Headache Headache Diagnosis is based on history Classification

Headache
")
Headache • Diagnosis is based on history • Classification - IHS (International headache society) – 1988 • 3 rd Edition – ICHD 3 - 2016

Headache - classification Part I - Primary headaches 1. Migraine 2. Tension-type headache 3. Trigeminal autonomic cephalalgias 4. Other primary headache disorders

Headache - classification Part II - The secondary headaches 5. Headache attributed to trauma or injury to the head and neck 6. Headache attributed to cranial or cervical vascular disorders 7. Headache attributed to non-vascular intracranial disorder 8. Headache attributed o substance or its withdrawal 9. Headache attributed to infection 10. Headache attributed to disorder of homeostasis

Headache - classification Part II - The secondary headaches 11. Headache or facial pain attributed to disorder of the cranium, neck, eyes, ears, nose, sinuses, teeth, mouth, or other facial or cervical structure 12. Headache attributed to psychiatric disorder Part III – Painful cranial neuropathies, other facial pains and other headaches 13. Painful cranial neuropathies and facial pains 14. Other headache disorder

Migraine 1. 2. 3. 4. 5. 6. Migraine without aura Migraine with aura Chronic migraine Complications of migraine Probable migraine Episodic syndromes that may be associated with migraine

Tension type headache 1. 2. 3. 4. Infrequent episodic tension-type headache Frequent episodic tension-type headache Chronic tension-type headache Probable episodic tension-type headache
 1. Cluster headache 2. Paroxysmal hemicrania 3. Short-lasting unilateral neuralgiform")
Trigeminal autonomic cephalalgias (TACs) 1. Cluster headache 2. Paroxysmal hemicrania 3. Short-lasting unilateral neuralgiform headache attacks (SUNCT) 4. Hemicrania continua 5. Probable trigeminal autonomic cephalalgia

Other primary headaches 1. 2. 3. 4. 5. Primary stabbing headache Primary cough headache Primary exertonial headache Primary headache associated with sexual activity Hypnic headache 6. Primary tunderclap headache 7. Hemicrania continua 8. New daily-persistent headache

Secondary headaches 5. Headache attributed to trauma or injury to the head and/or neck 6. Headache attributed to cranial or cervical vascular disorder stroke, brain haemorrhage, AVM, aneurysm, cerebral venous thrombosis 7. Headache attributed to non-vascular intracranial disorder CSF hypotension, CSF hypertension, brain tumors, epileptic seizures, etc. 8. Headache attributed to a substance or its withdrawal acute intoxication, using of drugs, etc. 9. Headache attributed to infection meningitis, encephalitis, etc.

Secondary headaches 10. Headache attributed to disorder of homoeostasis brain hypoxy, arterial hypertension, hypotyreosis, hunger, etc. 11. Headache or facial pain attributed to disorder of the cranium, neck, eyes, ears, nose, sinuses, teeth, mouth or other facial or cervical structure 12. Headache attributed to psychiatric disorder

Part three: painful cranial neuropathies, other facial pains and other headaches 13. Painful lesions of the cranial nerves and other facial pain trigeminal neuralgia, glossopharyngeal neuralgia 14. Other headache disorders
 •")
Headache diagnosis - based on history • characteristics • quality (sharp, blunt pulsing) • intensity • localisation • response on the physical • activity • accompanying signs Haas, D. C. , SUNY Upstate Medical University, 2002

Headache diagnosis - based on history • Accompanying signs Ø nauzea, vomitus Ø phonophoby, photophoby Ø aura ü informations about drugs which are used

Migraine is a common disabling primary headache disorder. • prevalence – 10% • • Nauzea prevalence in women • Fonofóbia 17, 5 % • Fotofóbia • • Bolesť prevalence in men 5, 7 % Unilaterálna Pulzujúca • positive familial Provokovaná history aktivitou fyzickou 58 % Haas, D. C. , SUNY Upstate Medical University, 2002

1. 1 Migraine without aura – 80% • A. B. C. Diagnostic criteria: At least five attacks 1 fulfilling criteria B-D Headache attacks lasting 4 -72 hr (untreated or unsuccessfully treated)2; 3 Headache has at least two of the following four characteristics: 1. unilateral location 2. pulsating quality 3. moderate or severe pain intensity 4. aggravation by or causing avoidance of routine physical activity (eg, walking or climbing stairs) D. During headache at least one of the following: 1. nausea and/or vomiting 2. photophobia and phonophobi E. Not better accounted for by another ICHD-3 diagnosis.

1. 2 Migraine with aura – 18% • Diagnostic criteria: A. At least two attacks fulfilling criteria B and C B. One or more of the following fully reversible aura symptoms: 1. 2. 3. 4. 5. 6. visual sensory speech and/or language motor brainstem retinal

1. 2 Migraine with aura – 18% C. At least three of the following six characteristics: 1. 2. 3. 4. 5. 6. at least one aura symptom spreads gradually over ≥ 5 minutes two or more aura symptoms occur in succession each individual aura symptom lasts 5 -60 minutes 1 at least one aura symptom is unilateral 2 at least one aura symptom is positive 3 the aura is accompanied, or followed within 60 minutes, by headache D. Not better accounted for by another ICHD-3 diagnosis.

