal care or began care later than their first trimester • 1 in 6 pregnancy-related deaths were obese May 2018 Source: Creanga, A. , Syverson, C. Seed, K. , Callaghan, W. (2017). Pregnancy-related morality in the United States, 2011 -2013. Obstetrics and Gynecology. 130(2), 366 -373 14

FORWARD THINKING • Lack of access to health insurance, family planning, mental health care, substance abuse treatment and other services that could cause healthier preconception periods • Lack of access in rural areas • Lack to health literacy to understand or communicate with their providers • A vast amount of information is given a women at the time of birth and little of that relates to symptoms after birth that are abnormal and they should return to the hospital Source: Suplee P. D. , Bingham D. , & Kleppel L (2017). Nurses’ knowledge and teaching of possible postpartum complications. The American Journal of Maternal/Child Nursing, 42. 15

2019 MARCH OF DIMES REPORT CARD MATERNAL AND INFANT HEALTH: CONTEXT AND ACTION SELECTED SOCIAL DETERMINANTS OF HEALTH Our unequal society has negative consequences for health. Factors such as these are linked to adverse maternal and infant health outcomes overall. Many other structur mothers and babies, especially for Black, American Indian and Alaska Native women. For example, income, health insurance status and prenatal care access are tra are held constant, racial and ethnic disparities persist. March of Dimes is collaborating with others to confront social and structural determinants of health, while ide impacts of such inequities. Uninsured among women (15 -44)* 11. 7 11. 1 HP 2020 22. 4 Inadequate Prenatal Care United States 15. 0 Indiana 16. 3 15. 1 Poverty among women (15 -44) 15. 7 *The Healthy People 2020 goal is for all women (15 -44) to be insured. 14. 6 0 10 20 Source: IPUMS-USA, University of Minnesota, ipums. org. American Community Survey. US Census Bureau; IPUMS-CPS, University of Minnesota, ipums. org. Current Population Survey. US Census Bureau; National Center for Health Statistics, 2017 final natality data. 30 40 MARCHOFDIMES. ORG/REPORTCARD

2019 MARCH OF DIMES REPORT CARD MATERNAL AND INFANT HEALTH: CONTEXT AND ACTIONS OTHER RECOMMENDED STATE ACTIONS March of Dimes recommends key policy actions to improve maternal and infant health in all states. Future Report Cards will assess these actions at the state level. • COMPREHENSIVE MEDICAID COVERAGE EXTENSION FOR ALL WOMEN TO AT LEAST ONE YEAR POSTPARTUM In too many states, Medicaid maternity coverage ends 60 days after giving birth, ending access to care at a time when risks of maternal complications and death persist. • GROUP PRENATAL CARE ENHANCED REIMBURSEMENT Group prenatal care has shown significant benefits to maternal health, increases healthy behaviors and reduces adverse birth outcomes. Increased benefits were seen in Black women who participated in group prenatal care. Enhanced reimbursement models, including delivery and outcomes-based incentives, can encourage providers to offer it. • MATERNAL MORTALITY REVIEW COMMITTEES Establishment, funding and reporting of state data to CDC through Maternal Mortality Review Committees is essential to understanding and addressing the causes of maternal death. MARCHOFDIMES. ORG/REPORTCARD

2019 MARCH OF DIMES REPORT CARD PRETERM BIRTH RATES AND GRADES BY STATE Preterm is less than 37 weeks gestation based on obstetric estimate. Source: National Center for Health Statistics, 2018 final natality data. MARCHOFDIMES. ORG/REPORTCARD

