Head and Neck Examination Yasar Kucukardali MD Professor



 - tower shape skull Dolichocephalia")





. Technique")





- Slides: 67
Head and Neck Examination Yasar Kucukardali, MD Professor Yeditepe University Medical Faculty Department of Internal Medicine
INTRODUCTION • The HEENT, or Head, Eye, Ear, Nose and Throat Exam is usually the initial part of a general physical exam, after the vital signs. • it begins with inspection, and then proceeds to palpation. It requires the use of several special instruments in order to inspect the eyes and ears, and special techniques to assess their special sensory function.
LEARNING OBJECTIVES • Identify anatomic landmarks of the head, neck, ear, nose mouth and throat. • Describe the physical examination techniques for routine evaluation of the head, neck, eye, ear, nose and throat. • Describe normal findings of the head, neck, ear, nose and throat exam.
We recognise the following head shape variations: Turicephalia (oxycephalia) - tower shape skull Dolichocephalia - skull elongated backwards Brachycephalia - generally shortened Microcephalia - diminished skull due to premature closure of the cranial sutures • Macrocephalia - enlarged skull, in hydrocephalus in childhood • Asymmetric - due to meningocele or bumpy in Paget disease • •
ANATOMY OF THE EYE External eye: Eyelids, lacrimal gland duct, palpebral fissures, medial and lateral angles. Internal eye: Light travels through cornea, anterior chamber, pupil, lens, and vitreous body on the way to the retina. Fundus: The posterior structures of the eye include the retina, retinal arteries and veins, the optic disc and the macula. These structures are viewed with the ophthalmoscope.
EXAMINATION of the EYE Vision testing • Should be done with any visit involving an eye complaint • Used to screen children for visual problems Acuity: • Far vision - test at 6 m with Snellen chart • Patient covers one eye, and is instructed to read the smallest line possible. Patient must correctly read half of symbols on line. Repeat for other eye. • Near vision - test at 35 cm with pocket chart • Patient covers one eye, and is instructed to read smallest line possible. Repeat for other eye. Visual fields: • Confrontation test estimates peripheral vision (may