Group Visits Edward Shahady MD Medical Director Diabetes
 Florida Academy")
Group Visits Edward Shahady MD Medical Director Diabetes Master Clinician Program (DMCP) Florida Academy Family Physicians Foundation

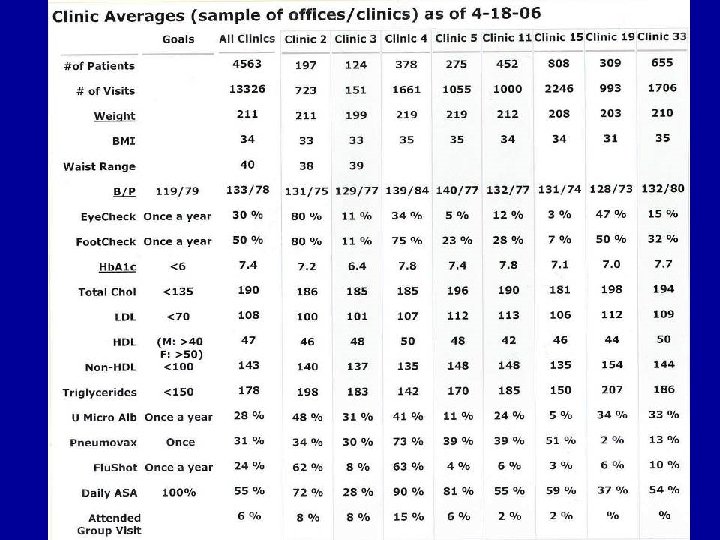
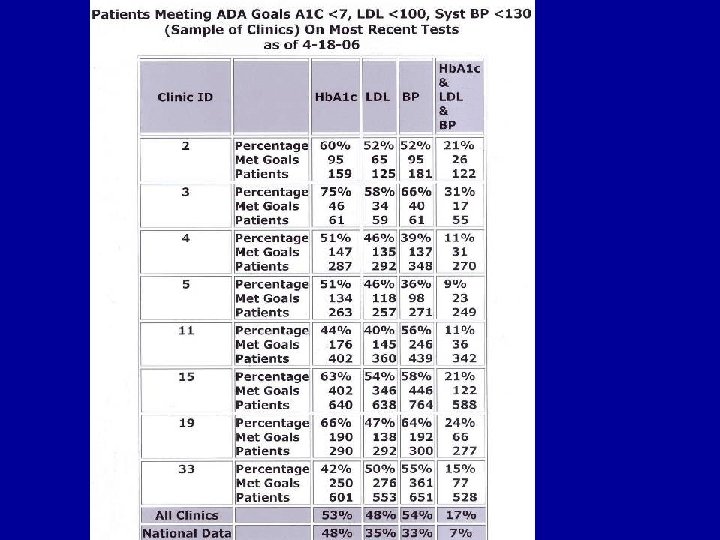
DMCP Program • Started November 2003 • Now has 35 practices->4500 patients and >13, 000 visits in the database (3 are residency programs) • All use the registry-60% conduct group visits • Registry is internet based system designed by IT consultant with clinical input from myself and other physicians re diabetes standards of care. • Team of a clinician and nurse/MA undergo 18 hours of training-1/2 in their offices-Practice manager and other staff also receive training. • Graduate as Diabetes Master Clinicians and Clinician Associates

Stages of New ideas in Medicine • Stage I the idea is considered absurd and or ridiculous • Stage II it is considered what “Fringe Drs Do” the “cutting or bleeding edge” • Stage III reaches the point of “being so obvious” that it is considered the standard of care. • Stage IV The new idea becomes an “old idea that is only used by the old timers (not age related) who are afraid to change”

Many Barriers to chronic disease care Group visits- may be ideal means of overcoming these barriers

Patient Barriers to Diabetes Care • Do not understand how to achieve goals • Depression • Can not afford medications • Feel they are not able to reach goals • Angry and frustrated with their disease • Don’t feel that is possible to change diet, exercise etc • Don’t feel the bad things will happen to

Physician/Staff Barriers to Diabetes Care • Think patients do not care • Clinical Inertia- “so what” • Do not know how to use questions to stimulate reflection and goal achievement • Do not know how to empower patients • Time and reimbursement

