Greater percentage body fat Less bone and muscle

여성과 운동 Greater percentage body fat Less bone and muscle Less metabolically active tissue Reduced oxygen carrying capacity Lower stroke volume Lower maximum oxygen consumption Age of menarche Menstrual dysfunction Menstrual cycle and performance Pregnancy

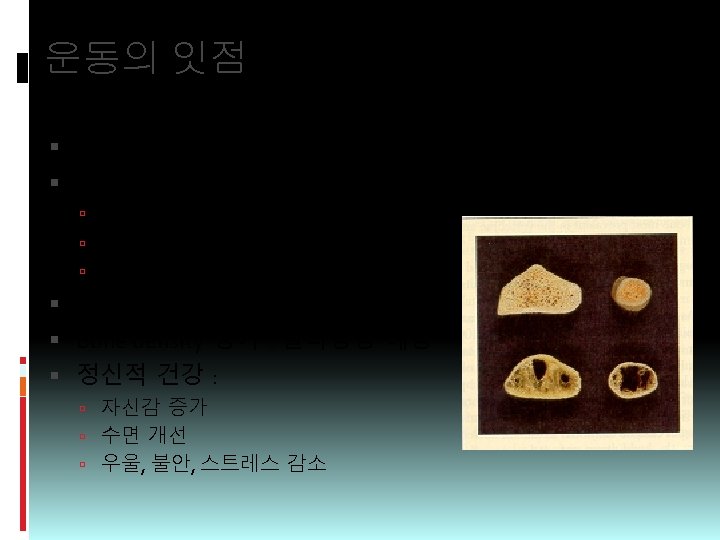
Exercise and Osteoporosis Factors affecting bone density Exercise Menopause Diet Smoking & alcohol Immobilization : increase bone resorption Moderate physical activity make higher bone density Extreme physical activity : accelerate bone loss

Aerobic vs anaerobic exercise Aerobic exercise Oxygen is supplied continuously from lung to muscles Moderate intensity : > 30 min, 70% MHR Jogging, walking, swimming, cycle Anaerobic exercise Energy is supplied from glucose (lactate accumulation) Sprint, weight-lifting, dumbell

Exercise and calorie expenditure Moderate exercise 7 -10 Cal/min expenditure Increase BMR Muscle mass , fat Muscle cell : “invisible exercise” If 300 Cal/d oversupply : 14 kg weight gain/yr Weight maintenance : 체중 유지에 운동이 중요 Prevent ‘yo-yo phenomenon’
")
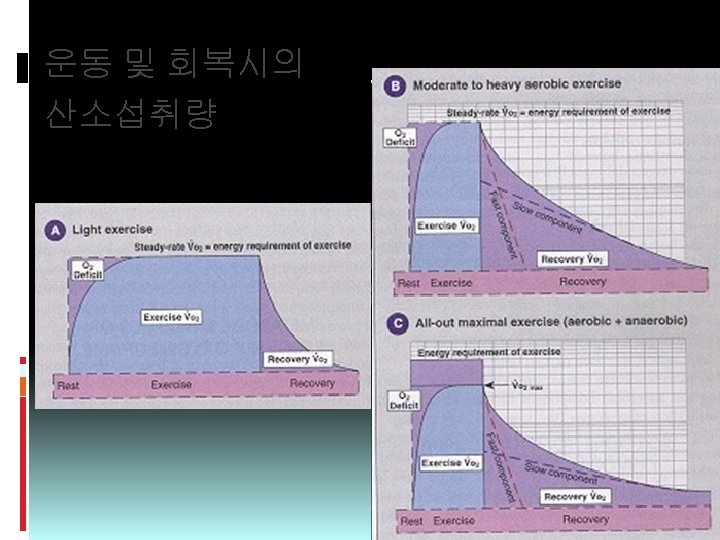
운동 후 3시간 초과 산소소비량 (EPOC; Excess Postexercise Oxygen Consumption)
 1. 2 kcal/min <20% EE")
Exercise metabolism At rest, energy expenditure (70 kg person) 1. 2 kcal/min <20% EE : skeletal muscle During intense exercise TEE may increase 15~25 times 18~30 kcal/min Blood flow to the muscle : >30 times

