Greater Manchester Cancer Implementation of Prehab 4 Cancer

Greater Manchester Cancer Implementation of Prehab 4 Cancer Dr John Moore Clinical Director for Prehab and recovery

John. moore@mft. nhs. uk @mysurgeryandme

Improving Surgical Care www. erasplus. co. uk

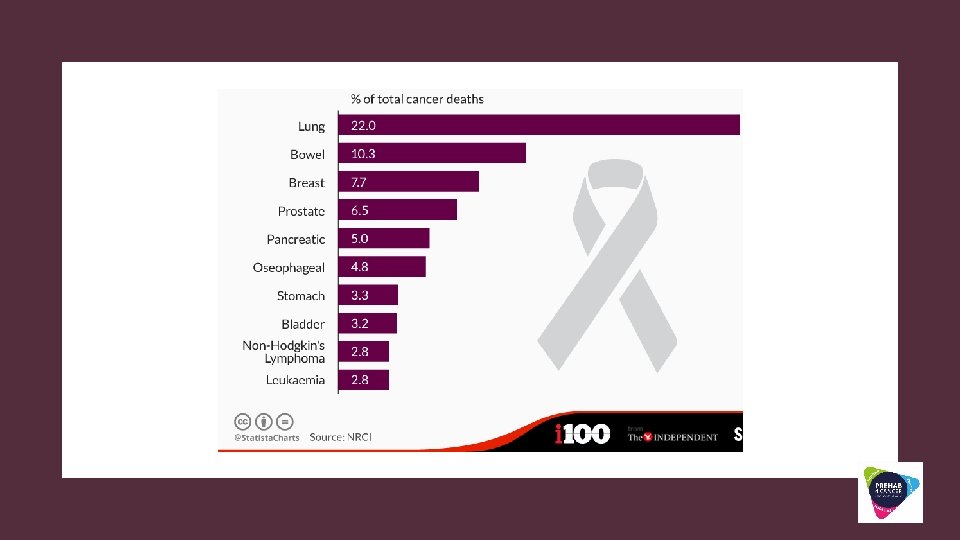
GM Cancer Prehab and Recovery @Prehab 4 cancer for Lung

WHAT CAN WE DO

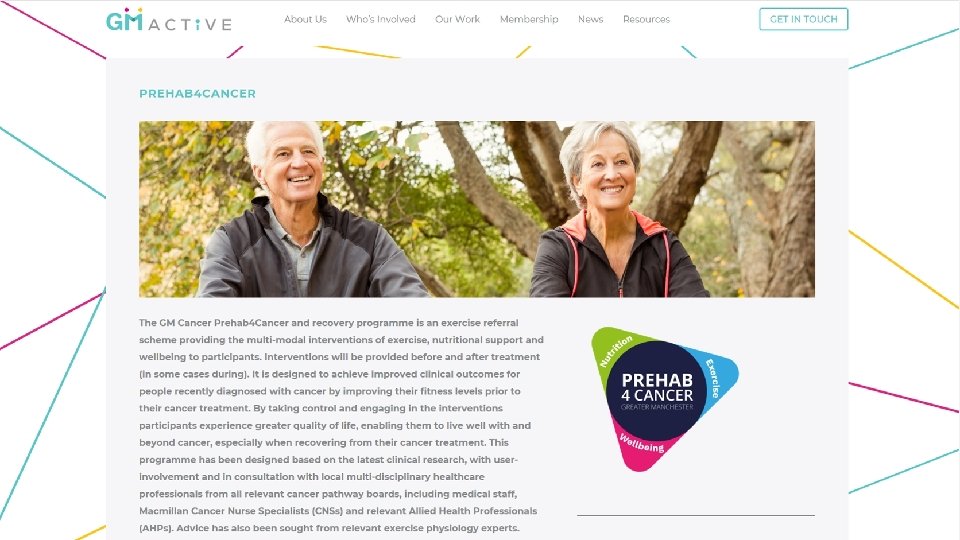
GM Cancer Prehab and Rehab Psychological Nutritional Exercise Intervention FITT Regional and National expert group Single referral point 48 hour reply GM wide coverage Deliver Prehab to 2000 patients Upper GI Lung Colorectal Head and Neck Universal prehab World leading outcomes Specialised prehab Prehab 4 cancer

