Health Measurement Why care about health Health affects

Health - Measurement

• Why care about health?

• Health affects income through its impact on human capital…better health means more schooling and higher productivity. • Greater worker productivity • More savings - Rising longevity encourages youngsters to save, which boosts investments. • 1 additional year of life expectancy associated with 4% increase in GDP per capita (difficult to test for causality)

• As incomes grow, individuals invest in higher quality diets, improved sanitation practices and better health care. The reverse channel is also operational. • Higher quality diets usually rich in iron, vitamin-A, iodine and other micronutrients.

• Life is better now than at almost any time in history • People live longer, there is lower child mortality, we have food certainty (and choice), time-saving machines (laundry, dishwashers) • Yet, progress has been unequal and non-linear

The Worst Mistake in the History of Mankind? • Agricultural transition, according to Jared Diamond • Varied diet, roughage, high in protein, low in fat • Brisk walking • Low fertility • Less contamination

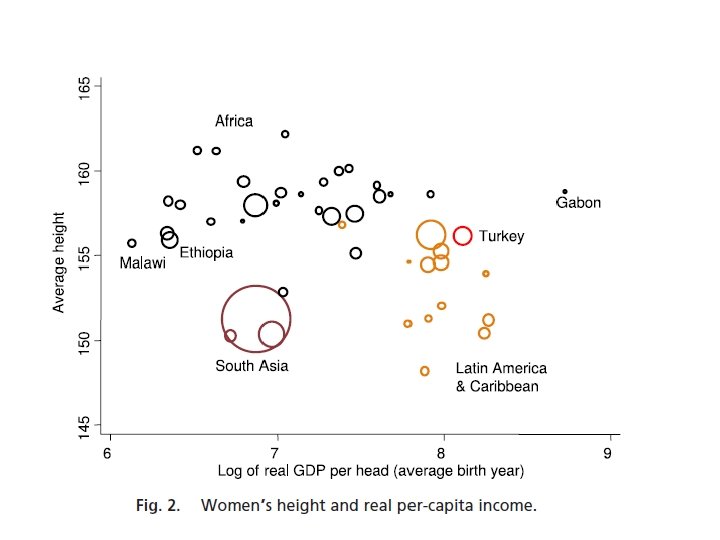
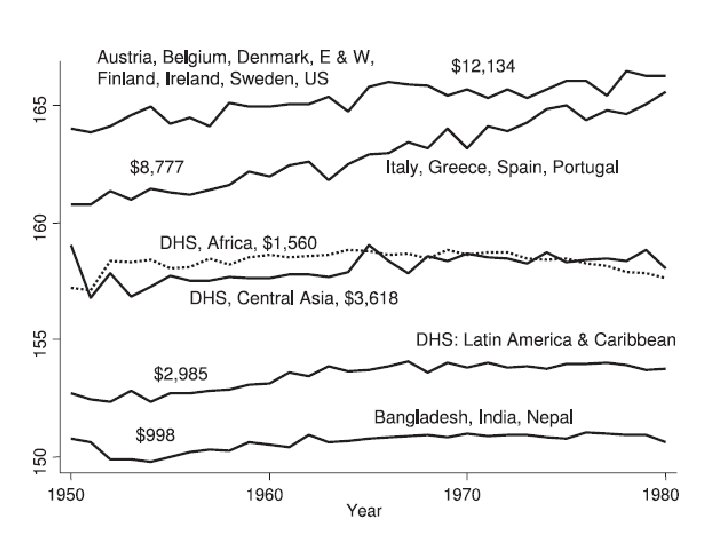
Height • Adult height is determined by genetic potential and by net nutrition, the balance between food intake and the demands on it, including the demands of disease, most importantly during early childhood. (Deaton, 2007) …taller people earn more on average, do better on cognitive tests, and live longer

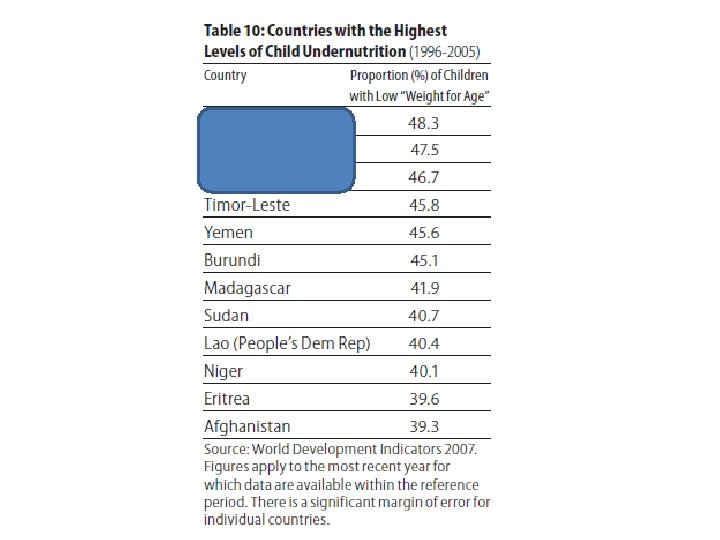
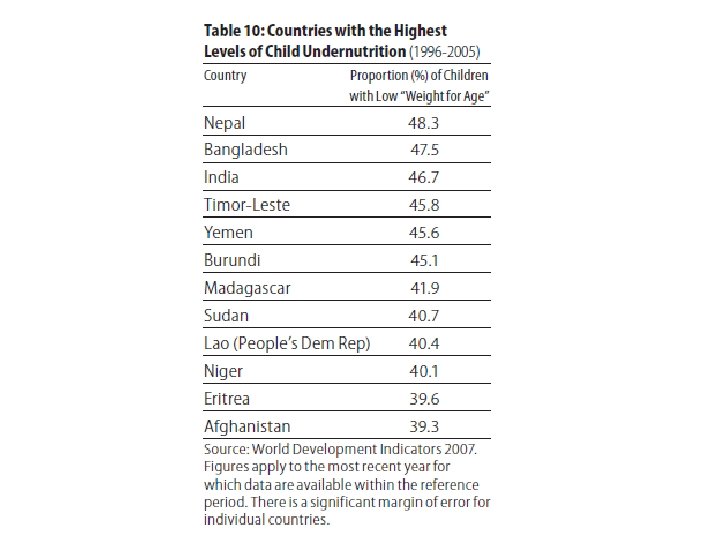
Stunting around the world

• Selection versus scarring

• In Mali in 1960, median life expectancy was 5 years. • Yet the surviving women reached an average height of 162 cm in adulthood as opposed to 151 cm for Indian women and 154 cm for Columbian women.

Fixed effects • Controlling for omitted variables in panel or repeated cross-sectional data • Fixed effects are usually used when there is panel data to control for factors that are fixed over time • If Acemoglu had panel data on property rights and gdp per capita, he should have included country fixed effects to control for variables that affect gdp per capita but are fixed over time within a country

• How does it work? • Include a dummy variable for each country – so if there are 200 countries, there should be 200 dummy variables and these are called together as country-fixed effects • This is effectively only using variation within each country to predict the coefficient. It is not comparing countries with each other.

