Hba 1 c for diagnosis Dr Karen Adamson

Hba 1 c for diagnosis Dr Karen Adamson

What is Hb. A 1 c? • Glucose binds irreversibly to haemoglobin in red blood cells, forming Hb. A 1 c • The higher the glucose, the higher the Hb. A 1 c • Hb. A 1 c reflects the prevailing blood glucose over the preceding 2 -3 months

Why Measure Hb. A 1 c? • • Serial measures show an individual’s glucose control, and thus risk of complications, change in response to alterations in management • • Measure 2 -6 monthly • • Set individual target levels
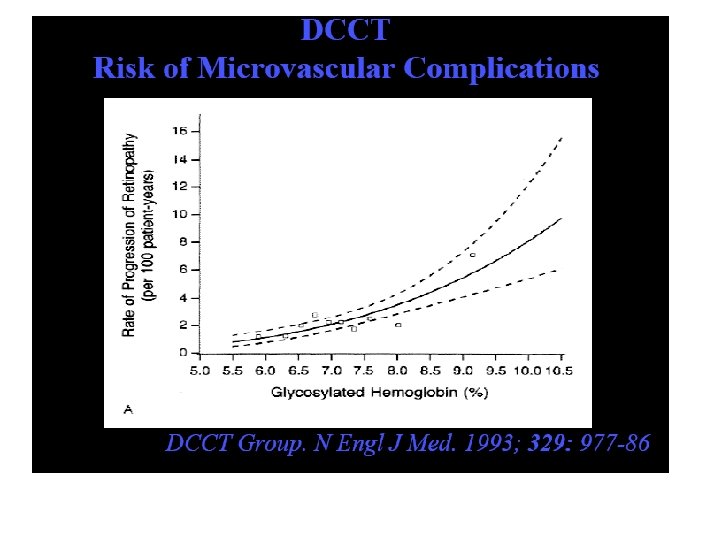
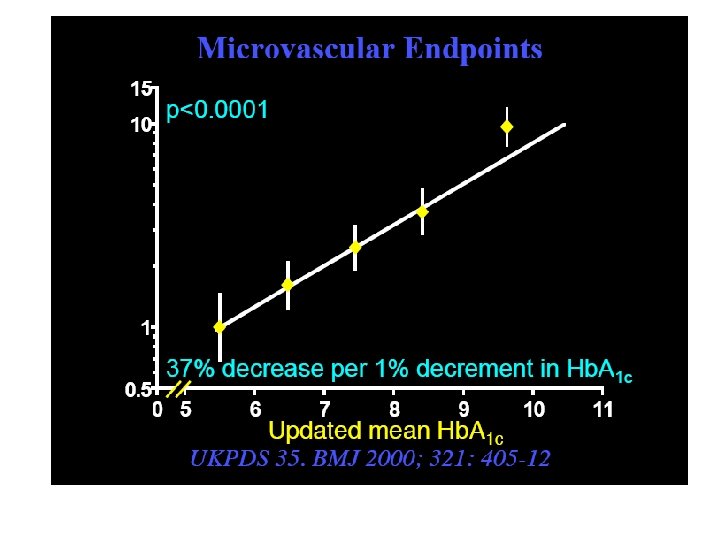

Hb. A 1 c as an Indicator of Glycaemic Control
* • Preferred test for")
Available Measures of Glycaemic Control – Fasting Plasma Glucose (FPG)* • Preferred test for diagnosis (mmol/l or mg/d. L) • Snapshot of glycaemia – Oral Glucose Tolerance Test (OGTT) • Response to glucose challenge, can be used to diagnose disease – Hb. A 1 c (Glycated Haemoglobin) • Long-term measurement of glycaemic control (~3 months) – Postprandial Glucose (PPG) • Glucose level after eating (mmol/l or mg/d. L)** – Random Blood Glucose (RBG) • Measures blood sugar at any point in time, normal levels not defined – Continuous Glucose Monitoring (CGM) • Assesses how blood glucose levels react to insulin, exercise and meals *measured after at least 8 hours of fasting; **measured 1 - 2 hours after eating
 Rapid onset of diabetes a) Suspected")
Not suitable for Hb. A 1 C 1) Rapid onset of diabetes a) Suspected T 1 DM – see symptomatic patient flowchart b) Drug-induced: steroids, anti-psychotics, immunosuppressants – a fasting glucose may not be sufficient. Seek advice from diabetes team. c) Pancreatic disease. Seek advice from diabetes team. 2) Pregnancy – Hb. A 1 C reduced in pregnancy. Gestational diabetes should be diagnosed by OGTT. N. B. OGTT diagnostic criteria are lower than for the general population. 3) Conditions affecting Hb turnover / Hb. A 1 C assay a) Haemoglobinopathy b) Haemolytic anaemia c) Severe blood loss, Blood transfusion d) Splenomegaly / Splenectomy e) Renal dialysis +/- erythropoitein f) Anti-retrovirals, ribavarin, dapsone

Diagnosis of diabetes mellitus in symptomatic patients Thirst, polyuria Unexpected weight loss Symptomatic patient Recurrent infection Blurring of vision Discoloured/ulcerated feet + random glucose ≥ 11. 1 mmol/L or fasting glucose = ≥ 7. 0 mmol/L DIABETES Mild symptoms Severe symptoms ? ketotic Full assessment & initiate management of Type 2 Diabetes vomiting / dehydration young OR age ketonuria (or ketonaemia*) URGENT discussion with diabetes team (may need insulin therapy) URGENT HOSPITAL ADMISSION *ketones can be measured on some POC glucometers
 random ≥ 11.")
Diagnosis of diabetes mellitus in asymptomatic patients (repeat on separate day) random ≥ 11. 1 mmol/L glucose INITIAL lab glucose (random OR fasting) fasting glucose repeat fasting glucose ≥ 7. 0 mmol/L not diabetic ≤ 6. 0 mmol/L high risk 6. 1 – 6. 9 mmol/L Consider Hb. A 1 C diabetes random glucose 7. 8 – 11. 0 mmol/L fasting glucose 6. 1 – 6. 9 mmol/L YES ≥ 7. 0 mmol/L suitable for Hb. A 1 C? * NO (repeat blood test on a separate day) Hb. A 1 C not diabetic high risk diabetes ≤ 41 mmol/mol 42 – 47 mmol/mol ≥ 48 mmol/mol OGTT not diabetic high risk diabetes fasting glucose ≤ 6. 0 6. 1 – 6. 9 ≥ 7. 0 mmol/L AND OR OR 2 -hr glucose ≤ 7. 7 7. 8 – 11. 0 ≥ 11. 1 mmol/L All glucose measurements used for diagnosis must be laboratory samples
- Slides: 10