GP Update on Stoma Care Heather Wilson Stoma



































- Slides: 36
GP Update on Stoma Care Heather Wilson Stoma Care Nurse Specialist Gateshead Health NHS Foundation Trust
Aims of the Session • To give a brief overview of stoma care management and the support of the patient/family/carer • Discuss the role of the Stoma Care Nurse Specialist • To discuss a variety of stoma problems that patients may face • To outline the management of these problems
History • First surgical stomas were created on battle casualties in the early 1700 s • No documentation of the specific care of stoma patients in the nursing profession press until the late 1930 s (Plumley, 1939) • The first stoma therapist was not a nurse , but a patient. Norma Gill, Ohio, USA • In the UK Barbara Saunders a ward sister, set up the first stoma clinic in 1969. • 1971 saw the first stoma care nursing posts
Types of Stomas • Over 80, 000 people in the UK living with a stoma • Stoma greek word for mouth • Colostomy (wet colostomy) • Ileostomy • Urostomy • Loop or end, permanent or temporary
End Colostomy
End Ileostomy
Loop Ileostomy
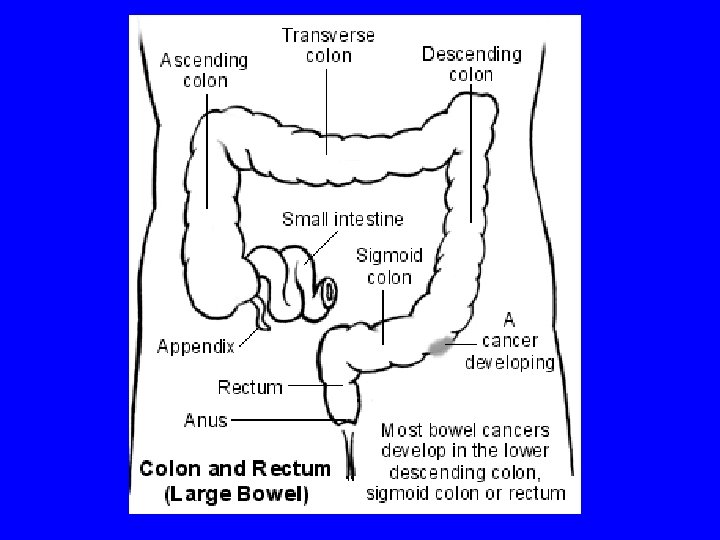
Reasons for needing a stoma • Varied • Cancer – bowel/rectum or bladder • Inflammatory Bowel Disease – Crohn’s Ulcerative Colitis • Diverticular Disease • Congenital abnormalities • Bowel ischaemia • Irradiation damage, fistula formation
Stoma Care Nurse Specialist • • Some are Colorectal Nurse Specialists Present in all major hospitals in the NE Some are community based Strong network, regional meetings, patient open days, study events, collaborative working/patient referrals • Sub specialist nurses in Paediatrics and Urology
• Senior Nurse who has undertaken formal training/examination in the field of stoma care/colorectal • Clinical and consultative role • Patient advocate, support and education • Teaching • Management, research, audit, change agent
Stoma Care Management • Team approach – specialist nurses, ward and community nurses, medical staff, patient, carers and family • Practical Support – how to look after the stoma and surrounding skin, dietary advice, types of appliances, holiday advice • Psychological Support – emotional reaction to this type of surgery, lifestyle issues, sexuality and body image • Preoperative preparation including siting • Post operative support and education • Continued support once patient is discharged into the community • Aim is for the patient to become an‘expert’ in stoma management and adapts to life with a stoma
Stoma Problems Divided into 3 main areas 1. Problems in the management of a stoma e. g. hernia, prolapse, stenosis 2. Skin conditions which may arise due to the stoma or wearing of an appliance 3. Psychological issues
Post op stoma shrinkage • 6 to 8 weeks for stoma to shrink in diameter and spout. Patients may need to change appliance type e. g. Convex • Need regular review by stoma nurse in the first 2 to 3 months.