• What if there is a common effect on all countries that changes every year? – For example, technological change or climate change

• Then include a set of year fixed effects
 and you")
• What if countries are innovating at different rates (omitted variable) and you want to control for this in your regression? • Use Country time trends. This is a countryspecific variable that controls for linear trends.
 – standards")
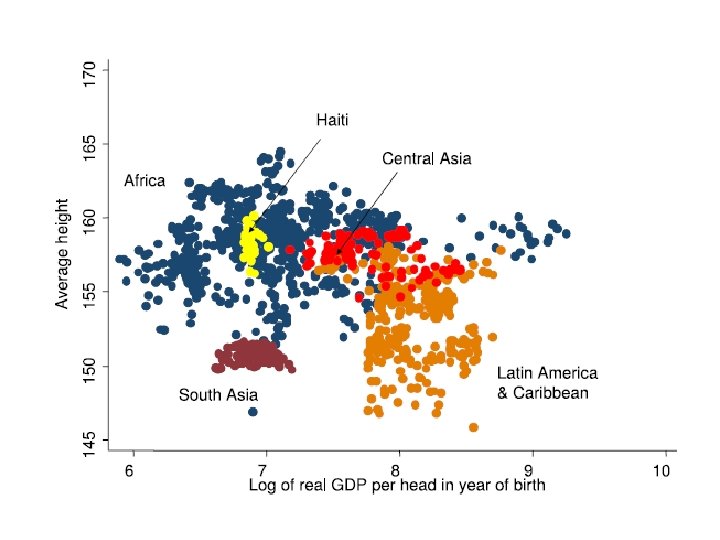
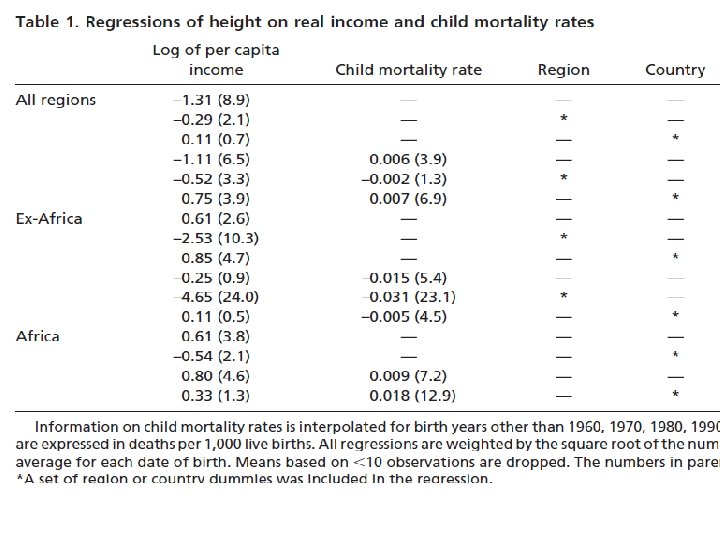
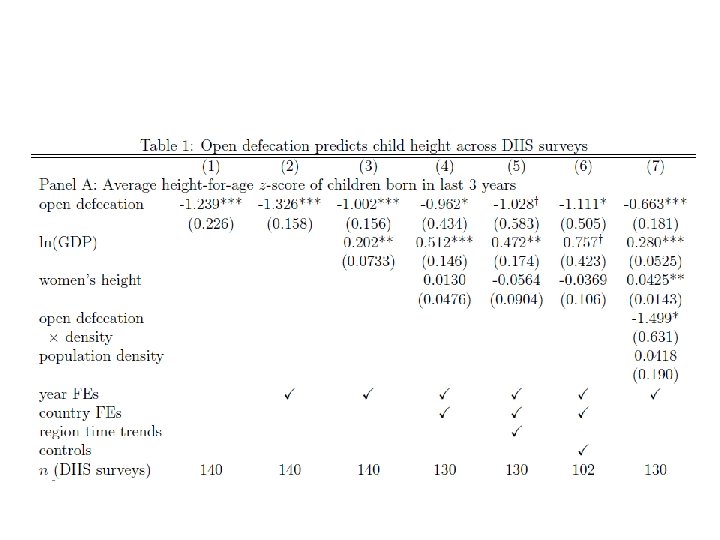
Puzzle: Height appears to be uncorrelated with income • Genetic potential (Panagariya) – standards are wrong • Cultural view – cereal vegetarian diet? • Exposure to open defecation more common in India than in SSA (Spears) • Stunting is heterogeneous depending upon birth order and sex of child. First-born boys in India are taller than their peers in SSA. (Jayachandran and Pande)

Spears

Jayachandran and Pande

• For children, anthropometric indicators are typically based on age, height and weight. Three standard indicators are - “height-for-age”- Cumulative indicator of nutritional deprivation, low height-for-age is referred to as “stunting”. - “weight-for-height” – Indicator of short-term nutritional status, low weight-for-height is referred to as “wasting” - “weight-for-age”- Captures both stunting and wasting, low weight-for-age is referred to as “underweight”.

Puzzle • Less wasting among certain populations, but they are still stunted, in spite of the absence of any significant food deprivation. - “Genetic potential” hypothesis – less accepted now in the literature - “Social determinants” hypothesis: Stunting among privileged children reflects social factors such as a poor epidemiological environment, inadequate social support, and inappropriate social norms relating to breastfeeding or child feeding. - “Gradual catch-up” hypothesis: Indian children have the same genetic potential as children in the reference population, but it takes time for the heights of privileged children to catch up.
 correlated with income?")
• Is nutrition (consumption of calories) correlated with income?
 • Real GDP per head in India grew at 3.")
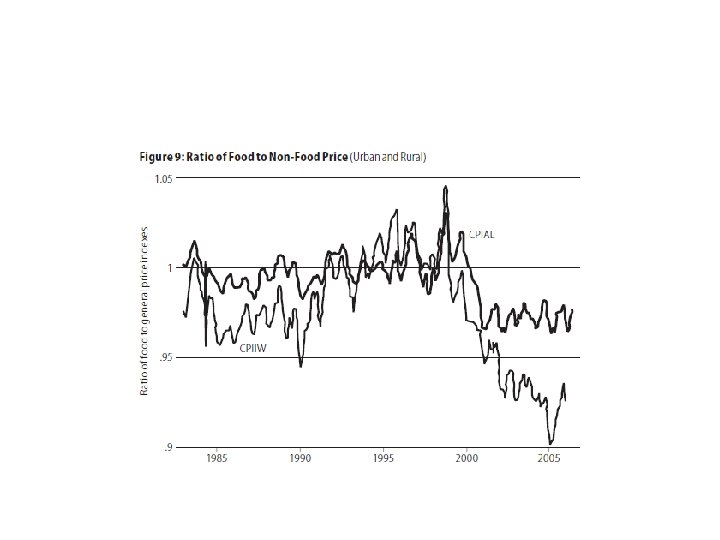
Deaton and Dreze (2009) • Real GDP per head in India grew at 3. 95% a year from 1980 to 2005, and at 5. 4% a year from 2000 to 2005. • In contrast to per capita total expenditure, there has been no real increase in per capita food expenditure, particularly after 1987 -88.

