Hand Trauma CT 3 MSK Day Vijay Kama



















")















 amputation")








 • Dorsiflexion & radial deviation (glass holding")





















- Slides: 75
Hand Trauma CT 3 –MSK Day Vijay Kama Consultant EM Peterborough City Hospital
Let us look ……… • • Why is it important? Basic anatomy Clinical examination Common injuries
Hand Injuries
The Importance of the Hand • Communication • Sensation • Employment • Independent Living
The Hand - Communication • Greetings
Communication… • Gestures
Communication… • Sign Language
Sensation • Large area brain structure devoted to touch. Highly sensitive.
Sensation… • Relationships
Employment • Use of hands fundamental to most vocations.
Independent Living • Without the use of our hands, most people would find independent living impossible.
• This equals 6 -8 weeks off work!! No income for 2 months. How would your finances cope?
Basic Anatomy of the Hand
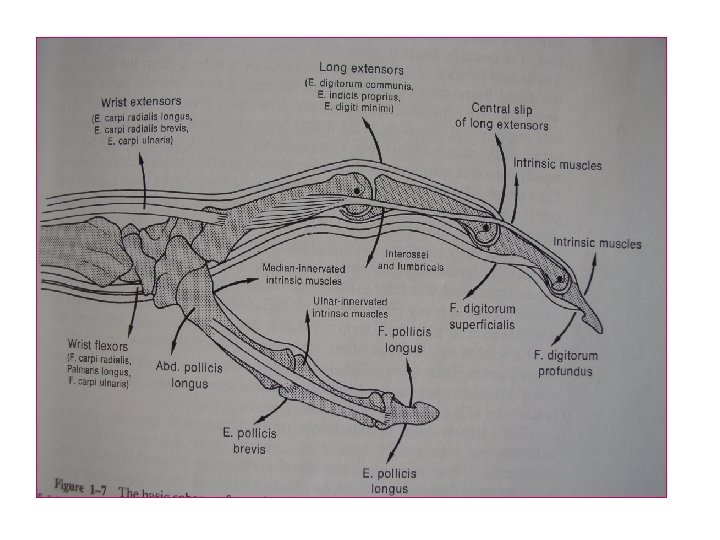
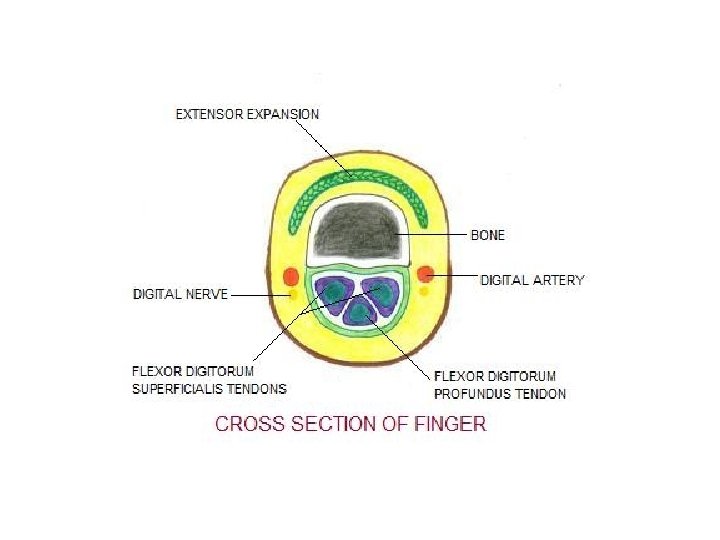
Anatomy - Tendons
Anatomy - Nerves
Anatomy of the Hand • Small area – lots to injure. • Even small lacerations may cause functional issues.
Assessing the Injured Hand - Look
Assess the Finger Posture
Feel • Is it cold? • Is sensation intact?