be important in glaucoma, multiple sclerosis, stroke, or pituitary or other CNS tumor) • Use your own visual fields as a reference Technique - face patient at eye level. Ask patient to cover one eye. Slowly move your fingers from outside the patient's peripheral visual field towards the center of the patient's vision. Ask the patient to tell you when he sees your fingers.
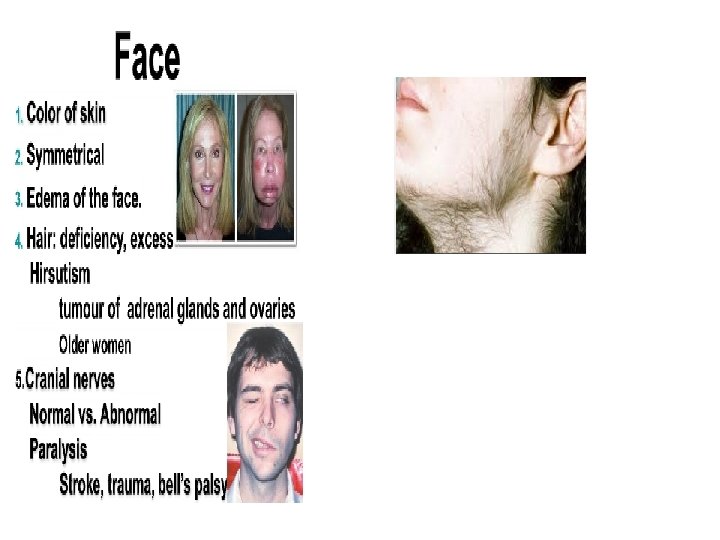
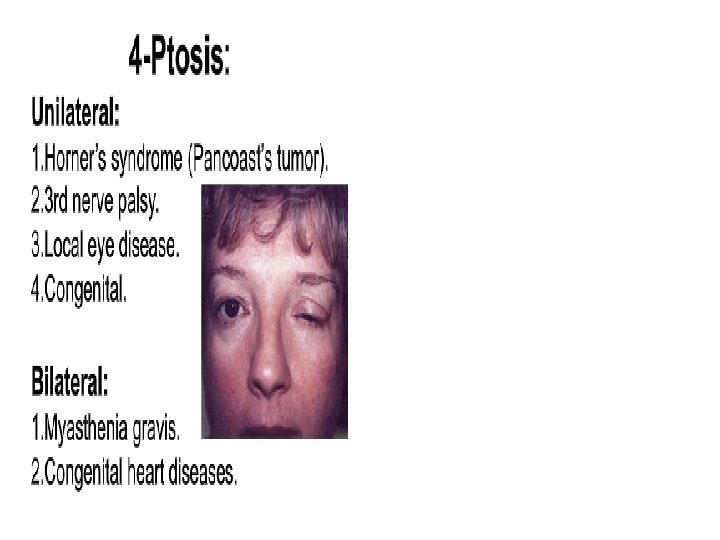
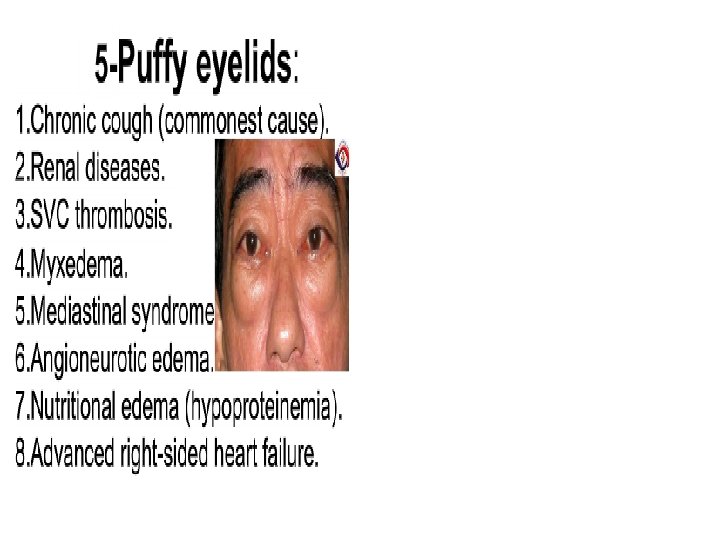
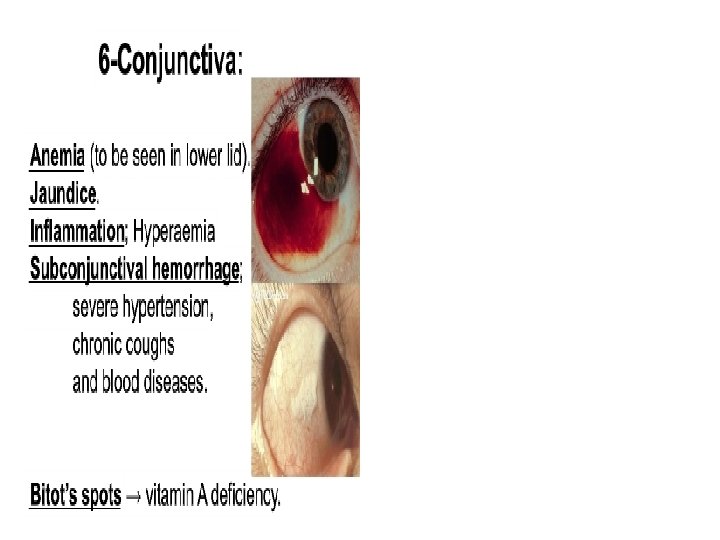
EXAMINATION of the EYE Be systematic - inspect eyebrows, lids, and globe including conjunctivae Findings Eyebrows : Loss of lateral growth may suggest hypothyroidism Xanthelasma -irregular, slightly raised yellow periorbital lesions may suggest lipid disorder Eyelids : Ptosis (TOH-sis)- if upper lid covers part of pupil (muscle weakness or neurologic lesion) Ectropion (lid turned out) Entropion (lid turned in) Hordeolum (stye)-inflammation of sebaceous gland Foreign body - may need to evert lid for full inspection • Conjunctiva: Hemorrhage- from trauma
EXAMINATION of the EYE Conjunctivitis- inflammation from infection, allergy. . . Pterygium - growth of conjunctiva over cornea Cornea: Sensation tests cranial nerve V (CN V) Arcus senilis - lipid deposits, seen in many elderly Pupils Check direct and consensual response to light Shine light source briefly into pupil, observing for constriction. Shine again into pupil, and observe for constriction of contralateral eye. Check accommodation (papillary constriction with near focus) Ask patient to look at finger held several feet from face, then to look at finger brought just beyond the end of the patient's nose. Findings: • Miosis if <2 mm (narcotic use, elderly) • Mydriasis if >6 mm (head injury, drugs) • Anisocoria - unequal pupil size, may be normal variation
Extraocular eye movements Test CN III, IV, VI and 6 extraocular muscles (EOM). Technique Patient watches your finger move through 6 "cardinal positions" Observe for coordinated movement, nystagmus (or "jerkiness" of motion. Findings Lack of coordinated movement denotes problem with cranial nerves or muscle strength/alignment. Nystagmus- involuntary rhythmic eye movements A few beats of horizontal nystagmus at extreme lateral gaze is normal Lid lag- exposure of sclera over iris as patient moves eyes inferiorly (found in hyperthyroidism)