• The Engel Curve tracks the consumption of a Good X as an individual’s income changes. Income is plotted on the x-axis and the quantity of Good X consumed is plotted on the y-axis. The curve that follows the amount of Good X consumed as income increases plots the Engel Curve. • The slope of the Engel Curve also tells us whether or not the good is a normal good or inferior good. If the slope of the curve is positive, the good is a normal good because consumption increases as income is increased. If the slope of the curve is negative, the good is an inferior good because consumption decreases as income is increased.

• Calorie elasticity is the slope of the Engel curve where per capita calorie consumption is plotted against per capita household expenditure.

Calorie Engel Curve • It plots per capita calorie consumption against per capita household expenditure. • There has been a downward drift of the curve for the last 20 years for both rural and urban households.
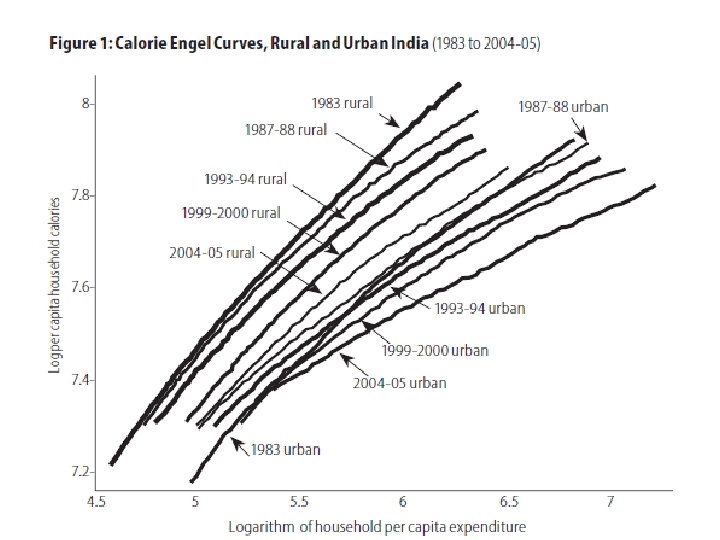

• ‘Benchmark’ view- Calorie elasticities of around 0. 3 -0. 4 in the poorest households which fall as calorie availability increases.

• Misreporting of food consumption- May be more pronounced in expenditure surveys than 24 -hour nutrition surveys - Food consumption by non-members is systematically related to household expenditure (richer households have more servants, feed more guests, own more livestock) - Overstatement of calorie availability in richer households - Upward bias to calorie estimates

• “When you are unemployed, which is to say when you are underfed, harassed, bored, and miserable, you don’t want to eat dull wholesome food. You want something a little bit ‘tasty’. There is always some cheaply pleasant thing to tempt you. Let’s have three pennorth of chips! Run out and buy us a twopenny ice-cream! Put the kettle on and we’ll all have a nice cup of tea!”

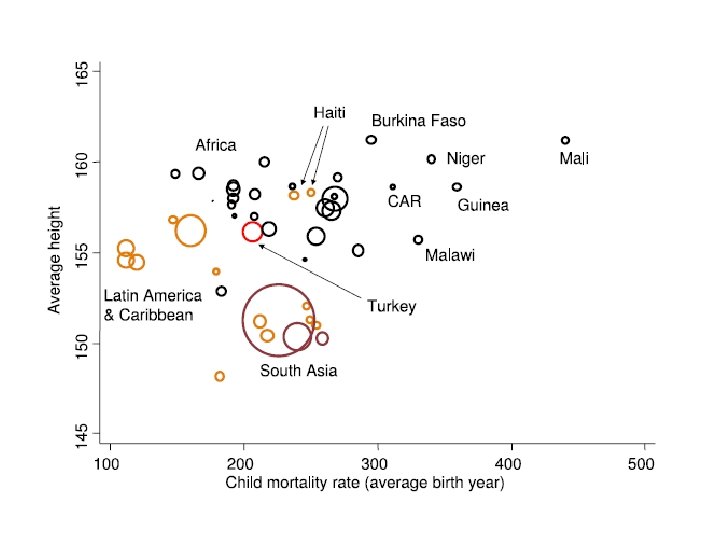
Lessons so far • Stunting is a serious multi-faceted problem that is negatively correlated with child mortality when looking at Africa and Asia. • Stunting and wasting may not move together. • Income growth of households not likely to improve nutritional status much (as Engel curves are becoming flatter). • Reducing calorie deficits among poor households by improving the quantity, quality and diversity of food remains very important (especially in South Asia).

Health – early childhood environment as a determinant Prakarsh Singh
")
Environmental hypotheses • Early childhood environment (disease vectors, breastfeeding, food, curative and preventive care) is critical for growth.

Key issues • Technological or Informational solution? • Changing household behavior through voice, information or incentives? • Demand-side or supply-side incentives? • How do demand supply-side interact with each other?


How do these worms affect child health? • Hookworm, roundworm, whipworm, and schistosomiasis infect more than one-quarter of the world's population. • Studies in which medical treatment is randomized at the individual level give biased estimates

• Miguel and Kremer evaluate a Kenyan project in which school-based mass treatment with deworming drugs was randomly phased into schools, rather than to individuals, allowing estimation of overall program effects. • The program reduced school absenteeism in treatment schools by one-quarter, and was far cheaper than alternative ways of boosting school participation. • Deworming substantially improved health and school participation among untreated children in both treatment schools and neighboring schools, and these externalities are large enough to justify fully subsidizing treatment. • No evidence that deworming improved academic test scores.

To make it free or compulsory?

In the United States, public health measures such as improved sanitation, provision of clean drinking water, and hookworm and malaria eradication are the main factors behind the massive improvements in child health in the past 150 years. Household behavior played a minor role. (Dupas, 2011)

• In 1809, Massachusetts passed the first immunisation law in the USA requiring smallpox vaccination for the general population. The constitutionality of the Massachusetts law was questioned when Henning Jacobson of Cambridge, Massachusetts, refused to be vaccinated against smallpox.