Energy for Muscle contraction Hydrolysis of high-energy compound ATP myosin ATPase ADP + Pi + energy Creatine phosphate (CP) ADP + CP Creatine kinase ATP + C Rapid glycolysis Aerobic oxidation Krebs cycle & electron transport chain Fat metabolism

Aerobic vs. anaerobic exercise Glycogen glycolysis Glucose G-6 -P Fatty acids ATP Pyruvate Fat Lactate Anaerobic Acetyl Co. A Krebs cycle Oxygen Oxi. Phos H 2 O + CO 2 ATP Aerobic

Energy Utilization

Measurement of Oxygen consumption Direct calorimetry Indirect calorimetry Measurement of O 2 consumption (VO 2) Metabolic rate (kcal/min) = VO 2 (L/min) × [4. 0+RQ] RQ = VCO 2/VO 2 Energy cost Metabolic equivalent 1 MET = 3. 5 ml/kg/min

Maximal Oxygen consumption VO 2 = HR × SV × a-v. DO 2 (Fick equation) 70 kg person, absolute O 2 consumption at rest 250 ml/min ÷ 70 = 3. 5 ml/kg/min (1 MET) Running at 10 km/hr pace 10 times the resting EE 10 METs = 35. 0 ml/kg/min Maximal vs submaximal RPE Moderate 13~20
의 macaque monkey 실험 1군 : normal")
Exercise, Diet & Heart disease Kramsch(Boston med college)의 macaque monkey 실험 1군 : normal diet, sedentary 2군 : atherogenic diet, kept sedentary 3군 : atherogenic diet, treadmill running (2 -3. 5 km/hr, one hour, 3/week) Resting pulse; 1, 2군 160/min, 3군 112/min bigger, more efficient heart : large LV resting & exercise pulses much wider coronary vessels thinner coronary arterial wall thickness, less collagen deposition
 목적 Risk factors 발견 적절한 운동목적 결정, 개인에 맞게 처방하기 위한")
Screening Examination (2) 목적 Risk factors 발견 적절한 운동목적 결정, 개인에 맞게 처방하기 위한 기 초 운동프로그램의 효과를 재는데 기초자료 선별검사의 3요소 생활습관(Lifestyle) 평가 : 식사, 음주, 흡연, 스트레스, 운 동습관, 동기 의학적 평가 : cardiovascular symptom, respiratory/musculoskeletal disease, P/E 운동적성(Physical fitness) 평가 : VO 2 max, submaximal exercise stress test, flexibility, muscle strength, agility

EXERCISE PRESCRIPTION Type of exercise : aerobic, stretching, resistance exercise Intensity Moderate intensity : 50 - 75% Target heart rate = 60% - 85% MHR [Karnoven: 60+(MHR-60)*0. 6~0. 85] Max Heart Rate = 220 - age Duration 25 -45 min/session 300 Cal/session Frequency : at least 3 times/week Session Warm-up : 3 - 5 min Conditioning : 15 - 40 min Cool-down : 2 - 5 min Progression Keep pulse in target range Evaluate every 2 - 4 weeks

 15 ~")
1일 에너지 소비 구성 60 ~ 75% : Resting Metabolic Rate (BMR) 15 ~ 30% : Thermic Effect of Physical Activity < 10% : Thermic Effect of Feeding

고혈압과 운동 HYPERTENSION & EXERCISE

서 론 역학 유병률 : 20~25% 고혈압 인지 - 60%, 적절한 치료 - 35% SBP 150 mm. Hg 이상 : CVD risk 2 Risk reduction : CVA, CHF Nonpharmacological Tx Behavior modification Exercise and Hypertension
 Normal <120 and Prehypertension 120 -139")
Blood Pressure Classification BP classification SBP (mm. Hg) Normal <120 and Prehypertension 120 -139 or 80 -89 Stage 1 HT 140 -159 or 90 -99 or ≥ 100 Stage 2 HT ≥ 160 JNC-7 Criteria. JAMA 2003; 289: 2560 DBP (mm. Hg) <80