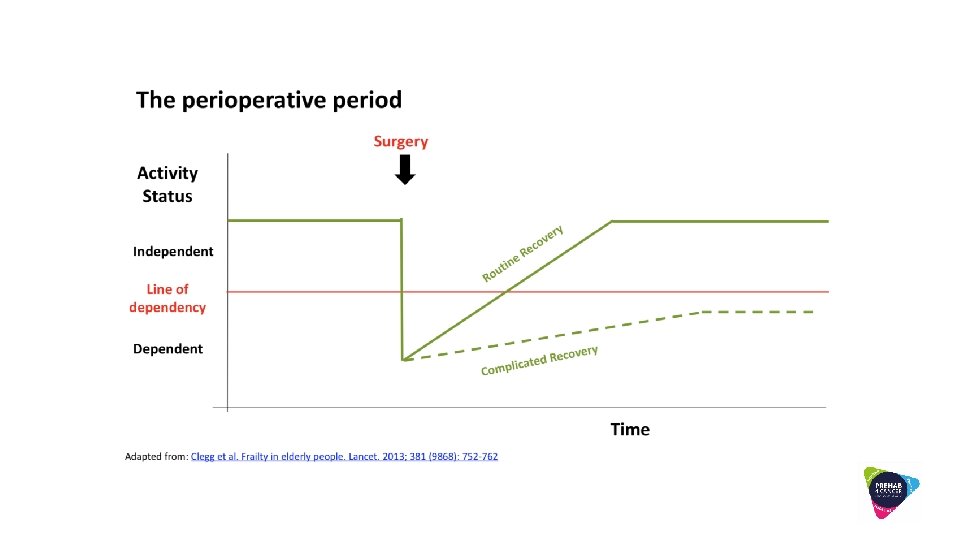
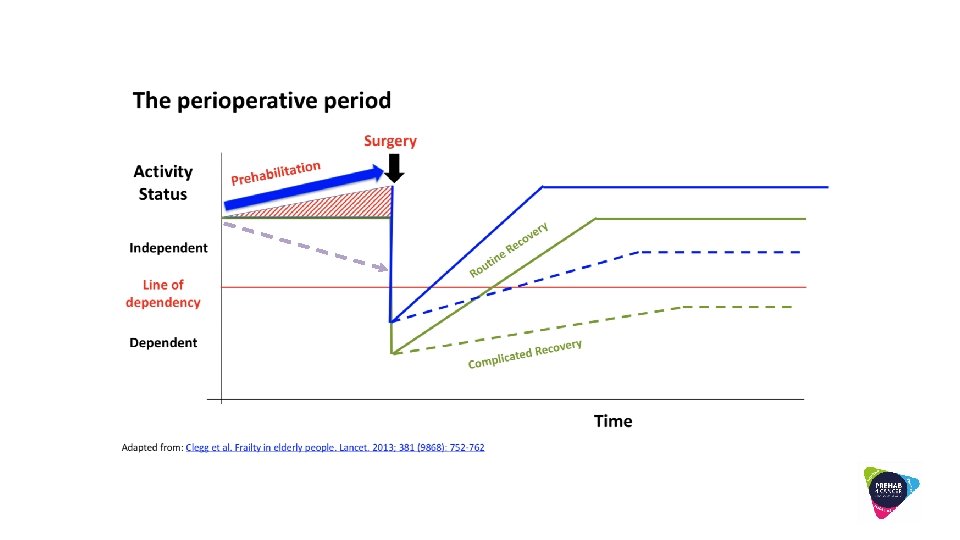
Days FITNESS Elective Surgery Complication s Weeks Later Complication s Failure to recover HIGH 2 year mortality ELECTIVE CANCER SURGICAL PATIENT 2 -YEAR MORTALITY

VA hospitals >100, 000 patients 19901991 NASQIP Review of 8 operations and complications Colorectal Upper gi Vascular Over eight years follow-up

DUTCH STUDY 4400 PATIENTS 6 YEAR FOLLOW-UP • 45% having medium – high risk surgery • Looking at what patients died from

WHY PATIENTS DIE LATER AFTER SURGERY Normal recovery Loss of lean muscle Altered immune function Complicated recovery • Cytokine and oxygen free radical induces apoptosis – reduces organ function • Accelerated