Henning Jacobson • “A compulsory vaccination law is unreasonable, arbitrary and oppressive, and therefore, hostile to the inherent right of every freeman to care for his own body and health in such way as to him seems best; and that the execution of such a law against one who objects to vaccination, for whatever reason, is nothing short of an assault upon his person. ”

US Supreme Court • “The liberty secured by the constitution of the United States to every person within its jurisdiction does not import an absolute right in each person to be, at all times and in all circumstances, wholly freed from restraint. There are manifold restraints to which every person is necessarily subject for the common good. ”
 estimates that more than 2 billion people")
• The World Health Organization (WHO) estimates that more than 2 billion people are deficient in key vitamins and minerals, particularly vitamin A, iodine, iron and zinc

• Food fortification is one of the strategies that has been used safely and effectively to prevent micronutrient deficiencies and has been practiced in developed countries for well over a century now. • In the early 20 th century, salt iodization began in Switzerland; vitamin A-fortified margarine was introduced in Denmark in 1918; and in the 1930 s, vitamin A-fortified milk and iron and B complex flour was introduced in a number of developed countries.
 • “Hemoglobin concentrations showed a significant rise when food was")
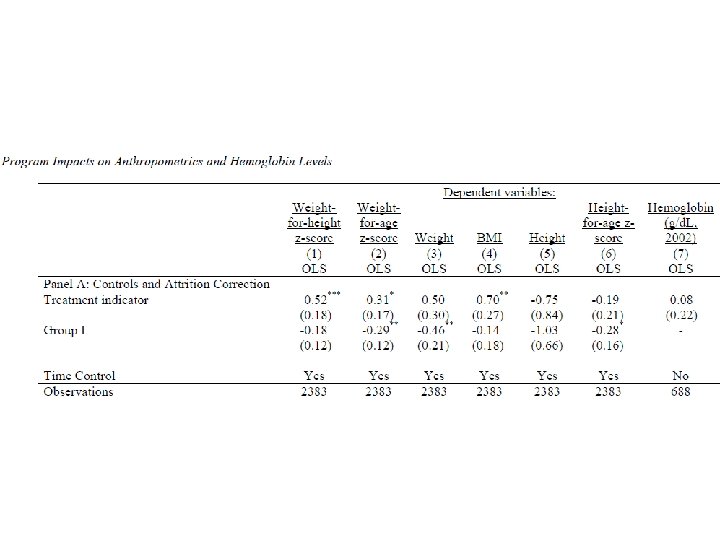
Das et al. (2013) • “Hemoglobin concentrations showed a significant rise when food was fortified with vitamin A, iron and multiple micronutrients. Fortification with zinc had no significant adverse impact on hemoglobin levels. Multiple micronutrient fortification showed nonsignificant impacts on height for age, weight for age and weight for height Z-scores. ”

• Mass fortification involves foods that are widely consumed, such as wheat, salt, sugar; targeted approaches fortify foods consumed by specific age groups like infant complementary foods; and the market-driven approach is when a food manufacturer fortifies a specific brand for a particular consumer niche. • Food vehicles commonly used can be grouped into three broad categories: staples (wheat, rice, oils), condiments (salt, soy sauce, sugar), and processed commercial foods (noodles, infant complementary foods, dairy products).

• Examples: Iron-fortified wheat, vitamin-A, vitamin-D and calcium enriched milk, iodinefortified salt.

Public policy question • Suppose the government is choosing a vehicle for iron and it has two options: • Option 1: Ask companies to mix it in with milk and milk products • Option 2: Ask companies to mix it in with condiments (curry powder, fish sauce and soy sauce) What will you take into account when deciding the vehicle?

• Approximately 40% of children are anemic across various African and Asian countries. • Iron deficiency anemia leads to weakness, poor physical growth, a compromised immune system, and is also thought to impair cognitive performance and delay psychomotor development. • Bobonis, Miguel and Sharma evaluate the impact of a project in the slums of Delhi, India, which delivers iron supplementation and deworming drugs to 2 -6 year old preschoolers.

• It is hypothesized that iron supplementation could generate school participation gains through two mechanisms: • Improved physical activity (motor development and overall decreased morbidity) • Cognitive development.

Bobonis, Miguel and Sharma • They find substantial gains in child weight – roughly 0. 5 kg (1. 1 lbs. ) on average – in the treatment schools relative to control schools. • Average preschool participation rates increased sharply, by 5. 8% points, among assisted children, reducing preschool absenteeism by one fifth. • Gains were especially pronounced for those most likely to be anemic at baseline, particularly for girls and children in low socioeconomic status areas.

• Technology or Information?

• As many as one billion people in the world drink unsafe water, and over two million deaths from diarrhea are estimated to have occurred in 1998, mainly among children. • People drink unsafe water because they are not informed about the risks to their health and because they lack access to safe water. • Providing information is a less expensive and simpler policy than providing safe sources of water. • Therefore, it is important to know if and when information alone can induce people to seek safe water with their own resources.

Madajewicz et al. • One-third or more of the wells in Bangladesh have arsenic concentrations above the Bangladeshi safety standard of 50 micrograms per liter, which can cause a variety of potentially lethal health problems. • The authors tested the water in wells in a district of Bangladesh, labeled the well as safe or unsafe and reported the result to the users of the well. • They also organized discussions about the dangers of drinking unsafe water. • Households in control areas, in which they did not provide information, were also exposed to information about arsenic disseminated by the government through TV, radio and newspapers.

Madajewicz et al. Role of Information • 60% of people who learn that the well they used before the information campaign is unsafe change to another well within one year. • Only 14% of people whose baseline well is safe change, and only 8% of people change in control areas. • Those who change to another well increase the time they spend walking for water fifteen-fold, by 4. 3 minutes for a round trip. (The opportunity cost of time is likely to be the main cost borne by those who change to a neighbor’s private well or a community well. )
")
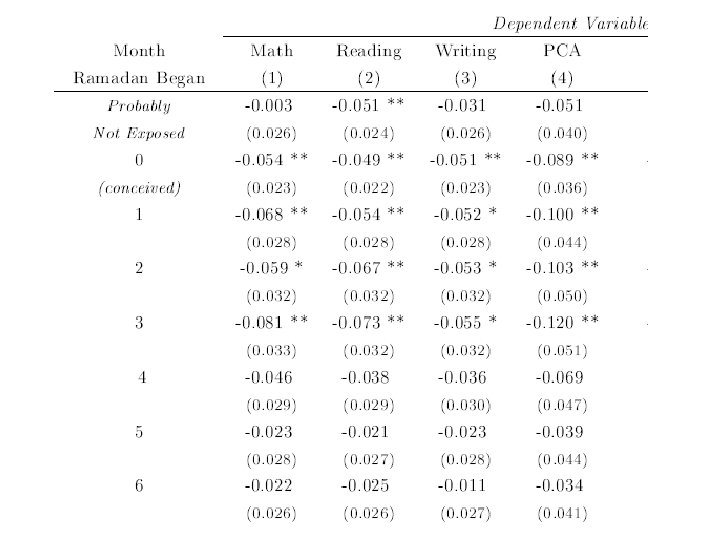
Dupas (2011)
")
Dupas (2011)

Demand-side incentives

PROGRESA • PROGRESA began in 1997 as a national program in Mexico designed to address the immediate needs of extreme poverty and break its intergenerational transmission. • Over its first three years, PROGRESA extended benefits to approximately 2. 6 million families in 50, 000 rural villages, which is about 40 percent of rural families and 10 percent of all families in Mexico. • PROGRESA conditions cash transfers (typically about 20 -30% of household income) on children’s enrolment and regular school and clinic attendance. It also includes nutritional supplementation for children up to age 5, and pregnant and lactating mothers.
 • Evidence indicates that PROGRESA has led to significant increases in")
PROGRESA (cont. ) • Evidence indicates that PROGRESA has led to significant increases in the school attendance of boys and girls that are accompanied by a significant reduction in the participation of boys and girls in work activities. • The program has a lower impact on the incidence of work for girls relative to boys. • There seems to be a significant improvement in the health of children in response to PROGRESA. • Moreover, the effect of the program seems to increase the longer the children stay on the program, suggesting that program benefits are cumulative.