2019 MARCH OF DIMES REPORT CARD RACE & ETHNICITY DISPARITY BY STATE The March of Dimes disparity ratio measures and tracks progress towards the elimination of racial/ethnic disparities in preterm birth. It's based on Healthy People 2020 methodology and compares the group with the lowest preterm birth rate to the average for all other groups. Progress is evaluated by comparing the current disparity ratio to a baseline disparity ratio. A lower disparity ratio is better, with a disparity ratio of 1 indicating no disparity. Gestational age is based on obstetric estimate. Race categories include only women of non-Hispanic ethnicity. Source: National Center for Health Statistics, 2015 -2017 natality data MARCHOFDIMES. ORG/REPORTCARD
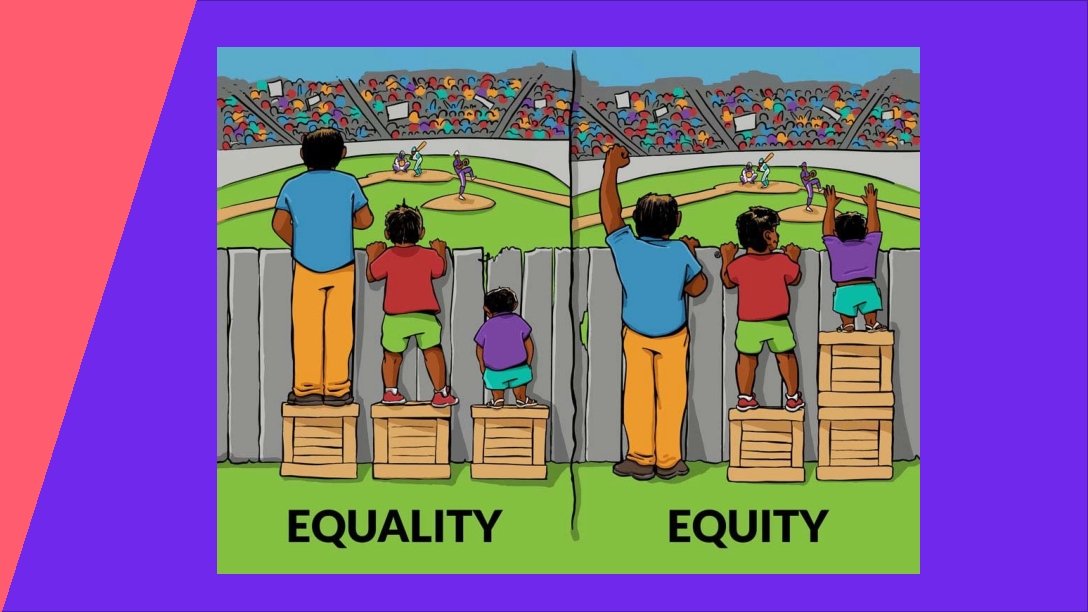
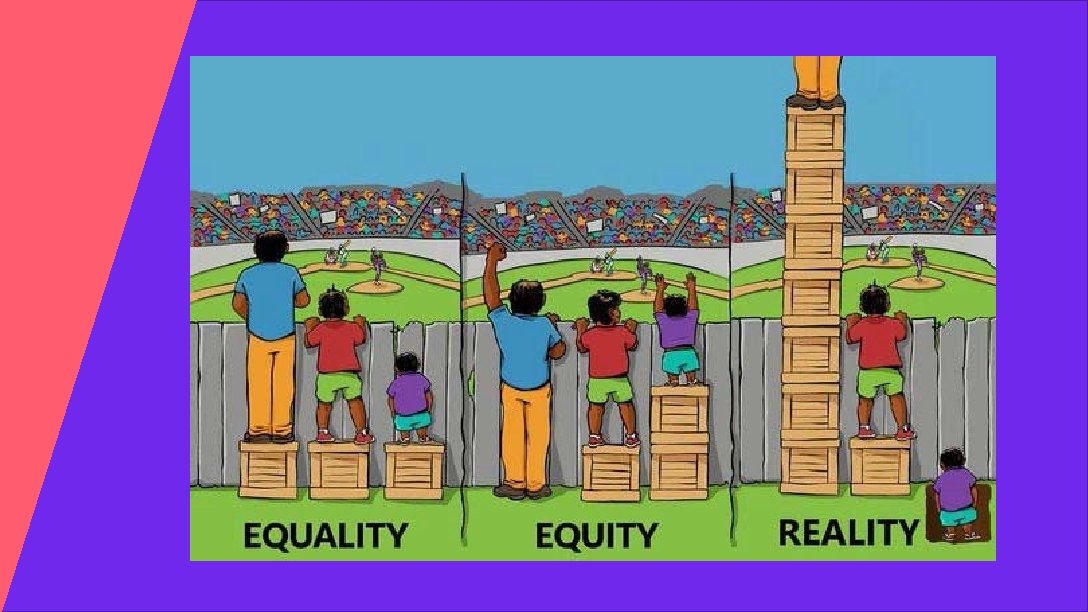