2003 European Society of Hypertension Guidelines for the Mx of Arterial HT The lifestyle measures that are widely recognized to lower BP or cardiovascular risk, and that should be considered are: � Smoking cessation � Weight reduction (and weight stabilization) � Reduction of excessive alcohol intake � Physical exercise 30 -60 min moderate intensity dynamic activity 4 -7 days/week � Reduction of salt intake � Increase in fruit and vegetable intake and decrease in saturated and total fat intake

Stroke mortality by BP and age
 SBP")
Lifestyle Modifications To Manage Hypertension Modification Weight reduction (BMI 18. 5~24. 9 kg/m²) SBP Reduction 5~20 mm. Hg/ 10 kg Diet 8~14 mm. Hg Dietary sodium reduction (<6 g/d salt) 2~8 mm. Hg Physical activity (30 min, most of the days of the week) 4~9 mm. Hg Moderation of alcohol consumption (<2 drinks/d) 2~4 mm. Hg

Intervention of Hypertension
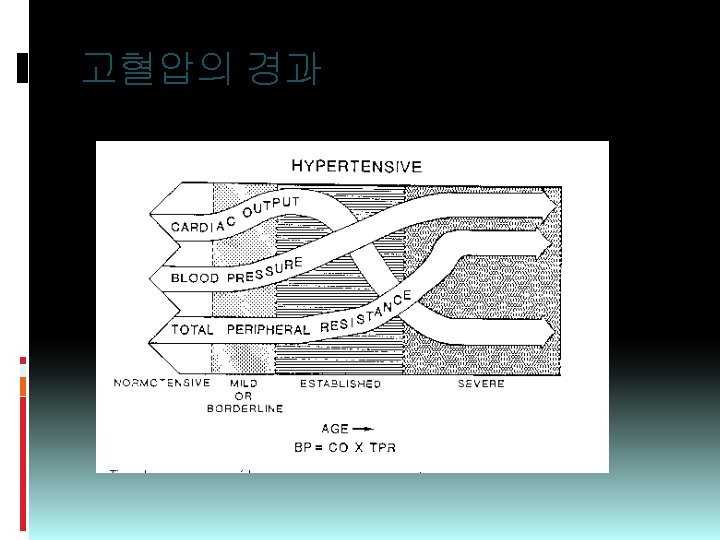

Hemodynamic Effects of Dynamic Exercise Elevated SBP is consistently maintained with increasing VO₂(BP = ↑↑CO × ↓SVR) SBP responses are steeper than normotensive persons SBP change : 150 mm. Hg(rest) → 250 mm. Hg(exercise) in Stage 1 pt’s Stage 2 : more marked ↑HR, less rise in SV → Rise in CO (CO = SV × HR) Stage 3 : subnormal ↑CO, ↑↑HR, PApr↑

Hemodynamic Effects of Static Exercise Stage 1 & 2 Isometric exercise similar to normotensive controls Elevated BP at rest Absolute increase of SBP/DBP is the same HR & CO : mod ↑, SVR unchanged Isometric exercise gives heavier strain on vascular system than dynamic exercise. (short duration) After exercise, BP drops within 15 -30 sec.

Hemodynamic Response to Exercise Hemodynamic factors SBP DBP HR Dynamic exercise Static exercise ↑~↑↑↑↑ ↔~↓ ↑~↑↑↑↑ ↑~↑↑ Mean BP ↔~↑ ↑~↑↑↑ SVR 0~↓ 0~↑

Indications of Exercise Testing 1. Hypertensive pattern in normotensive at rest 2. Insufficient BP response with ↓myocardial ft 3. Support the need of Tx in mild HT 4. Efficacy of Drug therapy during exercise 5. Inadequate/absent BP increases during exercise 6. Ensure the physical working capacity is not impaired by drug

The Risks of Exercise Test Complication rate 18. 4 per 10, 000 tests Common in pre-existing CHD Exclusion Resting BP > 200/115 mm. Hg Exercise SBP > 260 mm. Hg