Colostomy • • • Effluent less corrosive to the skin Usual formed stool, closed pouch, 3 x daily Transverse colostomy may need drainable Some patients may opt for irrigation Constipation –diet, fluids, drugs, age, mechanical e. g. Hernia, stricture, adhesions • Oral laxatives/microlax enemas/suppositories
• • Diarrhoea – right sided/transverse stomas Chemotherapy/radiotherapy Infection – stool sample Drugs, diet, stress, malabsorption, disease e. g. crohn’s, cancer, sub acute obstruction • Imodium
Ileostomy • Effluent very corrosive to skin. 1 -2 days. • Output should be “porridgy”, 350 -600 mls per day. Imodium. • Increased/fluidy output –infection, diet, drugs • Obstruction- foods high in cellulose, adhesions, strangulated hernia, stenosis • Stoma oedematous, cramps, fluid effluent then ceases
• Loop ileostomy can be difficult to manage due to its odd shape, mucus from distal part • High output ileostomy – electrolyte drinks, TPN, appliance type • Chemotherapy treatment- increasing stoma activity, skin more sensitive, reduced feeling in patient’s fingers
Urostomy • Infection – clean specimen using a fine catheter, or place collecting bottle under clean stoma. Mucus shreds in the urine is normal • PH of the urine should be kept between 5 and 7. Ascorbic acid 100 mg, cranberry juice • Phosphate deposits, Chronic papillomatous dermatitis around urostomies. 50% household vinegar soaks, appliance review.
Necrosis / Sloughy Stoma • • Early post op complication, too tight appliance Compromised blood supply Difficult surgery Post op stoma bridge Ill fitting appliance If superficial will slough off Use intrasite gel or orabase paste to aid removal of slough • Refer to surgeon in severe cases
Necrosis and Dehiscence
Stenosis • Narrowing of the lumen of stomal outlet • Healing of necrotic tissue, dehiscence of stoma, poor surgical technique • Secure appliance • Patient may be taught to dilate • Surgical revision
Retraction • Bowel under tension • Surgical technique, post op weight gain • Can be difficult to manage –skin damage/leaks/difficult for patient to see stoma. Appliance review. • Convex products, rings, pastes, belt • May need to change pouch more frequently • Surgery may be indicated
Parastomal Hernia • Affects 40% plus an increasing problem • More common in older patients • Loss of muscle tone • Appliance review • Support garment • Observe patient • Surgery
Prolapse • Defined as when a length of bowel prolapses out onto the exterior of the abdominal wall • More common in transverse loop colostomies (larger stoma) • Fit larger appliance • Reduce prolapse • Surgical intervention
Pancaking • Colostomy effluent does not fall to the bottom of the pouch, collects around the stoma. Can be difficult to manage. • Leaks, frequent pouch changes • Sore skin • Odour issues – blocked filter • Cover filter, tissue paper in pouch, lubricating gel, diet, 2 piece pouch
Trauma to Stoma • Many causes • Most common ill fitting appliance • Cause laceration on stoma. Bleeding. • Usually heals quickly • Use of special powders e. g. orahesive, hollister • May need suturing
Over Granulation • Occurs at the junction between stoma and skin • Can occur at any time • Probably a reaction to irritation • Bleeding • Soreness • Powders • Silver nitrate • Liquid nitrogen
Skin Problems • Very common • 1/3 of people with colostomies • 2/3 ileostomy or urostomy pts experience skin problems Lyon & Smith, (2001) • Many causes - poor fitting appliance, flush stoma, poorly sited stoma, hernia, weight gain, pre-existing skin condition e. g. eczema (1)
Skin Problems • Allergic reaction • Allergic contact dermatitis • Patch test. Change pouch type. • ? Refer to dermatologist • May need topical steroid. Lotion, inhalers, nasal spray (2)
• • Check stoma spout, abdomen examination Check stoma effluent Appliance review May need barrier spray, wipes or powder to heal skin • Use of accessories e. g. Rings/paste , skin creases, dips
Patient Impact • Stoma formation and stoma complications can effect the physical, psychological, sexuality and social well being of the patient • Loss of self-esteem • Change in body image • Loss of confidence • Social recluse • Affecting work, relationships, social activities / holidays • Regular support especially early in recovery period is vital
Patient Support • Healthcare Professionals • Clinical psychology • National and local patient support groups e. g. Urostomy association • One to one patient support • Stoma appliance manufacturers, pharmacy, dispensing appliance contractors
Conclusion • Stomal problems should be assessed holistically • Using multi-disciplinary team • No one simple answer to any of the complications • Patients need easy access to specialist nurse for ongoing advice and support • Nurses need to involve other specialists where appropriate e. g. tissue viability nurse, dietitian • Dealing promptly and affectively with a problem will minimise patient anxiety and promote adaptation.
Conclusion • Stoma care management can be varied, challenging and at times complex. • Careful assessment, prompt management and good communication within the team is essential, as is ongoing patient support. • The reward is a confident patient who is able to just get on with life.
• Thank you for listening • Any questions ?