Results from PROGRESA

What would happen if CCT was replaced with UCT?

• CCT most effective at getting parents to invest in outcomes/children they normally would not • Conditionality pushes parents to enroll the “marginal child”—those not enrolled at baseline, girls, young children, low ability children • CCT & UCT same impact for children enrolled at baseline, boys, older children, higher ability children
 • Immunization is a highly cost effective way of improving")
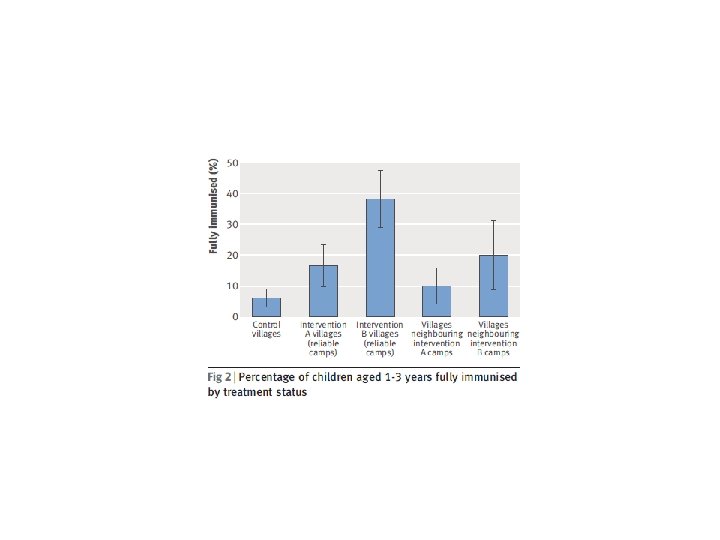
Banerjee et al. (2010) • Immunization is a highly cost effective way of improving survival in children in developing countries. • However, every year throughout the world an estimated 27 million children and 40 million pregnant women do not receive the basic package of immunizations, and two to three million people die from diseases that can be prevented with vaccines. • Reliable supply of free immunization services and incentives to improve the demand for these services could improve immunization rates.
, regular, wellpublicized immunizations were held, while in the")
• In one intervention (A), regular, wellpublicized immunizations were held, while in the second intervention (B), similar camps were held and parents were also offered 1 kg of raw lentils per immunization administered and a set of thalis (metal plates used for meals) on completion of a child’s full immunization worth 80 cents.


• Is it worth it?
")
• Calculate VSL (Value of Statistical Life)

• Suppose that the increased risk of death on a job is 1 in 10, 000 compared to a job with no observable job-related death, and that a worker is paid an additional $0. 35 per hour for accepting this risk. • Assume the worker works 2, 000 hours per year (40 hours per week times 50 weeks), so that $0. 35 x 2, 000 = $700 per year in wages is paid to the worker for death risk. • Since the expectation is that 10, 000 people would be paid this additional $700 per year in wages per one death, the statistical value of life is given by the total marginal wages earned ($700 x 10, 000 = $7, 000) per death.

• VSL of a child in India = $500000 • Cost of one immunization with incentive = $5 • As long as probability of survival is increased by 0. 001%, it’s worth it!

Why did a small incentive make such a big difference?

Some conclusions • Lack of information could be an important factor. • What information is provided and to whom. • Although information can make a difference, it is often not sufficient to achieve optimal health behavior. • Complementarities? • Small incentives may have a disproportionate impact on take-up of health behaviors. Need a persistent “push” that can move them out of their inertial state. • Even though people would like to save or adopt healthy behaviors in the long run, they might not be willing to sacrifice consumption or pleasure today.

Initial conditions matter • Growing realization that early life conditions can have a profound impact on later life.

Barker Theory • Barker and his colleagues found that malnutrition at a very early age (in utero and in infancy) in Britain resulted in earlier and more severe adult chronic disease. • Other studies show that iodine deficiency during pregnancy affects fetal brain development at a critical stage and can permanently affect cognitive performance. • Preventive measures should begin with improving the nutrition and health of women to prevent damage to their fetuses.
 finds that less educated women spend less time with their")
• Hsin (2009) finds that less educated women spend less time with their low birth weight children, while more educated women spend more time. • Smith (2009) finds that adults who were in poor health during childhood have lower earnings than their own siblings who were not in poor health. • Currie and Hyson (1999) found that low birth weight children were more than 25% less likely to pass English and math O-level tests, and were also less likely to be employed.
 find that low birth weight children are less")
• Datar et al (2010) find that low birth weight children are less likely to be breastfed, have fewer well-baby visits, are less likely to be immunized, and are less likely to attend preschool than normal birth weight siblings.

• Human capacity is inherently multidimensional, including health, cognitive, and non-cognitive components which are synergistic over the life course.
 found that prenatal iodine supplementation raised educational")
• Field, Robles, and Torero (2009) found that prenatal iodine supplementation raised educational attainment in Tanzania by half a year of schooling, with larger impacts for girls.

• The recent “fetal origins” literature in economics finds substantial effects of prenatal health on subsequent human capital and health. • Policy implications?

Summary of solutions for improving health • Role of information (level of arsenic, nutritious recipes) • Role of incentives (cars, lentil, cash) • Role of technology (deworming drugs, ITNs, iron supplements, vitamin pills, iodized salt) • Role of supply-side (employing for discovery, teaching, distribution)

Moral hazard • Suppose introduction of bicycle insurance leads to more bike thefts. Why would this happen?

• If no insurance is available, consumers have an incentive to use locks • Note the tradeoff: too little insurance means that people bear a lot of risk, too much insurance means that people will take inadequate care.

• What does this imply about the types of insurance contracts that will be offered? • They will want the consumer to face some of the risk (eg. deductibles)

• Is there a moral hazard problem in public health care?

Health care supply

• How to motivate public sector health workers?

• When effort is contractible, providing efficient incentives is trivial. But, in the more realistic case where there is hidden action (moral hazard), one of the keys to successful personnel practices is to design incentives for employees. • When effort is not contractible, one way to get the socially efficient level of worker effort is to pay the worker the full value of output. • The base salary will need to be negative – that is, the worker will pay the firm for the right to work there – in order for the firm to find the employment arrangement profitable. • Make employees the residual claimants on their effort.

• Worker output may be imperfectly related to inputs • Risk aversion

• Tournaments • First, prizes are fixed in advance and depend on relative rather than absolute performance. • Second, larger spreads in wages at different levels of the hierarchy • An important variable in the Lazear and Rosen (1981) model is the amount of noise – that is, to what degree luck affects the probability of winning. When there is more noise (so that luck becomes relatively more important and effort relatively less important), workers will try less hard to win because effort has a smaller effect on whether or not they win. • In production environments that are very uncertain, large raises must be given in order to offset the tendency by workers to reduce effort

Monitoring and Shirking of workers • Between 1924 and 1927 the level of lighting was systematically changed for experimental groups in different departments (Mayo, 1933) at the Western Electric Company plant in Hawthorne.