System Barriers to Diabetes Care • Average office visit 5 to 7 minutes is wasted by the clinician trying to find all the data related to the diabetes- (organization) • Patient thinks traditional role is passive recipient of information-do not know their goals or how they need to achieve them-they are not prepared for the visit (roles)

Current Medical Education System may Promote Barriers • Acute care model may promote noncompliance and non adherence. Anderson Funnell (1) • Most exciting and memorable part of education is a bed bound patient with a short term illness. Sets up a system of immediate gratification. • Chronic care model gratification is delayed and measured differently. • Inability to adapt to different type of

Empowerment • Art of Empowerment by Anderson and Funnell-every practice given a copy of the book and CD • “Empowerment is not techniques-it is a vision and attitude” • Goal is to enable patient to make informed decisions • Patient identifies problems and learning needs • Patient is the problem solver and caregiver, professional is the resource

Group Visits • Group visits empower not only patients but also the staff and the clinician. • Group visits generate income-can charge a 99214 for 8 to 10 patients. 1 hr and 20 mins of clinician time. 2 hrs and 20 mins of one staff persons time. • Some of our DMCP practices have

Group Visits • Not Lectures-lectures provide knowledge do not change behavior • Patients experiences, values, culture, fear, myths, emotions, etc mold their behavior • Group visits provide a safe environment (trust) for discussing all of above • Emotions are the fuel of change • Physician/Nurse (MA) team need to become skilled in listening to emotion and facilitating discussion • The curriculum for a group visit is driven by the patients questions and concerns

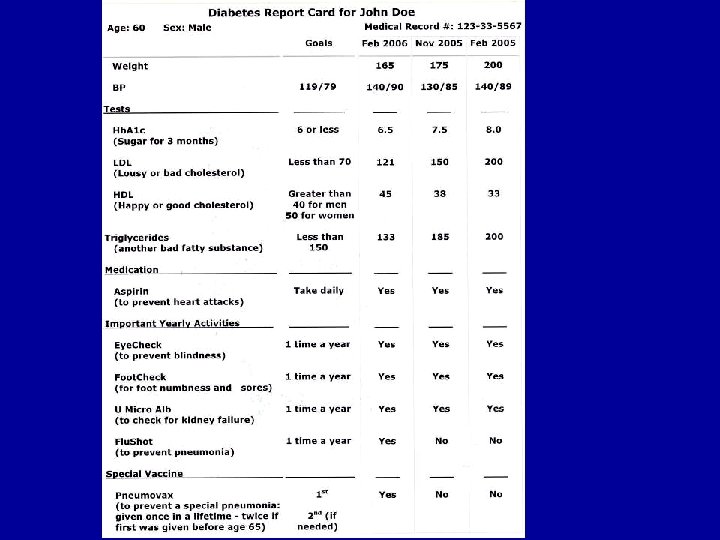
Patient Evaluations • 350 patients from DMCP evaluated the group visits • On a satisfaction scale of 1 to 5 with 5 being the highest-average rating was 4. 7 • Comments included • Loved the chance to hear from others with diabetes • The report cards are great. I no longer forget my numbers like I did before. I like terms like lousy and happy.

Group Visit Values. Patient • Increased trust in their physician • Setting attainable goals (incremental pace) • Increased confidence in their ability to do what is asked of them (selfmanagement) • Will change Behavior because they understand goals and feel they can reach them • Increased satisfaction

Group Visit Values. Physician • Offer More time to address best care activities • More time to assess patient understanding and literacy level. • Deliver consistent message to multiple patients • Increase satisfaction – Diabetes Care 26: 2032 -36 2003

Will group visits become the Standard of Care? • Yes for many chronic diseases, chronic problems and routine care like prenatal and well child care • 1/3 of patients will not try them • 20% drop out rate after attending a group visit • Some Drs will not try them • FM Residents will follow the lead of the physician faculty. • Based only on my observations and opinion

Stages of New ideas in Medicine • Stage I the idea is considered absurd and or ridiculous • Stage II it is considered what “Fringe Drs Do” the “cutting or bleeding edge” • Stage III reaches the point of “being so obvious” that it is considered the standard of care. • Stage IV The new idea becomes an “old idea that is only used by the old timers (not age related) who are afraid to change”

“It’s easy to make patient care hard and hard to make it smart” “Old habits are easyresisting the new makes smart hard”

Thanks for your attention
- Slides: 23