The Effect of Exercise �Mechanism ↓ Circulating norepinephrine ↑ Endothelium-dependent vasodilation ▪ Through ↑ NO production (Goto C, et al. Circulation 2003; 108: 530) Improve hyperinsulinemia Improve renal function Reduce weight

Exercise Prescription Mode : Aerobic exercise Duration : 30~60 min Frequency : 3~7 days/week Intensity : 50~85% MHR RPE(Ratings of Perceived Exertion) 11~13 700~2000 Cal/week Strength training Circuit training : high rep, low resistance

Weight reduction Obesity increases both preload and afterload, resulting in hypertensive effect Preload ↑intravascular volume ↑total peripheral resistance ↑LV preload Afterload ↑Central NE production ↑total peripheral resistance ↑LV afterload

Other Nonpharmacological methods High fiber diet Low saturated fat diet Elimination/moderation of alcohol consumption < 2 drinks per day Relaxation techniques Biofeedback Stress management Muscle relaxation techniques

Drugs and Exercise Drug BP at Ex_submax CCB ↓ ↔↓ ↔ ↔ βblocker ↓ ↓ αβblocker ↓ ↓ ↔ ↔ Diuretics ↓ ↔ ↔ ↔ Vasodilator ↓ ↓ ↔ ↔ αAgonist ↓ ↔ ↔ ↔ ACEI BP at Ex_max VO₂max Effect on Physical Act.

Pharmacotherapy General principles All antihypertensives permit normal exercise response except beta-blockers Best choices for endurance athletes ACEI : ↑ SV, ↓ HR ARB Alpha blockers : ↓ TPR, first dose effect Beta blockers Good for intermittent exercisers/untrained athlete ↓↓HR, ↑TPR Diuretics ↓PV, ↓SV, ↓CO CCB ↓TPR, ↓LV contractility

Exercise and BP Meta-analysis of RCT Mean reduction of BP : 4~6 / 3 mm. Hg (Stewart KJ et al. Arch Intern Med 2005; 165: 756 Dickinson HO et al. J Hypertens 2006; 24: 215) Swimming training : lower SBP 6 mm. Hg(150→ 144) (Tanaka H et al. J Hypertens 1997; 15: 651) Abstention of exercise → return of BP to preexercise level Fall of BP : dependent upon the intensity than frequency Ex 8 weeks at 50% VO 2 max 2×/w 60 min : ▼ 12/6 mm. Hg As much as Ex 5 ×/w 120 min (Ishikawa TK et al. Am J Hypertens 2003; 16: 629)

Possible predictor of adverse events � 정상 혈압이라도 운동으로 인한 혈압 상승 과다 : 추후 고혈 압 위험 증가 Framingham Heart Study, ↑DBP resp(>95 %ile) → predictive subsequent HT ↑SBP resp during recovery in men →predict HT (Singh JP et al. Circulation 1999; 99: 1831) � Exaggerated ↑BP resp prone to develop LVH (Gottdiener JS, et al. Ann Intern Med 1990; 112: 161) � CV mortality increased 2000 healthy men (40 -59 y) 6 min bike test CV death at 16 yr : two-fold with post-ex SBP >200 mm. Hg (Mundal R, et al Hypertension 1994; 24: 56)

비만아동에서의 운동 사춘기 이전 만 9세 비만아 44명 RCT 60분 3/wk, 3개월 운동 vs inactive 결과 운동군 대조군 SBP * -1. 9 (11. 8) 4. 4 (10. 3) DBP * -1. 3 (9. 7) 4. 7 (7. 0) VO 2 max * 1. 9 (3. 5) -1. 6 (4. 6) IMT of CCA -0. 09 (3. 75) 1. 13 (4. 40) FMD (%) -0. 59 (3. 13) 0. 13 (2. 61) HT rate * -12% -1% (Nathalie J. J Am Coll Cardiol 2009; 54: 396)
 with HT 20 min")
Resistance Exercise in Hypertensives � 15 workers (42. 9 y) with HT 20 min TR(70~80% max) (treadmill) 20 min Circuit RE(20 rep at 40%RM) Control session �결과 TR RE SBP * -11. 1 (7. 6) -12. 6 (7. 3) DBP * -4. 0 (6. 4) -9. 0 (7. 0) Post-ex hypotension (Marcio RM J Strength Cond Res 2009; 23: 2331) Up to 7 hours