Oculary movements / Extraoculary muscles / nerves
EXAMINATION of the SINUSES Frontal and maxillary sinuses are the most accessible to examination Palpation and percussion may or may not be helpful Transillumination of maxillary sinuses: Darken room completely Look for light transmitted through sinuses to hard palate Lack of transillumination suggests that sinus is filled with secretions The following increase the likelihood that your patient has sinusitis: History of colored nasal discharge Poor response to decongestants Maxillary tooth pain Physical exam showing purulent nasal discharge and abnormal maxillary sinus transillumination
EXAMINATION of the Thyroid • Inspection • Inspect the thyroid with the neck slightly extended, using tangential lighting. Goiter is essentially ruled out if thyroid gland is not visible with neck extension. Mood? Hair loss? Dry skin? Periorbital oedema • Palpation: • palpate for size, nodules, and tenderness • Anterior or posterior approach – we prefer you learn the posterior approach. • Relax neck by using neutral position, also may further relax muscles on one side by tilting toward that side • Identify the appropriate level of the thyroid isthmus (below the cricoid cartilage). • Gently retract the trachea to the opposite side of the lobe you are palpating. • Have the patient swallow a sip of water while you palpate
THYROID • • • Important symptoms Duration of symptoms Signs/symptoms of under/over activity Any pain? Any problems with breathing? Any problems swallowing? Any changes in their voice? Family history? Previous radiotherapy? / irradiation? Are they on any current medications?
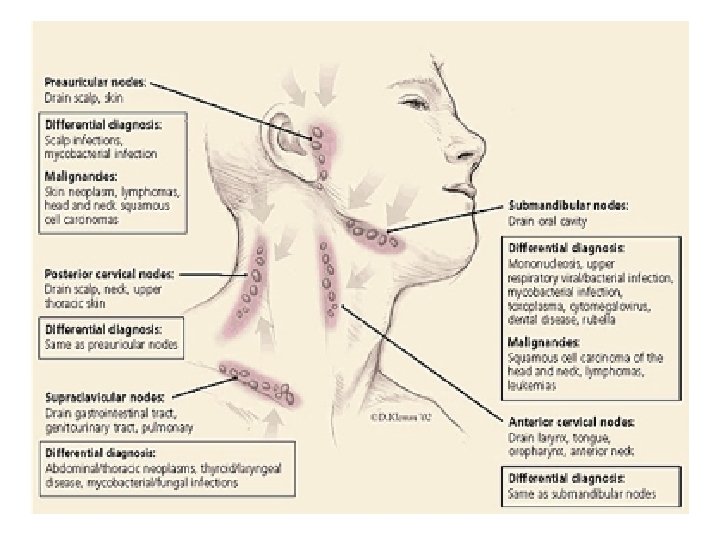
Findings: • Size: < 1 cm normal. • Consistency: hard or rubbery • Mobility: mobile or fixed • Tenderness: suggests inflammation • Warmth: suggests inflammation • If you find enlarged nodes, check drainage areas for infection, inflammation, or cancer • Important example: "Virchow's node"- left supraclavicular often a clue to abdominal or thoracic malignancy • Common example: Tonsillar or retropharyngeal nodes often enlarged in strep throat.