Hampshire Community Health Care Shoulder Pathologies and Physiotherapy






 �Primary � Bony abnormalities in the")
 § Articular side of Supraspinatus becomes impinged")
 § Subacromial space § Space 9 -10 mm § Arm")


























")

- Slides: 38
Hampshire Community Health Care Shoulder Pathologies and Physiotherapy Sharon Dekkers MSc MCSP
Contents q. Anatomy q. Pathologies and Treatment q. Sources of referred pain q. Exercises q. Neural mobility exercises – sliders q. Outcome measures
Anatomy – Shoulder joint complex � Glenohumeral joint � Acromioclavicular joint Sternoclavicular joint Scapulothoracic joint
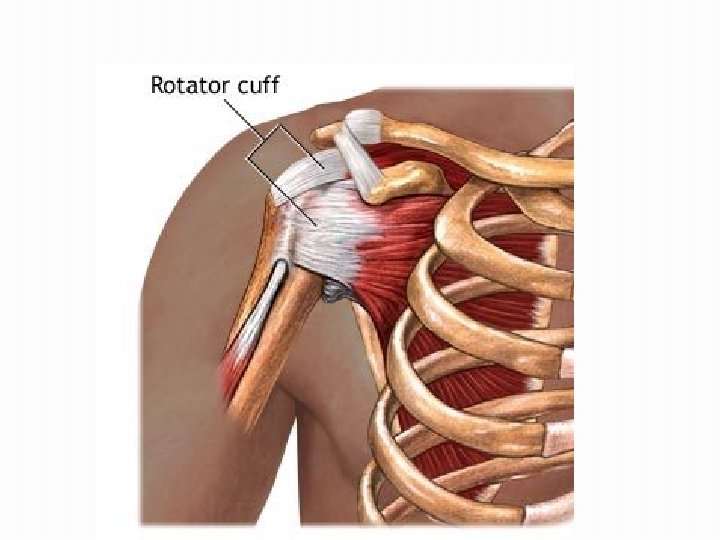
Anatomy - Rotator Cuff Muscles Supraspinatus Infraspinatus Teres Minor Subscapularis
Anatomy - Rotator cuff posterior aspect
Pathologies q. Impingement Syndrome q. Rotator cuff tear q. ACJ q. Labral lesions q. LHB q. TOS q. Referred Pain
Impingement External Internal External impingement (Sub-acromial Impingement Syndrome) �Primary � Bony abnormalities in the shape of the acromial arch � Bone spurs � Calcification �Secondary � Poor scapular stabilisation � Weakness of the rotator cuff � Muscular imbalance between deltoid and rotator cuff muscles.
Impingement Internal Impingement (Posterior Superior Glenoid Impingement) § Articular side of Supraspinatus becomes impinged between the greater tuberosity and the posterosuperior labrum. § Abduction and external rotation are affected. § Pain at the posterosuperior aspect of the shoulder
Subacromial Impingement Syndrome (External) § Subacromial space § Space 9 -10 mm § Arm elevation – superior head displacement § Rotator Cuff muscles § § § Provide dynamic stability Work with deltoid Prevent superior translation of HH § RC – Deltoid balance
Sub-acromial space contents § § Supraspinatus tendon Long head biceps tendon Subacromial bursa Superior border of capsule
Causes of Impingement § § § Instability/hypermobility RC overuse or tendinopathy Tight posterior GH capsule Poor scapular muscle control Poor Posture
Causes of impingement § Poor Tx spine extension – reduced GH elevation § Increased Tx kyphosis and FHP (forward head posture) will cause: § scapulae to abduct § resulting in lengthening of rhomboids and LFT § shortening of serratus anterior, latt dorsi, subscap – reduced § § § scapular upward rotation shortening of pect major and pect minor pull the coracoid process downwards bringing the acromion over the head of the humerus causing a mechanical block to arm elevation reduced subacromial space
Impingement tests SIS Hawkins Kennedy – pushes supraspinatus tendon / RC/ against coraco-acromial ligament q Neer’s Impingement test q Painful arc q Internal Impingement / Postero. Superior q Shoulder Abd, LR induce posterior pain, relieved by humeral head relocation (AP glide of humeral head)
Treatment q. Correct biomechanics of shoulder joint complex q. Correct posture q. Increase Tx mobility q. Lengthen shortened muscles q. Release tight posterior capsule or posterior cuff q. Strengthen weaker muscles esp. RC and scapular upward rotators – SA and LFT
RC Tear § Partial or Full § Overhead activity, trauma or recurrent impingement § If atraumatic - chronic diffuse pain more than 3 months § Common in over 40’s Tendonosis, smoking, steroids, RA, Diabetes § Affects 7% of elderly § Unable to sleep on effected shoulder § Limited internal rotation, passively painful
RC Tests § SS § § § IFS Full can Drop arm – eccentric control § LR at 45 deg MR at GHJ to minimize SS, post deltoid LR lag sign, Drop sign (Stop) § Hornblower’s sign (LR in 90 scaption) § § TM § Sb. Scap § Gerber Lift off / Belly press
ACJ q. Pain when lying on effected shoulder q. Pain when reaching arm across body q. Pain with passive or active arm adduction q. Tender on palpation over ACJ q. Scarf test / Cross body adduction
Labral lesions q. Superior – SLAP q. Bankart lesion Causes �FOOSH �Repetitive movements �Strong biceps contraction
Symptoms of glenoid labrum tears q. Clicking or catching with shoulder movements q. Vague pain at front or top of shoulder q. Pain is made worse by overhead activities or when the arm is held behind the back. q. Weakness and Instability in the shoulder. q. Pain on resisted flexion of the biceps