Immediate Reduced functional reserve Longer term consequences Peri-op cardiac event reduces cardiac function Persistent peri-operative inflammation accelerates cardiovascular atherosclerosis and plaque instability Cognitive dysfunction CVA Longer term cognitive dysfunction CVA Acute Neuromuscular weakness Prolonged disability

WHAT CAN WE DO Improve care delivery of surgical services =ERAS+/ERAS Patient and family preparation and recovery = PREHAB

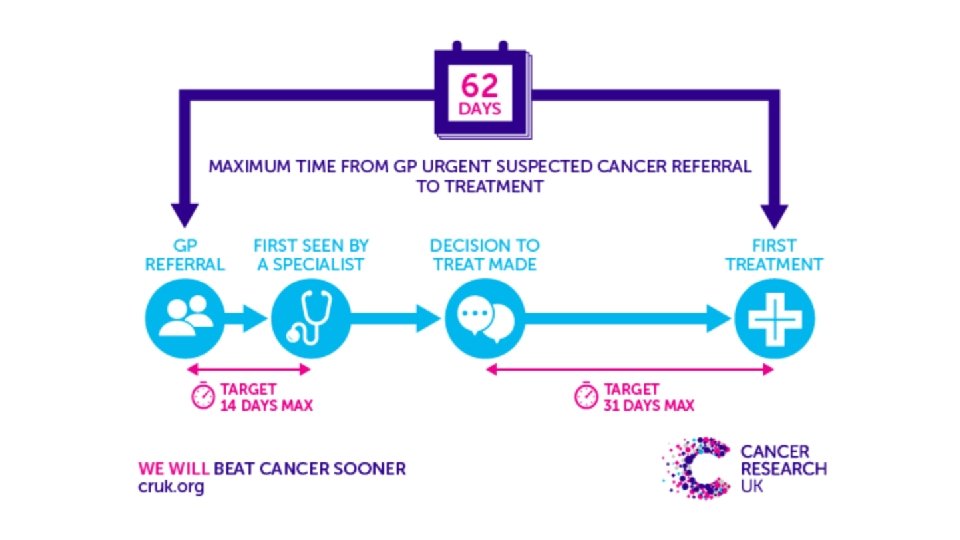
Measure MORBIDITY HOSPITAL THE CANCER SURGICAL PATHWAY 90 day mortality 2 year mortality QOL COMMUNITY PATIENT OUTCOME S Prehab 4 cancer NITY REHAB PATHWAY innovation

Improving Surgical Care www. erasplus. co. uk

OUR TEAM

ERAS+ PREHAB 01 PREHAB 02 OPTION HOSPITAL REHAB 03 05 HOSPITAL 04 OUTCOMES 06

OPTIMISING MEDICAL HEALTH

I COUGH Incentive spirometry Coughing Oral Healthcare Understanding Getting out of bed Head of bed elevation I COUGH: reducing postoperative pulmonary complications with a multidisciplinary patient care program Cassidy MR JAMA Surg. 2013 Aug; 148(8): 740 -5.

SURGERY SCHOOL

ACTIVE CHEST TRAINING Surgery is a big thing for your body and we need to get you as fit as possible NUTRITION Your body is getting ready for Surgery - need to eat well Lets get your lungs fit and ready for surgery FAMILY AND FRIENDS YOU will benefit from good support to help with your prep and recovery

 Moore et al Anaesthesia 72(3)")
50% reduction Moore et al, Anaesthesia 2016 (in print) Moore et al Anaesthesia 72(3) · March 2017 3 day LOS reduction = 500 K