Exercise capacity and all-cause mortality in prehypertensive men 4, 478 prehypertensive men at VA centers 4 fitness quartiles by GXT 9 years follow-up Results Ex capacity : strong predictor of all-cause mortality Adjusted mortality ▽ 15% for every 1 -MET▲ 18% for younger, 12% for older Inverse correlation betn fitness & mortality (Kokkinos P. Am J Hypertens 2009; 22: 735)
 � 937 hypertensive pt’s with")
고혈압 환자에서 운동의 심장 영향 및 심혈관결과 (LIFE study) � 937 hypertensive pt’s with LVH Physically active: > 30 min, twice/w Intermediate : < 30 min, 2×/w Sedentary �Results 운동군 : low HR, wt, BMI, LVmass Cox regression ▪ 운동군 CV death OR=0. 50(0. 22 -1. 10, NS) ▪ Stroke OR=0. 26(0. 13 -0. 49, p<0. 001) ▪ MI OR=0. 79(0. 35 -1. 75, NS) (Boman K. Eur J Cardiovasc Prev Rehabil 2009: 16: 242)

Risks of exercise for DM Hypoglycemia, if with insulin or oral agents - exercise induced hypoglycemia - late-onset postexercise hypoglycemia Hyperglycemia after very strenuous exercise Hyperglycemia patients and ketosis in insulin-deficient Precipitation or exacerbation of CVD : pectoris. MI. Arrhythmias. Sudden death. Angina Cont’d

Risks of exercise for DM Worsening of long-term complications of DM : - Prol. retinopathy : Vitr. hemorrhage. Retina Detach. - Nephropathy : Increased proteinuria - Peripheral neuropathy : Soft tissue/ joint injury - Autonomic neuropathy : Decreased cardiovascular response to exercise. Decreased maximum aerobic capacity. Impaired response to dehydration. Postural hypotension.

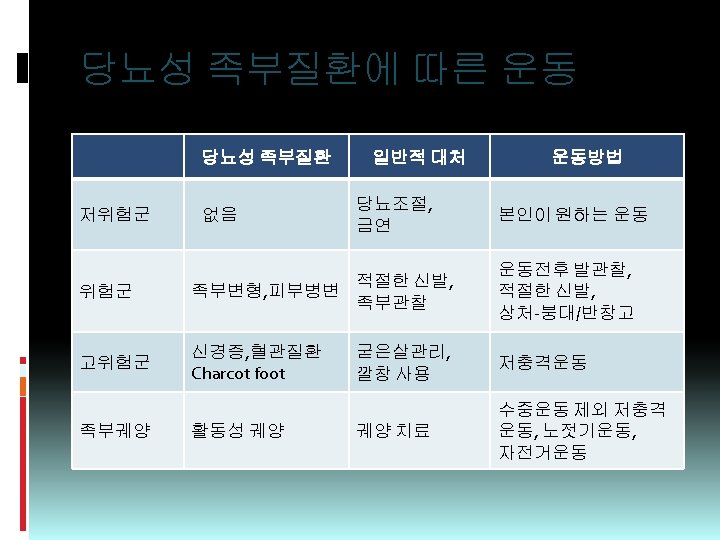
당뇨병성 말초신경병증 금기 Treadmill, Prolonged walking Jogging, Step exercises 권장 : Swimming, Bicycling, Rowing Chair exercises, Arm exercises Other non-weight-bearing exercises

운동 상대적 금기 혈당 ≥ 290 mg/dl 케톤뇨 > 36 mg/dl beta-hydroxybutyric acid > 9 mg/dl 저혈당 탈수
- Slides: 81