Frequently Presenting Hand Injuries • • Fractures Lacerations/Penetrating Injuries Amputations De-gloving Injuries Human (punch) Bites Animal Bites Hand infections
Lacerations • Very common cause of trauma. • Typical culprits –
Common Results
Lacerations • Regardless of size, always have a high suspicion for more serious injury. • Remember, glass only ever stops cutting when it hits bone. • Lacerated tendon when repaired takes 6 -8 weeks of healing and hand therapy to recover. • Nerve repairs often take 3 -6 months to get some benefit from the repair
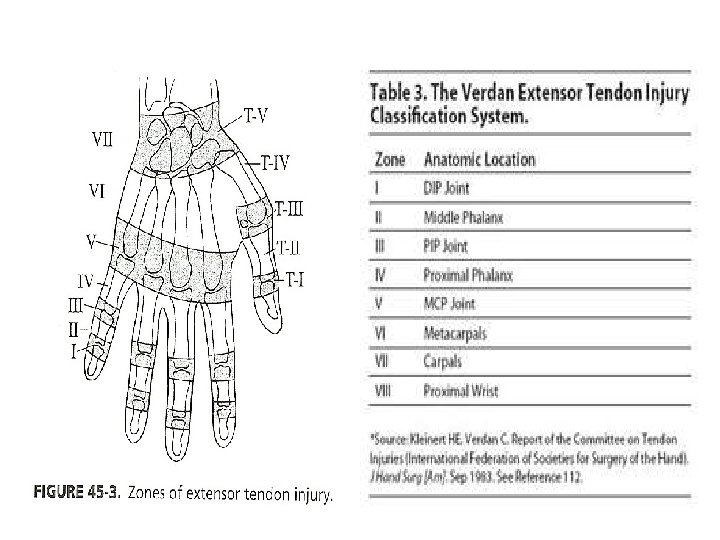
Tendon injuries Extensor tendon Injury: – Divided into Zones according to anatomical location of injury – In the hand wrist there are 7 extensor tendon zones Ref. http: //emedicine. medscape. com Orthopedic Surgery for Flexor Tendon Lacerations Author: Michael Neumeister, MD, FRCSC, FACS; Chief Editor: Harris Gellman, MD http: //www. orthobullets. com- Flexor Tendon Injuries- Derek Moore MD 27
Zone Presentation Management Mallet Deformity • Closed: splinting 6 -8 weeks • Open: suture repair for fixation. Soft tissue reconstruction Boutonniere’s Deformity • Closed: splinting MCP and PIP in hyperextension for 6 weeks • Open: suture repair (figure of 8 suture) V Fixed flexion of MCP • Closed: splinting , 45 extension at wrist and 20 flexion at MCP • Open: suture repair. VII Fixed flexion of MCP • Suture repair followed by post-op splinting I III 29
Deformities can be due to tendon, bone , nerve injury and joint dislocations – Specific types – Tendon injuries • Mallet finger
• Boutonniere deformity • Z deformity of the thumb
Flexor tendon injuries – 5 zones in the hand the wrist FDS Insertion Flexor Sheath Zone 1 One tendon only (FDP) from middle of middle phalanx distally Zone 2 Two tendons (FDS & FDP) from MCP joints to middle of middle phalanx Zone 3 Central palm Zone 4 Tendons in the carpal tunnel Zone 5 Tendons proximal to the carpal tunnel
Zone I II III, IV Thumb Presentation Loss of active flexion at DIP joint Hyperextension of DIP joint (Jersey finger ) Management Flexor injury • Primary or Secondary tendon repair • Careful suturing prevent post-op adhesions. • Skin closure then secondary repair Loss of active flexion by tendon grafting • Primary repair performed by at MCP joint skilled hand surgeon to minimize post-op adhesions. Same • Primary or secondary tendon repair • Examine carefully for thenar muscle injury and recurrent branches of median nerve. 34
Amputations • Can occur at any level. • Ability to re-plant / re-vascularise depends on both the level of amputation and the mechanism. • Once past the distal third of the distal phalanx the vessels are too small to be anastamosed.
Finger Tip Amputation Injured components may include skin, bone, nail, nail bed, tendon, and the pulp, the padded area of the fingertip.
• If just skin is removed and the defect is less than a centimeter in diameter, it is often possible to treat these injuries with simple dressing changes. • If there is a little bit of bone exposed at the tip, it can sometimes be trimmed back slightly and treated with V-Y plasty
Amputation. . .
Decision is based on: Importance of the part, level of injury, mechanism of injury expected return of function.
Recommended ischemia times for replantation: ◦ Major replant: 6 hours of warm and 12 hours of cold ischemia. ◦ Digit: 12 hours for warm ischemia and 24 hours for cold ischemia. Preoperative preparation: radiography of both amputated and stump parts to determine the level of injury and suitability for replantation 40
Outcome Overall success rates for replantation approach 80%. Better outcome with Guillotine (sharp) amputation (77%) compared to severely crushed and mangled body parts(49%). In general, the prognosis for ring avulsion injuries is poor. Studies have demonstrated that patients can expect to achieve 50% function and 50% sensation of the replanted part. Ref. Plastic Surgery, Goldwyn and Cohen, 3 rd edition. Plastic Surgery, Grabb and Smith, 3 rd edition. 41
De-gloving Injuries
Followup • Can get large areas of skin loss. • Typically treated as a skin graft with original skin, or debrided and skin grafted from the thigh. • Can get contraction of the scar.
