Hand Assessment and Common Injuries Objectives Understand how

Hand Assessment and Common Injuries

Objectives Ø Understand how to assess patients with hand injuries. Ø Decide what investigations are needed. Ø Introduction to common hand injuries.

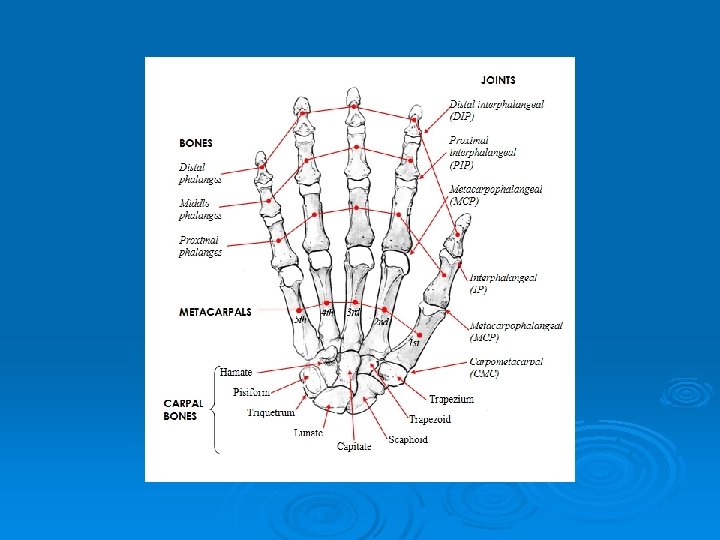

Nerve supply

Flexor tendons

Extensor tendons

Joints

History Mechanism of injury Ø Symptoms Ø Age, sex, handedness, occupation Ø Relevant pastimes/hobbies eg musician Ø Previous illness/injuries/operation on relevant limb Ø Current medication, allergies, tetanus status, Ø

General examination LOOK front and back for swelling, deformity, colour, wounds Ø FEEL bony tenderness, crepitus, instability Ø MOVE active and passive Ø Ø REMOVE RINGS

Specific Qs: Is there rotation?

Tendon Examination FDS Ø FDP Ø Extensor tendons Ø FPL Ø EPL Ø

Elson's Test Ask Pt to extend against resistance. Weakness of resisted extension of PIPJ & hyperextension of DIPJ occurs if the central slip is ruptured.


 Ø Median, ulnar")
Neurovascular Examination Nerves Ø Digital nerves (radial side and ulna side) Ø Median, ulnar and radial Circulation Ø Pulses Ø Colour Ø Temperature Ø CR

Common Injuries

Boxer’s fracture • Punch Injury • NB Bite wounds • Look for rotation, extensor lag and angulation Ø Investigation • X ray Ø Treatment • Neighbour strap distal #, volar slab proximal # • Elevation • Refer if wound/ >30 o angulation/rotation


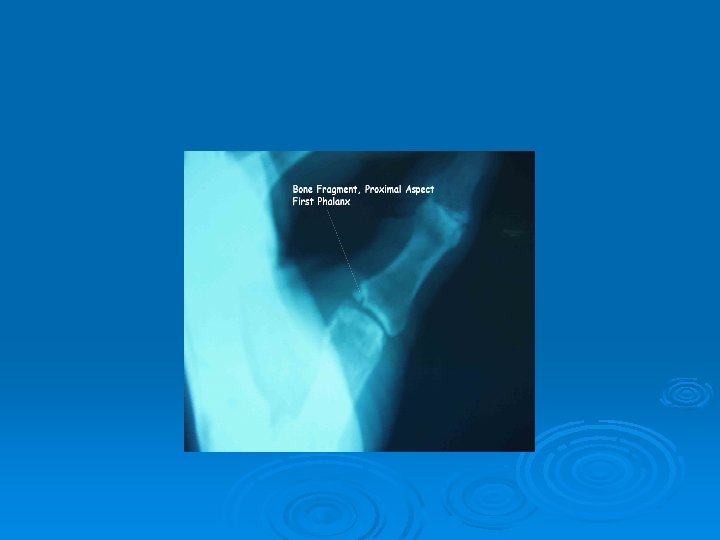
Bennett’s fracture-dislocation • Fall onto thumb • Fracture through base of thumb MC Ø Investigation • X ray Ø Treatment • Ortho referral for MUA & fixation

Ulna Collateral Ligament Injuries of the Thumb

History - Forced abduction of thumb Ø Examination - Tender MCP, laxity of UCL Ø Investigation – X-ray to exclude associated # Ø Treatment – sprain thumb spica, rupture refer. If unable to assess UCL due to pain review after a few days Ø


Volar plate injury

Mallet finger History – usually minor trauma to fingertip with inability to extend DIP joint Ø Examination DIP flexed with no active extension but full passive Ø X-ray – if large fragment of joint surface may require operative repair Ø Mallet splint in hyperextension Ø Review after 1 week to check splint still ok and skin is not macerated Ø Will require splintage for 6 weeks Ø


Fingertip Injuries Ø X-ray Ø Subungual haematoma –trephine. Ø Lacerated nail bed – ? Suture (absorbable) replace nail and secure with steristrips.


Amputations Amputation -amputated part wrap in a saline moistened swab, place this in a polythene bag and lay on top of ice in a container. Ø X-ray Ø Children – Rx conservatively Ø Tetanus? Ø abx Ø

Lacerations/Incisions History – usually glass or metal Ø Examination – record length and nature of wound. Examine base of wound for structural damage. Test nerve and tendon function. Assess circulation. Ø X-ray if possibility of retained glass FB Ø Usually primary closure Ø If deep structure damage refer Ø Complex lacerations refer Ø

Any Questions?

Summary Hand anatomy Ø History Ø Hand examination Ø Management of common injuries Ø
- Slides: 33