Graded Dose Response Curves Potency the drug concentration

 A=fentanyl C=morphine")

 indicated in the graph from most to least")
 indicated in the graph from most to least")

?")


 on the dose-response curve?")
 on the dose-response curve?")








 when compared to")










")

- Slides: 34
Graded Dose –Response Curves
Potency: the drug concentration resulting in half the maximal effect (EC 50) A=fentanyl C=morphine D= codeine
Efficacy: the maximal effect of a drug
Homework question 1. Order the drug(s) indicated in the graph from most to least potent. 2. Order the drugs from most to least efficacious.
Homework question 1. Order the drug(s) indicated in the graph from most to least potent? P: A>B=C>D 2. Order the drugs from most to least efficacious? E: A=B=D>C
What is a competitive antagonist?
What is a competitive antagonist (inhibitor)?
Review Q: South American hunters once used tubocurarine or curare on poison arrows. Although the drug will very quickly paralyze an animal impacted with an arrow, the meat can be eaten with no observed adverse effects. Why?
What would be the effect of a competitive antagonist on the dose-response curve?
What would be the effect of a competitive antagonist (inhibitor) on the dose-response curve?
What would be the effect of a competitive antagonist (inhibitor) on the dose-response curve? Note that with a competitive antagonist, the maximal effect can be reached by increasing the agonist concentration.
What is a non-competitive antagonist ?
What is a non-competitive antagonist ? https: //www. slideshare. net/rajud 521/drug-actions How would a non-competitive antagonist be expected to change a graded response curve?
Note that with a non-competitive antagonist, the maximal effect will never be reached no matter how high the agonist concentration.
Lecture 20: Individual Responses to Drugs Person A Person B Person C
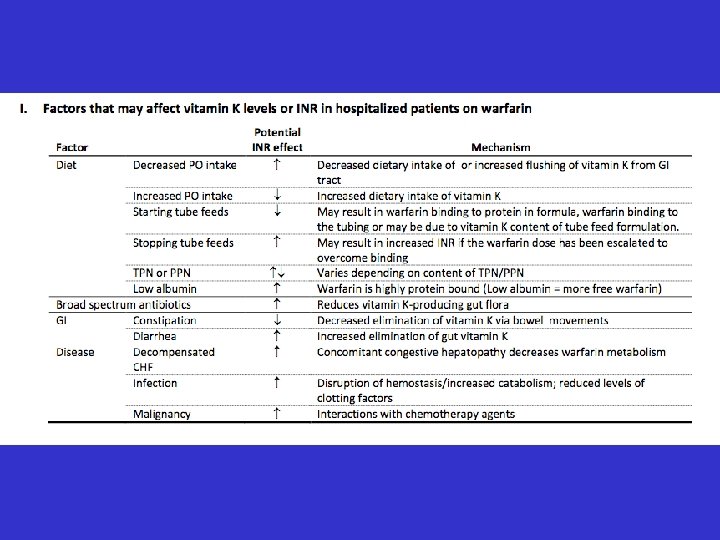
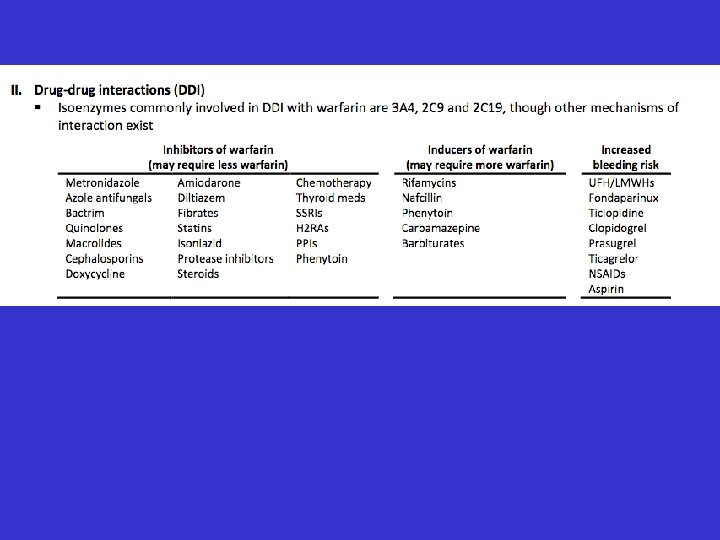
Why is there significant interest in identifying the causes of individual variation to warfarin?
Individual Responses to Drugs Q 1: What are some possible reasons for individuals not responding identically to warfarin?
Individual Responses to Drugs -Pharmacogenetics Ø gene Ø allele Ø polymorphism Ø pharmacogenetics
How much genetic variation is there in the human species?
Human variation Ø Humans have relatively little genetic variation (~0. 5%) when compared to many other species Ø Genetic bottleneck around between 50, 000100, 000 years ago decreased population to 300010, 000 individuals, from which we all can trace origin. Ø One bottleneck is postulated to have resulted from a massive volcanic eruption (Toba eruption) in Indonesia that triggered a ten-year volcanic winter ~ 70, 000 years ago.
23 and me
What is the basis for 23 and me stating that I am 68. 5% British and Irish?
Human migration Ø Q: What are some possible causes of isolated human populations having different alleles or a different frequency (abundance) of specific alleles?
Human migration out of Africa Ø Several waves of migration between 70, 000 - 200, 000 years ago Ø Interbreeding with Neaderthals (and Denisovans) which migrated ~600, 000 years ago ; homo erectus migrated ~ 1. 8 million years ago
What are some possible causes of isolated human populations having different alleles or a different frequency (abundance) of specific alleles? Ø founder effect: representation initially skewed in small migrating populations Ø genetic drift in small isolated population Ø selective advantage of particular alleles in a given environment Ø breeding with other groups (Neanderthals etc) that had migrated into specific region at an earlier time
In what types of genes would you expect to have the greatest impact on warfarin dosing?
In what types of genes would you expect to have the greatest impact on warfarin dosing? How would you test this?
Association studies n engl j med 364; 12 nejm. 1144 org march 24, 2011
Genetic variation impacting dosing of warfarin Ø Identified risk alleles only account for at most 45% of individual variation Ø clinical benefit of dosing based on pharmacogenomics had only limited success Ø What parameter would physicians monitor in determining dosage?
Are my 23 andme results by themselves of any use in predicting adverse reactions? Frequency of CYP 2 C 9 allele in different populations
Genetic testing-IRINOTECAN (Camptosar)
Patients with Reduced UGT 1 A 1 Activity. Individuals who are homozygous for the UGT 1 A 1*28 allele are at increased risk for neutropenia following initiation of CAMPTOSAR treatment. A reduced initial dose should be considered for patients known to be homozygous for the UGT 1 A 1*28 allele (see DOSAGE AND ADMINISTRATION). Heterozygous patients (carriers of one variant allele and one wild-type allele which results in intermediate UGT 1 A 1 activity) may be at increased risk for neutropenia; however, clinical results have been variable and such patients have been shown to tolerate normal starting doses. UDPGlucuronosyltransferase CAMPTOSAR