Performance pay to motivate workers • The incentive effect arises because pay-forperformance schemes increase the marginal benefit of effort, which leads employees to work harder, other things equal. • The selection effect arises because high-ability employees who are capable of achieving high performance can achieve higher pay and are, thus, attracted by schemes that reward performance, other things equal.

• The increase in pay inequality can reduce workers’ morale and lead to sabotage, or the change in the composition of the peer group due to the selection effect might affect workers’ behavior over and above the effect of the compensation scheme. • Identifying selection effects poses a difficult challenge for field experimenters – it requires information on the entire pool of potential employees and – time horizon of field experiments is short

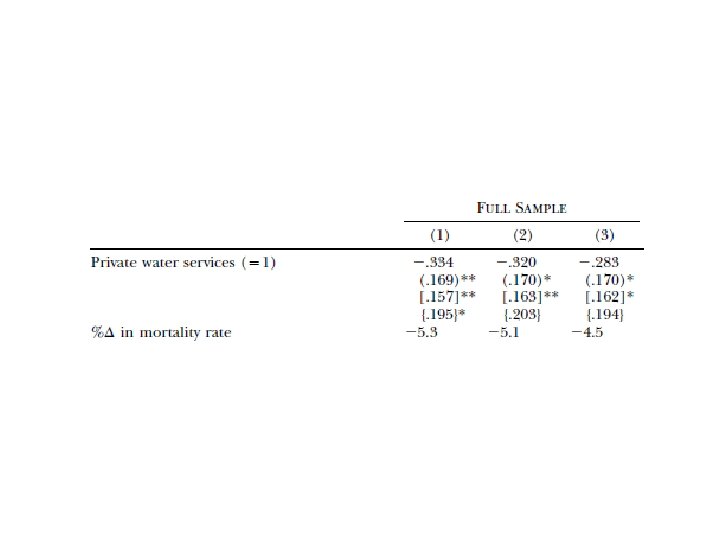
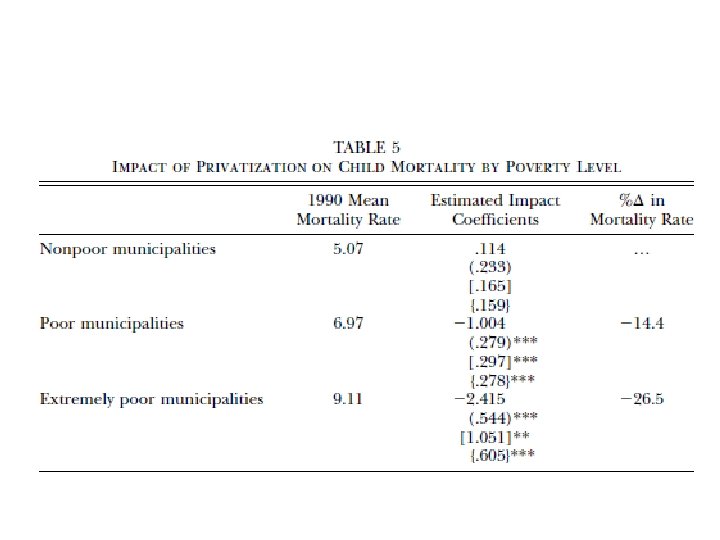
• Governments that want to privatize water systems are typically motivated by potential efficiency gains. They hope that these efficiency gains will be translated into expanded access and enhanced service quality, and thereby improved health outcomes.
 • Private water companies may provide suboptimal levels of service")
Galiani et al. (2005) • Private water companies may provide suboptimal levels of service quality because they fail to take into account the significant health externalities that are present in this industry. • In this case, privatization of water services may affect health outcomes negatively. • Privatization may hurt the poor through price increases, enforcement of service payments, and investment only in lucrative high income areas.

• Public programs can often crowd-out private behavior • Vaso de leche program in Peru • Mid-day meal program in India

Malaria in Eritrea

• Increase in supply could happen by building more clinics, hiring more workers • Perhaps the bigger problem is inefficiency or moral hazard • Possible solutions? Better monitoring, better selection, Performance Pay, Privatization • Need to be careful about a demand-side crowding-out effect of an increase in supply of health care services

• Often demand-side is modeled as a household but household can have members with different objective functions that may sometimes conflict with one another

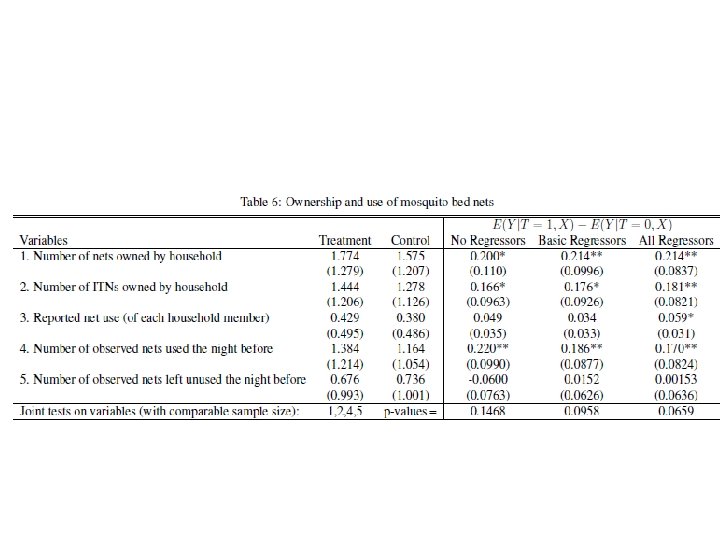
• Programs also need to be sensitive to whom they are targeting within the household and for what • Dupas (2009) randomly varied who in the household was targeted by a promotion campaign for antimalarial bed nets in western Kenya. • Households received a voucher for a bed net at a randomly chosen price. The gender of the household head that received the voucher, as well as a marketing message, was randomized: Either the female head alone, or the male head, or both heads were targeted. Women were not more likely to purchase the bed net, and they did not appear to be less price elastic than men. • Handing out the voucher in the presence of both household heads increased take-up by about 7 percentage points (20%) compared with targeting either of them alone.
 • Women were randomly selected to receive the voucher either")
Ashraf et al. (2010) • Women were randomly selected to receive the voucher either in private or in the presence of their husbands, giving the former greater facility to conceal take-up of contraception from their husbands as the husbands did not receive information about concealable forms of contraception. • The study results suggest that intrahousehold discordance over family planning plays a significant role in contraceptive use and fertility outcomes. When women were given greater opportunity to hide birth control (i. e. , the private treatment), they were 23% more likely to visit a family planning nurse and 38% more likely to adopt a concealable form of contraception, leading to a 57% reduction in unwanted births.