Punch Bite Injuries • Very common. • Injury occurs after punching someone in the mouth. Usually small laceration to the 2 nd or 3 rd MCPJ. Often extends into the joint with damage to the extensor tendon. • Always requires IVABs and a washout. • Common consequences – septic arthritis, extensor tendon loss.
Punch Bite
Followup • Usually require at least 1 washout. Sometime multiple. • Tendon cannot be repaired if already infected. • Tendon, although intially intact can be completely destroyed by infection. • Always, always refer.
Animal Bites • Cat bites – frequently become infected. Cat teeth puncture like a needle and deposit bacteria at the base to then form an abscess. • Dog bites – easier to treat than cat bites as dog teeth typically tear leaving the wound open and able to be irrigated. Cosmetically more difficult to treat.
Fractures and dislocations
Diagnosis…. . • Tenderness in anatomical Snuff box • Xray- fracture line
Treatment • Scaphoid cast (3 -4 months) • Dorsiflexion & radial deviation (glass holding position)
• Internal fixation • Herbert’s screw
Complications • Avascular necrosis • Delayed / non union • Wrist osteoarthritis
Lunate dislocations • Lunate dislocation perilunate dislocation • Open reduction • Avascular necrosis
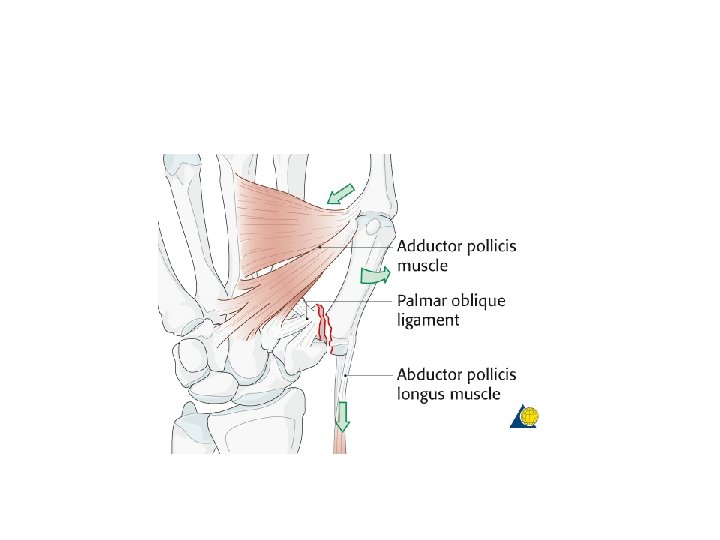
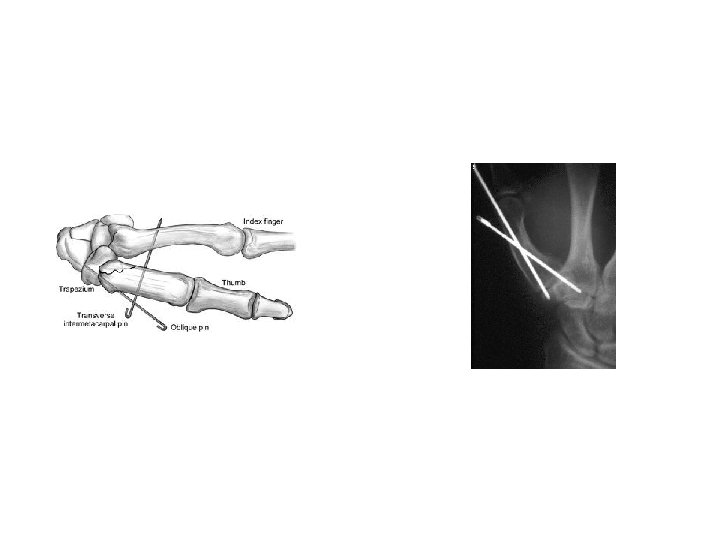
Bennett’s fracture dislocation • Base of 1 st metacarapal • Intra articular • Longitudinal force to thumb
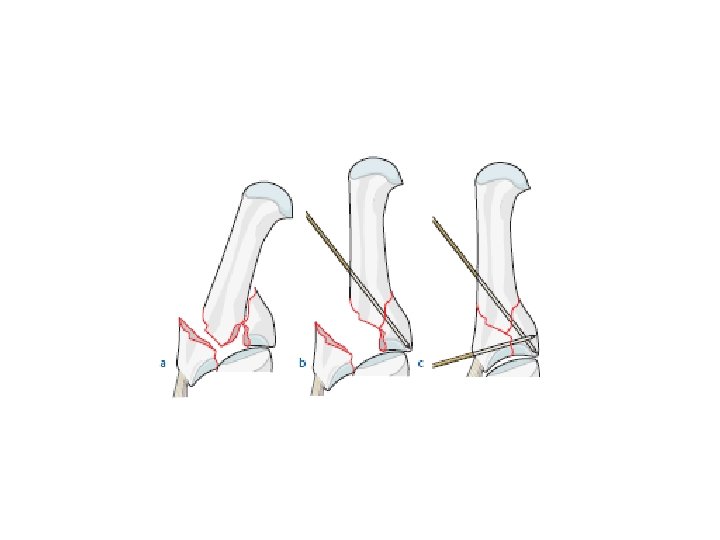
Rolando Fracture • Comminuted First Metacarpal Base # • Presents as ‘Y’ or ‘T’ Pattern • Differs from Bennette that usually no diaphyseal displacement
CMC dislocation 4 th 5 th MC
#dislocation of 5 th mc , reduced and fixed with k wires
Fracture phalanges • Fall of heavy object or crush injury • Undisplaced Displaced • Strapping • Open reduction
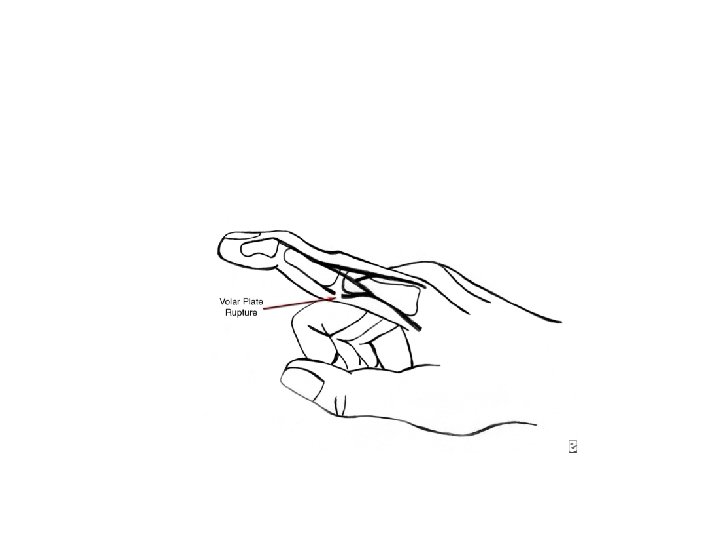
PIPJ dislocations/ volar plate disruption
