Health Disparities Why we have not solved the
















: An example")
 •")


- Slides: 22
Health Disparities Why we have not solved the problems Why we need new approaches Bill Jenkins, Ph. D. , M. P. H. The Research Center on Health Disparities Morehouse College
• Why we have not solved the problems of Health Disparities?
Infant Mortality Rates by Race: United States, 1915 -1997* *Note: For years 1915 -1960, “White” included persons stated to be “White, ” “Cuban, ” “Mexican, ” or “Puerto Rican. ” All others during that time period were referred to as “Nonwhite. ”
Black-White Ratio of Infant Mortality, United States: 1915 -1997* YEAR *Note: For years 1915 -1960, “White” included persons stated to be “White, ” “Cuban, ” “Mexican, ” or “Puerto Rican. ” All others during that time period were referred to as “Nonwhite. ”
A Model of Health Disparities 30 -30 -30 Socio-Economic Factors + 30 Percent Racism Factors + 30 Percent Cultural Factors + 30 Percent Medical Care Factors + 10 Percent Biological Factors + 1 Percent = Attributable Risk Percent
Racism • Racism remains a pervasive force in America today. Although more benign, it remains a major determinate of health and health policy in America. The most deleterious form of racism is subtle and complex as it interacts with socio-economic status, culture and a host of political and other factors – White Privilege. • There is no social force more pervasive, yet so misunderstood than racism. It creates the illusion that there is something called “Race” and then establishes assumptions to support it. So powerful a concept that even those who are disadvantaged by it, accepts it – the use of race supports racism, especially when used by African-Americans.
Racism • There is no “race” problem in America, There is a Racism problem. If you can not define a problem, you can not solve it – To many of us are afraid to use the word – • A social “construct” – not to the other 99 % of Americans. • The greatest problem using the term race it that it influences us to waste huge amounts of resources on issues which no or little chance of solving the problem: Genetics, Health care
It’s the culture - Stupid African-Americans most understand themselves and be understood by others as an ethnic group – competitive dance, • The problem of health care utilization is much less accessibility than acceptability of health care • Racial data has largely been changed to ethnic data already, but most people have noticed • Solving the problem of health disparities requires that we address the problems of Culture including issues of trust, competing risks, internalized racism….
Socio-Economic Status • SES remains perhaps the most powerful force producing health disparities – it is massive, multi-factorial, complex. • There is no will to solve this problem head on, however there are solutions which go un - and under utilized – head start, community participatory activities
• How can we solve the problems of Health Disparities?
AIDS Case Rates per 100, 000 Population by Ethnicity: United States, 1990 -2000 *Persons of Hispanic origin may be of any race.
AIDS Rate Ratios by Ethnicity as Compared to Whites: United States, 1990 -2000 *Persons of Hispanic origin may be of any race.
Primary and Secondary Syphilis Reported Rates per 100, 000 Population by Ethnicity: United States, 1995 -1999
Primary and Secondary Syphilis Rate Ratios by Ethnicity Compared to Whites: United States, 1995 -1999
Levels of Community Participatory Research • Community notification - inform the community of the intentions of the research risks and benefits relating to the individuals and communities involved • Community endorsement - community representatives are asked to formally support the research activities • Community advice - seeking and obtaining community advice in planning, development, execution, and dissemination of the research. • Community consent - obtaining some expression of community approval. • Community origination - research purpose and goals set by expressed community needs.
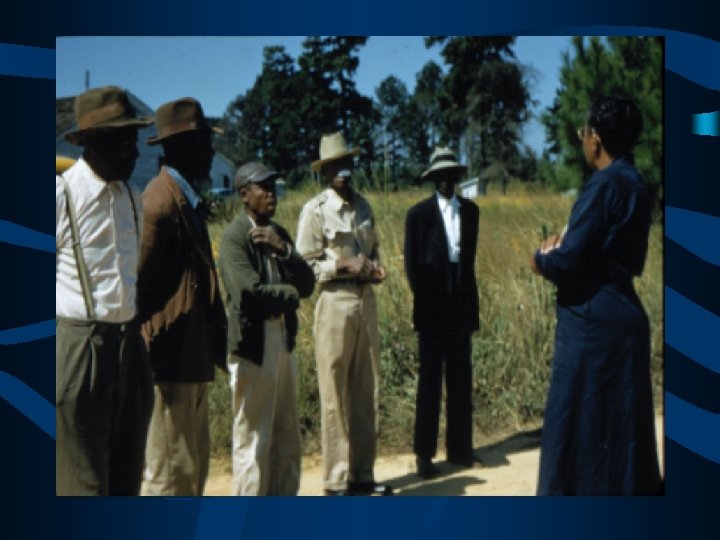
The Tuskegee Study of Untreated Syphilis in the Negro male (1932 -1972): An example of CPR • Community Notification Churches / Businesses • Community Endorsement Business Establishments • Community Advice The Tuskegee Institute • Community Consent Macon County Medical Society • Community Origination The Negro Health Movement • Cultural Competence Nurse Eunice Rivers
Barriers to CPR • Respect for Community Competencies • Willingness to share (Power) • Accepting another perspective
Things We Can Do • We can reduce the effect of SES on health through ethnic-specific interventions which include social support • We can improve our cultural competence • We can target low social capital communities; if not we increase health disparities • We can target resources to problems (less than 10% of the disparities are due to differences in health services, but more than 70% of research dollars are directed there) • We, or just one of us, can make a difference