• Spillovers between households may also play a role in adoption of behavior (malaria, HIV, recipe books)

Health and Behavioral Economics

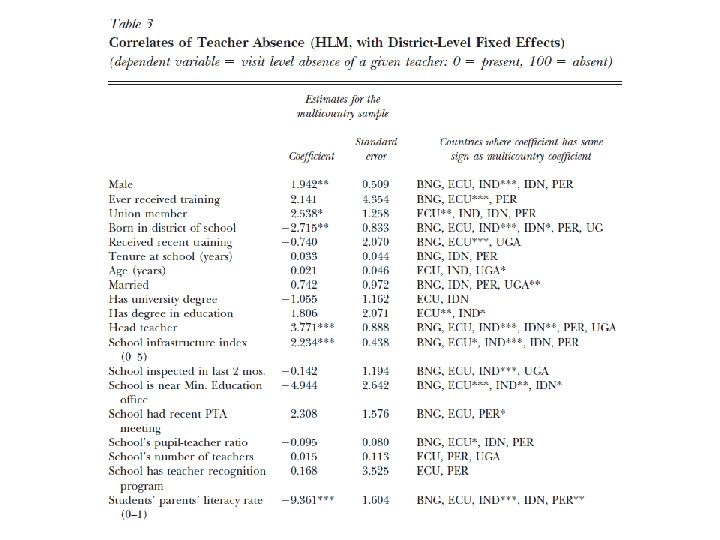
• Puzzle #1: High absenteeism in health clinics in developing countries • And when doctors are present, there is overmedication. • In Rajasthan, India, Banerjee et al. (2004) find that only 3% of patients at public health facilities have at least one diagnostic test performed on them, but 38% nevertheless get prescribed an injection or a drip.

• Ultimatum Game • Two players are provisionally allocated a pie to split. The first-mover offers a share to the second-mover who accepts or rejects the offer.

• Most of the data from developed countries support the norm of conditional reciprocity in which the two parties see the relationship more as a partnership in which both players accrue profit. • Accepted offers are implemented and rejections result in both players receiving nothing. • The mean offers are around 40% and low offers are routinely rejected which suggests that fairness norms are enforced.

• Puzzle #2: People respond to small incentives to get their children immunized • Conversely, when people have to pay for preventive care, they run away! • Cohen & Dupas (2010) find that pregnant women universally take up an antimalarial bed net when it is given for free during a prenatal visit, but only 40% buy one at the still highly subsidized price of US$0. 60. In Zambia, Ashraf et al. (2010 a) find that take-up of a water-treatment product drops from 80% to 50% when the price increases from US$0. 10 to $0. 25.

• Poor less likely to take preventive medicines but not likely to have low health expenditure: Using detailed diaries kept by rural households in Dupas & Robinson (2009) find that health expenditure represents 8% of total household expenditure. In the US, out-of-pocket health expenditure is considered unaffordable if it is more than 5% of family income

• Perhaps, there is lack of trust about immunization?
: The first-mover is given the chance to")
Trust and Reciprocity • Trust game (TG): The first-mover is given the chance to send as much of her endowment to an anonymous second-mover as she wishes. The experimenter triples the amount of money sent so that sending money is socially efficient. The second-mover then sends back as much he wishes.
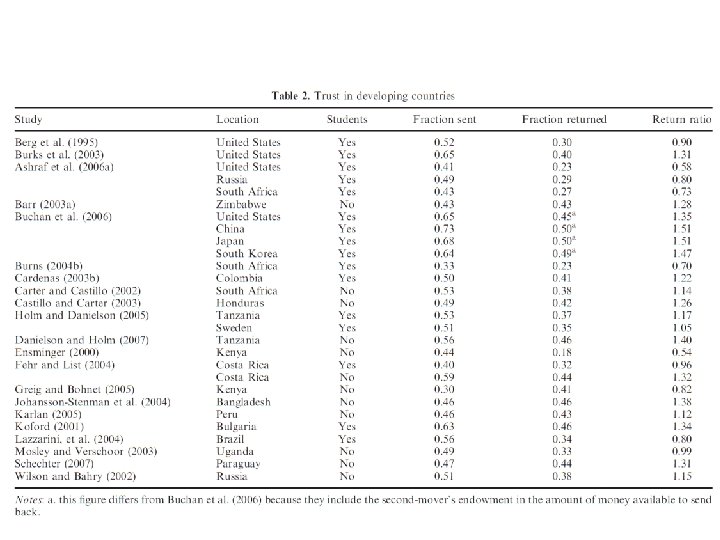

• Despite this prediction, on average, first-movers send 50 per cent of their endowment and second -movers return 30 per cent of what they receive. • Burks et al. (2003) finds that investing pays off (31% average return) when there is a homogenous student population

• Clearly, second-mover behaviour in the TG measures trustworthiness or reciprocity, more generally; however, first-mover behaviour might be harder to interpret. • That is, to what extent do first-movers see their transfer as a donation without any expectation of a return? • Dictator game – removes the self interest effect to get only the effect of altruism • Assuming that trust and altruism are additively separable, then pure trust is just the difference between the transfer in the TG and that in the DG • Also, positive correlation between level of trust according to the Trust Game and the trustworthiness measured by World Values Survey
 shows that, controlling")
Presence of altruism • Using data from rural India, Townsend (1994) shows that, controlling for village consumption, episodes of sickness among a given household do not affect consumption for that household. Robinson & Yeh (2011 a), looking at women who supply transactional sex in western Kenya, show that transfers from regular clients (partners) increase by 37%. 42% when a woman is sick.

Camerer’s comment on Mullainathan

CNBC, 9 June 2014 • The latest National Retirement Risk Index from the Center for Retirement Research (CRR) at Boston College says that more than half (53 percent) of households risk falling more than 10 percent short of the retirement income they'll need to maintain their standard of living. • More than 40 percent of retirees are also at risk of running out of money for daily needs, out-ofpocket spending on health care or long-term care, according to the Employee Benefit Research Institute (EBRI).
 Discounting of future")
Another solution to Puzzle 2 • Delta Discounting versus Beta-Delta (Hyperbolic) Discounting of future

• Hyperbolic discounting • Choose $10 today or $11 tomorrow • Choose $10 one year from now or $11 one year and one day from now.
 at one of the")
Quiz question • You need to buy malarial bednets (ITNs) at one of the three times available. That is t ∈ {0, 1, 2} and the costs associated with paying for the bednets at the three times are c 0 = 1, c 1 = 1. 5, c 2 = 2. 5. Take β = 1/2 and δ = 1. • Take Self 0 (the decision maker at time 0). • What is the disutility of doing the task at times 0, 1 and 2 assuming our payoffs or costs are discounted by β and δ? • When would Self 0 decide to undertake the task? Would he accomplish the task in the period he decides to undertake the task?

• The disutility at 0 is 1, at 1 is 0. 75, at time 2 is 1. 25. • Self 1 compares time 1 cost of 1. 5 with time 2 cost of 1. 25 and prefers the task to be done at time 2. Self 2 does the task at the cost 2. 5.

• Puzzle #3: The poor often fail to take their medications for HIV, diabetes, tuberculosis • The poor in the US are more obese • The poor are less likely to get their children vaccinated, wash their hands or treat their water

• Part of the solution is access and cost • However, poor on Medicaid pay nothing, yet they fail to take medicines

• Poor are not just short on cash, they are short on bandwidth (Mullainathan and Shafir, 2013) • Nearly every advanced cognitive function relies on bandwidth • Taxes working memory, makes us less productive • Information campaigns are least likely to work on the poor!