1. 4 Complications of migraine • • Status migrainosus Persistent aura without infarction Migrainous infarction Migraine aura-trigerred seizure

Pathophysiology of migraine • Hypotalamus and limbic system prodroms • Neuronal dysfunction and vascular changes aura and headache

Pathophysiology of migraine • Spreading depression of CBF from occipital region during aura • Spreading depression activate trigeminovascular endings

Pathophysiology of migraine • It is unknown mechanism of activation nuclei in brainstem (nc. caudalis trigeminalis) - by spreading depression - by biochemical chnages - both Activation stimulate perifepheral findings of n. V.

Pathophysiology of migraine • Stimulation of n. V. lead to release of substance P and neurokinin A neurogenic inflammation

Pathophysiology of migraine • Stimulation of serotoninergic cells – increased blood flow and vasodilatation • Sleeping – reduce releasing of 5 -HT - Sleeping treat migraine

Pathophysiology of migraine • Receptors 5 -HT are different activation of inhibting 5 -HT 1 B/1 D receptors release of serotonin, substance P, neurokinin block neurogenic inflammation • receptors agonists – triptans – treatment of migraine (triptans)

CGRP - neuropeptid involved in pathophysiology of migraine Potent vasodilatator Increased level during headache CGRP = calcitonino gene related peptid Goadsby PJ, et al. Ann Neurol. 1990; 28: 183 -187. . 5. Cernuda-Morollón E, et al. Neurology. 2013; 81: 1191 -1196.

Binding of m. Abs determines their therapeutic effects Ligand-receptor interaction m. Abs blocking ligand (CGRP) m. Abs blocking receptor Ligand (other than CGRP) CGRP RAMP 1 CLR CGRP primarily binds its receptor under normal conditions RAMP 1 § § CGRP is neutralized Other ligands may interact with the CGRP receptor CLR RCP RCP § CLR CGRP § § Receptor interaction is impeded CGRP and other ligands may bind other receptors Figure adapted from Pellesi L, et al. Clin Pharmacol Drug Dev. 2017. 216 CLR = calcitonin receptor-like receptor; RAMP 1 = receptor activity-modifying protein; m. Abs = monoclonal antibodies; RCP = receptor component protein. 216. Pellesi L, et al. Clin Pharmacol Drug Dev. 2017. doi: 10. 1002/cpdd. 345.

CGRP

Migraine • Nauzea • Phonophoby • Photophoby • Pain Unilateral Pulsating Provoke by physical activity Lasts 4 – 72 hodín Haas, D. C. , SUNY Upstate Medical University, 2002
 • Dietetical (alcohol, Na glutamat,")
Factors provoke atack of migraine • Hormonal (menstruation, kontraceptives) • Dietetical (alcohol, Na glutamat, chocolate, cheese) • Psychological (stress, anxieta, depression) • From environment (odors, changes of weather, high above sea-level) • Drugs ( NTG, histamin, reserpin, estrogens) • Others (head injury, physical activity)

Migraine with aura • Aura - visual sensoric afasic motoric IHS – lasts: 4 – 60 min. (70% do 30´)

Migraine with aura • Visual aura scintilating scotoma small point is enlarging to cik-cak border (scintilation), in the middle is dark scotoma Haas, D. C. , SUNY Upstate Medical University, 2002

Migraine with aura • Visual aura colloured scintilating scotoma Haas, D. C. , SUNY Upstate Medical University, 2002

Migraine with aura • Positive fenomenons cik-cak • Negativ scotoms Haas, D. C. , SUNY Upstate Medical University, 2002)

1. 6. Compliations of migraine • 1. 6. 1. Status migrenosus headache lasts more than 72 hours • 1. 6. 2. brain infarct neurological deficit is not reversible till 7 days and/or infarct on CT or others

Auxiliary examination Radiological Ø Different headache Ø Daily headache Ø Headache + neurological signs Ø Headache not responding on treatment Ø Posttraumatic headache

Auxiliary examinations Radiological • To exclude brain tumor for patient • CT-native , with contrast medium • MRI, MR angiography, • angiography

Auxilliary examinations • Elektroencephalography • X-ray of skull injury, TU • X-ray of cervical spinal column

Auxilliary examinations • Duplex ultrasound of carotid arteries, Transkranial Doppler • Optic fundus GLAUCOMA

Migraine - therapy • • • ASA Paracetamol + ASA + coffein Ibuprofen Naproxen Triptans (eletriptan, naratriptan, rizatriptan, sumatriptan, zolmitriptan) – middle or severe attacks of headache