PIPJ dislocation • Mechanism of Injury – hyperextension of the PIP joint • with or without dislocation • often initial injury seems trivial
PIPJ dislocation • If dislocation without # OR If # fragment less than 30% joint surface → reduce then manage conservatively in dorsal blocking splint (DBS)
Dorsal blocking splint • PIPJ in 30 degrees flexion • volar structures off stretch • slowly increase out to neutral
#’s • 5 th Metacarpal – Assess ROM and digit Rotation – Usually managed conservatively
#’s • 4 th Metacarpal Spiral # – Assess ROM and digit Rotation – Tendency to rotate – Impacted #’s result in extension lag = poor function.
Paronychia • infection of the finger that involves the tissue at the edges of the fingernail • superficial and localized to the soft tissue and skin • most common bacterial infection seen in the hand ( staph; strep).
Paronychia treatment • wound care alone. • collection of pus - drain. – a simple incision over the collection of pus to allow drainage. – scalpel may be inserted along the edge of the nail to allow drainage. – If the infection is large, a part of the nail may be removed. • oral antibiotic. • wound care at home.
Felon • infection of the fingertip. • This infection is located in the fingertip pad and soft tissue associated with it.
Felon treatment • incision and drainage » incision will be made on one or both sides of the fingertip. » break up the compartments » gauze will be placed into the wound to aid the initial drainage. » flush out with a sterile solution • antibiotics.
Infectious flexor tenosynovitis & Deep space infection • infection involves the tendon sheaths and deep spaces • penetrating trauma that introduces bacteria • surgical emergency and will require rapid treatment with IV antibiotics.
Kanavel’s cardinal signs • intense pain – along the course of tendon with extension – this is the earliest and most important sign • flexion posture • uniform swelling • percussion tenderness along the course of the tendon sheath