• Also fewer resources to exert self-control

• Self-control problems • Scratching a rash, eating chocolate, smoking, overspending, procrastination • No-bite nail polish and Disulfiram- Those who want to stop biting their nails can buy bitter nail polishes. Disulfiram is an extreme version of this concept. It is given to alcoholics, and it causes them to throw up and suffer a hangover as soon as they start to drink. • Quit smoking without a patch- CARES is a savings program offered in the Philippines, in which a would-be non-smoker opens an account with a minimum balance of one dollar. For 6 months, she deposits the money she would otherwise spend on cigarettes into the account. After 6 months, the client takes a urine test to confirm that she has not smoked recently. If she passes, she gets her money back. If she fails, the account is closed and the money goes to charity. Early results look very good.


- In a psychology experiment, participants were asked to remember either a short two digit number or a seven digit number and then to walk down a hallway to another room for an interview. - As a seeming afterthought, they were told there is a snack cart in the hallway and to help themselves to either fruit salad or chocolate cake. - The subjects asked to remember the two-digit number selected the chocolate cake 37% of the time.

- The subjects tasked with remembering the longer seven digit number overwhelmingly chose the chocolate cake 59% of the time. - The repeated trade-offs confronting the poor in daily decision making – i. e. “should I purchase a bit more food or a bit more fertilizer? ” – occupy cognitive resources that would not bother the wealthy when confronted with the same decision. Shiv and Fedorikhin (1999)

• The role of savings

Psychology of Savings • Duflo, Kremer and Robinson found that only 40% of farmers in a region in Kenya had ever used fertilizers even though the average annual return to using fertilizer exceeded 7% • When asked why they weren’t using fertilizers, farmers said they did not have enough money on hand to buy fertilizer when it was time to use it • Saving at home is difficult • Purchasing fertilizer in advance increased the fraction of farmers who used fertilizers by at least 50%

• Time-inconsistency - The vision of how we should act in the future is often inconsistent with the way we will act in the future. • Many of the ways the poor save seem to be intended not only to keep money safe from others, but also to guard it from themselves. • Paradox - there are ways to get around selfcontrol problems, but to make use of them usually requires an initial act of self-control.

• Microfinance and ROSCA as a solution to health problems

Microfinance Game • Consider two players: Alpha and Beta. Alpha moves first. • At the start of the game, Alpha has two piles of coins in front of her: one pile contains 4 coins and the other pile contains 1 coin. • Each player has two moves available: either "take" the larger pile of coins and give the smaller pile to the other player or "push" both piles across the table to the other player. • Each time the piles of coins pass across the table, the quantity of coins in each pile doubles. For example, assume that Alpha chooses to "push" the piles on her first move, handing the piles of 1 and 4 coins over to Beta, doubling them to 2 and 8. Beta could now use his first move to either "take" the pile of 8 coins and give 2 coins to Alpha, or he can "push" the two piles back across the table again to Alpha, again increasing the size of the piles to 4 and 16 coins.

• An overwhelming majority of Rosca participants are women, who are typically also married and earn an independent income. (Anderson and Baland, 2002) • Rosca funds in Kenya are typically spent on school fees, household items, food, medicines, small business (Gugerty, 2007) • Roscas are immensely popular but what is their attraction? They often pay no interest. In fact, given the potential for default (those who received the pot early may stop paying in), they may effectively pay a negative interest rate.
 • Seductresses who lured nearby sailors with their enchanting")
• Sirens (Greek mythology) • Seductresses who lured nearby sailors with their enchanting music and voices to shipwreck on the rocky coast of their island. • Many ROSCA participants “bind their hands” through the use of a pre-commitment mechanism (mast) in which participants agree in advance on how they will use their funds and the group monitors the individual to ensure that she honors her commitment.

• One reason for their popularity may be that they serve as a commitment device in several ways. By making savings a public act, they allow social pressure from other Rosca members to commit them to their desired savings level (Ardener and Burman 1995). • Responses to the question of why individuals joined a Rosca: - “You can’t save alone—it is easy to misuse money. ” - “You cannot trust your husband. If you leave money at home, he will take it. " - “Sitting with other members helps you to save. ” (Gugerty, 2007)
 • They offer depositors at a bank")
• Ashraf, Karlan and Yin (2004) • They offer depositors at a bank in the Philippines the opportunity to participate in “SEED” accounts. • These accounts are like deposit accounts, except individuals cannot withdraw deposits at will. • Instead, they can only withdraw the money at a pre-specified date or once a pre-specified savings goal has been reached. This account does not pay extra interest and is illiquid. • In most economic models, people should turn down this offer in favor of the regular accounts offered by the bank. Yet they find large demand for them. More than 30% of those offered the accounts take them up. They also find these accounts help individuals to save. Six months later, those offered the accounts show substantially greater savings rates

www. Stickk. com - With financial commitments, an individual puts up money and agrees to accomplish a certain goal by a certain date, and also specifies how to verify his accomplishment. If he fails, the money goes to charity. - Non-financial commitments include peer pressure (emails to family or friends) and monitoring one’s goal via a group blog - Similar to a Self-help group

• Paying tuition fees at the start as a commitment device for studying regularly • “Paying upfront every month really gets me to go to the gym. ” • What about group meetings stressed by Selfhelp groups?
 • Examine the impact of cigarette taxes. • Under the")
Gruber and Mullainathan (2002) • Examine the impact of cigarette taxes. • Under the rational model, smokers are made worse off with these taxes. This is a standard dead-weight loss argument. • Smokers who would like to smoke cannot now because of the higher price. • Smokers who wanted to quit, but were unable to due to the inability to commit, are now better off. • Taxes serve as a commitment device.
 form dynamically consistent plans.")
• Sophisticated people would recognize the inconsistency and (recursively) form dynamically consistent plans. In other words, they would only make plans on which they would follow through. • On the one hand, individuals appear to consciously demand commitment devices, to help them commit to a particular path. On the other, they appear to have unrealistic plans. • Limbic system (experiential, fast, unconscious, now) versus Prefrontal cortex (forward looking, creative, logical, slow)

Summary • Malaria, respiratory infections, diarrhea, AIDS, and other diseases are estimated to kill more than • 15 million people each year, most of them children. Yet the great majority of these diseases can be prevented or treated.

• Disease burden affects people at much younger ages than the disease burden in developed countries, and its main channels of morbidity and mortality are infectious and parasitic diseases, which generate important public health externalities. • However, there has been progress on reducing child mortality

• Sleeping under a bed net prevents malaria, treating drinking water prevents waterborne diseases, taking deworming pills gets rid of intestinal worms, and using condoms prevents HIV. • The bad news is that take-up of these strategies is often slow. • Adoption of product may not lead to adoption of behavior

• • • Role of technology Role of information Demand-side incentives/mandates Supply-side expansion or incentives Time-inconsistent preferences
- Slides: 162