Migraine - therapy • Triptans Sumatriptan Zolmitriptan Naratriptan Rizatriptan Eletriptan dose max. d. 25 -50 -100 mg 300 2, 5 – 5 mg 10 2, 5 mg 5 5 – 10 mg 30 40 - 80 mg 160

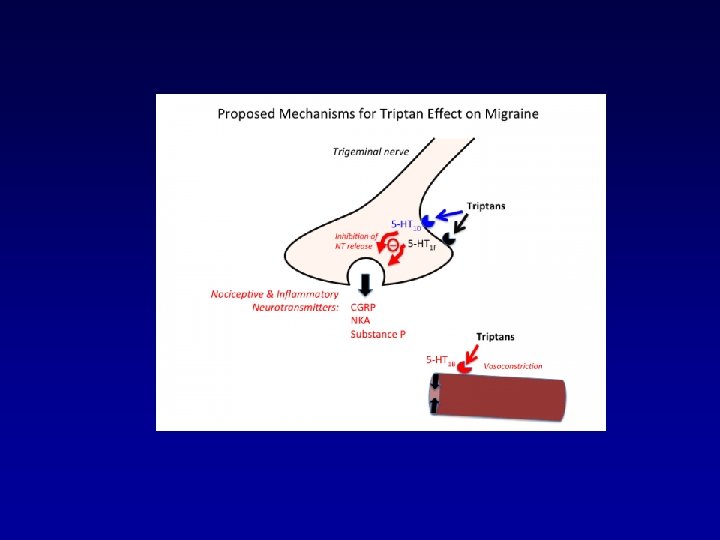
Migraine – therapy mechanism of triptans • Vasoconstriction of meningeal, cerebral, pial vessels activation 5 -HT 1 B receptores in smooth muscles of vessels • Inhibition of neurogenic inflamation stimulation 5 -HT 1 D receptores at the endings of trigeminal C and A fibers (subst. P, neurokinín A, CGRP) • Central inhibition of pain activation 5 -HT 1 D, 1 F receptores in brainstem decrease excitability of neurones ncl. trig. caudalis

Migraine – therapy • Prevention – more than 3 attacks/month betablockers, blockers of calcium, chanels, antiepileptics – topiramat, valproid acid pizotifen

Monoclonal antibodies against CGRP receptor

Mechanism of erenumab action

Tension headache • The most often chronic headache • Prevalence - women – 88% • Prevalence – men – 69% the most days outside of work

Tension headache • Pain - around the head - nonpulsating - bilateral - 30 min. – 7 days - not increased by physical activity Haas, D. C. , SUNY Upstate Medical University, 2002

Tension headache • Increased muscle tone in the neck • Stright cervical lordosis • Therapy • Analgetics, myorelaxants, nonsteroid antiflogistics, physioteraphy, psychoteraphy, local 1% mesocain

Cluster headache • 6 times more frequent in men • Pain - periorbital - frontal, temporal - UNILATERAL - burning Haas, D. C. , SUNY Upstate Medical University, 2002

Cluster headache • Alarm-clock pain -beginning at night • Pain lasts: 15 – 180 min. shorter than migraine • Congestion • Lacrimation • Conjuctival inflamation • Therapy • O 2, triptans, DHE

Chronic paroxysmal hemicrania • More often in women • Pain – unilateral - lasting: 2 – 45 min. - more times during the day - ipsilateral lacrimation, conjuctival inflammation - nasal congescion, rhinorea - ptosis • Effect of Indometacin – dg. test

Pain Migraine Tensiion headache Cluster headache Localisation Unilateral Bilateral Unilateral Lasting 4 – 72 hours Hours days 30 – 180 min Intensity Light severe Light middle Severe Nauzea, phono-, photophoby Lacrimation, nasal congestion YES No No (could be) It could be No YES

Subarachnoid haemorrhage • Sudden onset of the strong headache • Immediatelly to hospital HOSPITAL

Trigeminal neuralgia • Etiology – focal demyelinisation of n. V. or of ganglion • Idiopatic – pulsations of arteries near n. V. • Symptomatic – tumors • Prevalence – 6/100000, more women, and older people

Trigeminal neuralgy • Clinical feature shooting pain in area of n. V. , increasing after chawing, in symptomatic - trigger area, loose of weight • Therapy anticonvulsants – Gabapentin, alcoholisation of ganglion, surgery

Temporal arteriitis • Inflammation of a. temporalis superficialis • Age – risc factor • Headache in temporal region, thick, painful temporal superficial artery, chawing claudications, stronger pain polymyalgia reumatica – spasm and pain of masticatory muscles

Temporal arteriitis • Late diagnosis– risc of blindness and stroke • Dg. – laboratory – FW, CRP, AG, biopsy • Therapy – Prednison – 60 (100) mg/day long time, after decreasing – control of FW, FW – back to former dose

Conclusion • Headache – one of the most often symptoms • Correct differential diagnosis correct therapy shortened headache improving quality of life economical profit, shortened working inability
- Slides: 59