>70% + would like to trial digital support It needs to be simple

PREHAB PREPARATION FOR PLANNED BODY STRESSOR PHYSICAL ACTIVITY NUTRITION WELL-BEING

A systematic review of trials investigating the effectiveness of preoperative exercise for patients undergoing a range of oncological surgery Most benefit for Lung Cancer Surgery
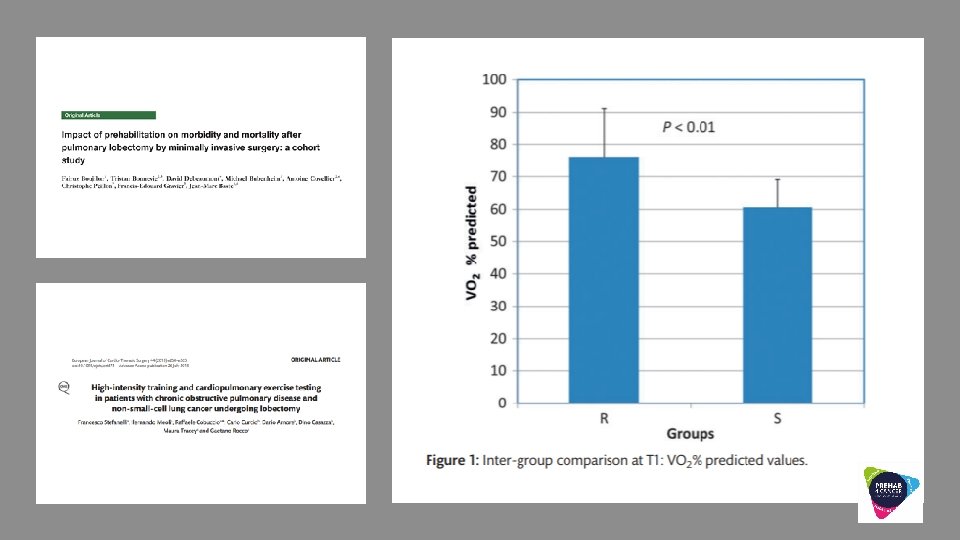

SUMMARY OF PREHAB EVIDENCE SO FAR • We can improve fitness but in studies difficult to relate to improved outcomes and tends to excludes least fit for prehab • Highly likely stronger benefit in higher risk patients. • We need multi-modal prehab

DOSE O F EXERCI SE INTERVENTI ON FITT P RINC IPLE Frequency Intensity Time – duration of session Type of exercise

GM Cancer Prehab and Recovery @Prehab 4 cancer for Lung

WHAT CAN WE DO

SURGICAL RISK High Medium Low More frail 50 -60% complications Highest mortality short and long-term

PREHAB INTERVENTION Can we get NHS England to recognise period of PREHAB as care for these patients Specialised Targeted Universal More frail 50 -60% complications Highest mortality short and long-term

Prehab 4 Cancer team led by Kirsty and her team 60 level 3 -4 PT trained in the exercise intervention Exercise combination of CVS endurance and strengthening Supported by UK Active Progressive programme KPI - Aiming for 3 sessions minimum per week Exercise Intervention FITT Regional and National expert group Psychological Nutritional

GM Cancer Prehab and Rehab Lung Cancer Surgery Phase 1 Evaluation points (6 MWT, Strength, EQ 5 D, self efficacy) PREHAB 01 90 day hospital length of stay PREHAB 2 year mortality

GM Cancer Prehab and Rehab Surgery Phase 1 Prehab 4 cancer launches 25 th April 115 patients referred to programme since launch >90% patients taking part 14 evaluation sessions across GM Reason for Not Participating: Patient too high risk for exercise in community Unable to contact patient Already active with private gym and declined the offer Declined the programme

GM Cancer Prehab and Rehab Lung Cancer Surgery Phase 1 Referring Hospitals Number of Referrals 8 Prehab 4 cancer launches 25 th April 7 6 5 4 34 patients referred to programme 3 2 >90% patients taking part 1 0 Bolton (1) Referred Intends to Participate Participating Not Participating Left Early Bury - Fairfield (1) MRI (6) 1 1 5 1 Wythenshawe Wigan - RAEH Salford Royal (6) (8) (10) 1 3 2 2 3 4 7 1 1 Stepping Hill (2) 1 1 For less fit patients we are only averaging 2. 2 sessions/week Reframe this as Exercise Dose

GM Cancer Prehab and Rehab Non-surgical Lung Cancer Chemo/Dxt Phase 1 Evaluation points (6 MWT, Strength, EQ 5 D, self efficacy) 90 day hospital length of stay 2 year mortality

GM Cancer Prehab and Rehab Non-surgical Lung Cancer Chemo/Dxt Phase 1 Evaluation points (6 MWT, Strength, EQ 5 D, self efficacy) PREHAB 01 90 day hospital length of stay PREHAB 2 year mortality

GM Cancer Prehab and Rehab Lung Cancer Surgical and then chemo Phase 1 Evaluation points (6 MWT, Strength, EQ 5 D, self efficacy) PREHAB 01 PREHAB
- Slides: 53