Health Promotion in rural Nepal Jane Stephens Director
")



 • What is the situation on the ground?")








- Slides: 14
Health Promotion in rural Nepal Jane Stephens, Director Green Tara Trust (UK)
Purpose of Programme • Government policy and health systems change need to be informed by good quality evidence from the field, and vice versa • All forms of good quality evidence need to be included- qualitative, quantitative, case studies, lessons learned from implementation of field programmes • Create opportunities for dialogue between field, district, national and international level where all are seen as equally valuable.
Health Promotion Cycle Needs assessment Evaluation Health Promotion Cycle Implementation Programme Planning
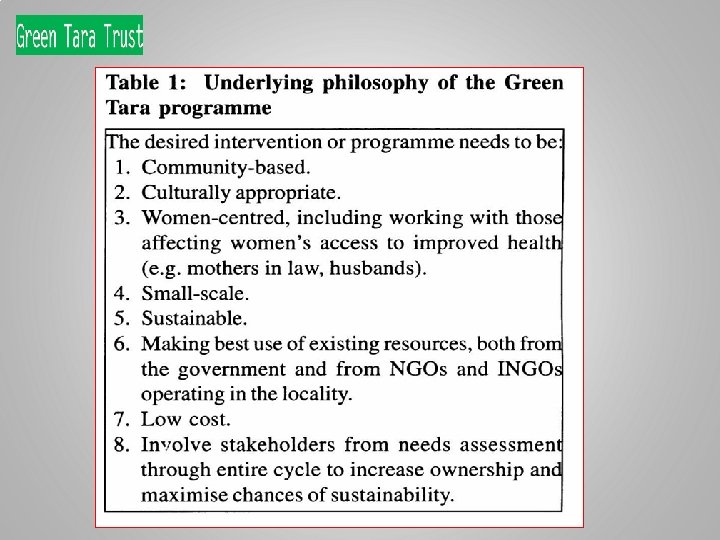
Our methods Helping communities find their own solutions to health problems
Needs assessment • First Phase: (2006) • What is the situation on the ground? • Available data - GON, university student projects, Gvt. and NGO programmes • Community visit, broad FGDs and IDIs- identify main problems • Second phase: • Needs assessment- quantitative and qualitative • Confirm problems, find out WHY problems exist and main players
Needs assessment • • Third phase: Dissemination of findings Fourth phase: Negotiation of community priorities between different groups and who will take responsibility for each part? Young people Fertile Women Mother in laws Fathers Teachers Politicians Health workers
Programme planning from Needs Assessment • Identified 3 major target areas • Improving antenatal attendance & quality of care • Increasing women’s decision making power around health decisions • Increasing number of women having trained attendants at delivery • Participatory Action Research: monitoring by community-empowerment & sustainable behaviour change, external monitoring by GTN staff, external evaluation
Sketching Monitoring Map in Village
Implementation – Main Activities • 2 Government trained HW - HP for 10, 000 people • Reactivation/ formation women’s groups • Home visits • Mass events • Training for traditional healers, FCHVs • Support to health facilities: goods, mentoring • Mobile ANC clinics in areas far from health post
Implementation – Resources required • People; key community players • Skills: training in HP & PRA • Motivation to improve own and community’s health • Infrastructure: existing buildings, health facilities, empty community buildings • Support from main players at ALL levels • Transparent & clear health systems with people in ‘post’ • Goods: teaching materials, small incentives • Small amounts of money: transport, meetings
Implementation – Challenges • Previous NGOs providing incentives: hard to change this behaviour • How can we encourage environment of positive behaviour change that is sustainable in this environment? • Critical thinking and ability to reflect • Participation requires some self-confidence and breaking down of hierarchy; and we can only set up environment, people need to take responsibility for their own behaviour • How can we set up the conditions for this shift in thinking and behaviour to come about in Nepal?
HP in low-resource setting: rural Nepal • Greater need and scope of health promotion • Advocacy in support of health promotion at all level • Alliances & networks • Need to move beyond disease prevention approach Paper is freely available on the web: www. healthrenaissance. org. np/uploads/7141_24852_1_PB. pdf
Thank you Contact UK Karunamati: doctorjane 99@hotmail. com Padmadharini: Director- gttpadmadharini@gmail. com Nepal Green Tara Nepal: Ram Chandra Silwal, Country Director gttn@wlink. com. np