Labral SLAP tests q O’Brien Active Compression Test Pt stdg, flexion 90°, adduction 15° with elbow extended Full MR so thumb pointing down Resist flexion Pt laterally rotates arm so thumb pointing up Resist flexion Positive test = Pain or painful clicking elicited with thumb down and decreased or eliminated with thumb up q Crank test Shoulder elevated to 160° in the scapular plane A gentle axial load is applied through glenohumeral joint with one hand, while other hand does IR and ER Positive test = pain, catching, or clicking in the shoulder
Long Head Biceps q. Yergason’s test Elbow flexed 90. Resist supination of forearm. Positive test if tenderness over bicipital groove q. Speeds test Resist forward flexion of extended and supinated arm from 0 – 60 dg flexion
Thoracic Outlet Syndrome Abnormal compression of the neurovascular bundle by bony, ligamentous or muscular structures at thoracic outlet Neural symptoms: Paraesthesia esp C 8 T 1 dermatomal distribution q Pain in upper limb and hand q Numbness q Muscle weakness and atrophy of hand muscles q Difficulty with fine motor control of hand q
Thoracic Outlet Syndrome Vascular symptoms: Deep pain at neck and shoulder, worse at night q Feeling of heaviness in arm or hand q Fatigue in arms and hands q Swelling of hand q Bluish discoloration q Superficial vein distention in hand q
TOS q. Interscalene triangle q. Costoclavicular triangle q. Subcoracoid space
TOS Tests �Adson’s test Locate the radial pulse Neck rotation toward the tested arm Neck extension PT extends the arm Deep inspiration with hold A positive test is indicated by a disappearance of the pulse. �Allen’s test Shoulder horizontal extension and lateral rotation Palpate radial pulse Neck rotation away from the tested arm Positive if radial pulse disappears
Referred Pain : Cervical
Referred Pain: Gastro-Intestinal Liver : R shoulder Gall bladder: R shoulder and R scapula Diaphragm : unilateral / bilateral shoulder pain Spleen: L shoulder + upper 1/3 arm Aortic Aneurysm: L scapula Cardiac: L shoulder + Scapula Post Laparoscopy: uni / bilateral shoulder pain
Referred Pain: Pancoast Tumour of apex of lung Invade chest wall structures such as Lymphatics Lower roots of brachial plexus (esp. C 8, T 1) Intercostal nerves Sympathetic chain and Stellate ganglion Adjacent ribs Initial symptom is pain in the shoulder and medial aspect of scapula Referred pain to C 8, T 1, T 2 dermatomes Horner’s syndrome later develops Pt supports arm to relieve neural tension Hand muscles later develop atrophy
Exercises Scaption instead of Abduction Better joint congruence q Reduced tensile forces on ligaments q Optimal sub-acromial space and clearance q Optimal alignment of RC muscles q Increased proprioceptive feedback q Increased activation of scapula upward rotators and RC muscles q Exercises for RC with minimization of deltoid and Upper Fibres Trapezius activity
Exercises RC q. Supraspinatus Full can in scaption +/- wt Empty can in scaption <90 dg q. Infraspinatus / Teres minor LR in varying degrees of abduction q. Subscapularis MR in varying degrees of abduction Diagonal exercise Dynamic hug Push up plus
Scapular exercises Side lying flexion +/- wt Side lying lateral rotation +/- wt LFT – prone arms overhead MFT – prone 90 abd with LR UFT – prone arms by side Scapular setting progression in prone: Short lever arm, lateral rotation (wrist lift) Short lever arm, medial rotation (elbow lift) Short lever arm lift Long lever arm lift with wt Stability exs – active wall slide with towel, 4 point, and ball press ups
Exercises q. Serratus Anterior Knee Push up plus Seated press up Forward punch with TB attached behind Scaption with wt Dynamic hug
Posterior capsule tightness q. STM of soft tissues at posterior shoulder q. Medial rotation stretch (Sleeper’s stretch) q. Horizontal adduction stretch q. AP glide in neutral / medial rotation q. AP axial glide in horizontal adduction q. Corner stretch for pectoralis minor q. Doorway stretch for pectoralis major
Neural mobility exercises Median nerve Radial nerve Ulnar nerve
Outcome measures - SPADI Activity Difficulty 1. Washing your hair? 2. Washing your back? 3. Putting on an undershirt or pullover sweater? 4. Putting on a shirt that buttons down the front? 5. Putting on your pants? 6. Placing an object on a high shelf? 7. Carrying a heavy object of 10 pounds? 8. Removing something from your back pocket? Disability scale: How much difficulty do you have…. 0 = no difficulty 10 = unable to do NA = not applicable Pain
DASH (Disabilities Arm Shoulder Hand)
Outcome measures – Simple shoulder test