HEALTH EQUITY “everyone has a fair and just opportunity to be as healthy as possible. ” Braveman et al, 2017 BIRTH EQUITY “the assurance of the conditions of optimal births for all people with a willingness to address racial and social inequalities in a sustained effort. ” National Birth Equity Collaborative

WHAT IS MARCH OF DIMES DOING AROUND HEALTH EQUITY? CONVENING IMPLEMENTING DRIVING CHANGE Bringing partners together Developing & delivering programs Using data to address disparities 23

Address the Problem at Multiple Levels WIDER COMMUNITY Health care access, equitable and culturally sensitive care, life course perspective, meaningful engagement of patients/communities, effective health promotion, service integration, data systems, name and challenge “isms” Understand that nature of the problem for your community. Promote social equity (equal access and opportunity) HEALTH SYSTEM INDIVIDUAL Health education, counseling, screening, access to resources, respect inherent worth and dignity of each person, name and challenge “isms”
 in 2019 to develop implicit")
IMPLICIT BIAS TRAINING MOD collaborated with Quality Interactions (QI) in 2019 to develop implicit bias training. QI is a Minority Owned Business founded in 2003 by Harvard-trained experts in health equity and exclusively delivers research-and evidencebased cultural competence and implicit bias training in hospital, health plan, and medical school settings. 25

IMPLICIT BIAS TRAINING KEY COMPONENTS 1. Overview of implicit bias 2. Historical overview of structural racism in the United States 3. Strategies to mitigate racial bias in maternity care 4. Commitment to creating a culture of equity 26

WHY IMPLICIT BIAS TRAINING? • A strategy to improve patient-provider communication and treatment decisions, contributing to improved quality of care. • Provide healthcare professionals with important insights on how to recognize and remedy implicit bias. • Training alone will not lead to immediate improvements in racial and ethnic disparities in birth and maternal health outcomes • Improved patient experience, better quality of care, and culture shift across committed organizations towards the broader goal of achieving equity for all moms and babies. 27

IMPLICIT BIAS: NEXT STEPS In October we co-developed the main content of the training with Quality Interactions. It was mutually decided that we would further test the content with our initial focus group participants and that we would complete the entire e-learning course prior to launching the training. 2020 goal of: • Live, in-person trainings • Live, webinar trainings • Self-directed, e-learning experience If you need any additional information or have questions or concerns, please contact Kweli Rashied-Henry, MOD health equity director at krashied-henry@marchofdimes. org or call (919) 424 -2158. 28

BEYOND LABELS MICROSITE MOD has an award-winning microsite on stigma, https: //beyondlabels. marchofdimes. org/. The toolkit was created to raise awareness about the impact of stigma for all March of Dimes staff and partners. Stigma and implicit bias are based on stereotyping, which means assigning labels and/or categorizing people based on negative perceptions. The stigma toolkit is currently a free resource. 29

THANK YOU Jeena Siela, MPH Director, Maternal-Child Health and Government Affairs March of Dimes Indiana jsiela@marchofdimes. org (317) 285 -0192
- Slides: 30