Good Morning 6 June 2003 Uremic Bleeding Pathogenesis

Good Morning 6 June 2003

Uremic Bleeding: Pathogenesis and Therapy 麻醉科 林子富
 § purpura (Bright 1836) §")
Clinical Manifestations § renal disease and bleeding (Morgagni 1764) § purpura (Bright 1836) § hemorrhagic pleural effusion and hemorrhagic pericarditis from serosal irritation

§ characterized by ecchymoses and prolonged bleeding from puncture sites and mucous membranes (epistaxis, GI and GU tract bleeding) § Subdural hematoma (hypertension, anticoagulation with heparin) § Menorrhagia



Laboratory Evaluation • The only clinically reliable test available to evaluate the risk of bleeding in uremic patients and their response to therapeutic interventions is bleeding time. • Mild thrombocytopenia may develop in uremia, but it is not sufficient to account for the abnormality in hemostasis • Abnormalities in the prothrombin time(PT) or partial thromboplastin time (PTT) may occur but usually denote other associated clotting problems or drugs.

Therapy § Dialysis § Uremic plasma elicits changes in the function of platelets from normal donors. ( toxins, inhibitory peptides) § Peritoneal dialysis: less bleeding risk ( lack of systemic heparinization and of platelet activation by contact with a bioincompatible membrane ) § preferred over hemodialysis in the high-risk patient with active bleeding or subdural hematoma

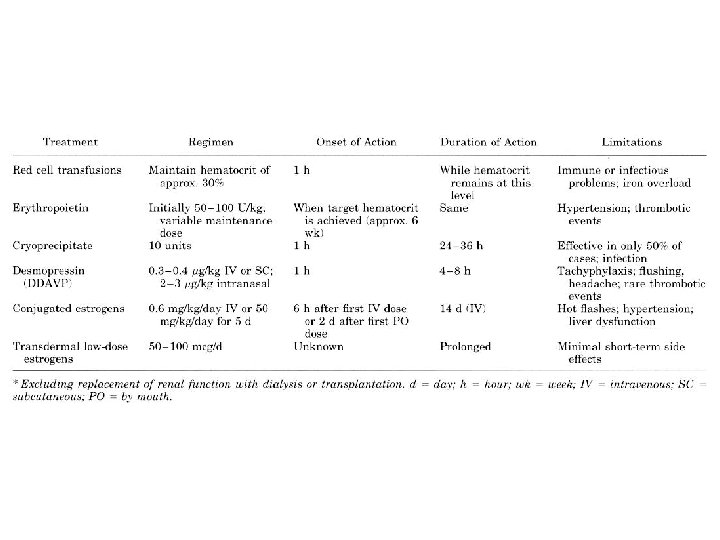
Therapy § Cryoprecipitate § rich in v. Wf and fibrinogen, was found to improve the uremic bleeding diathesis § effect is rapid, but not invariably present. § Within 1 hour after infusion of approximately 10 units, there is normalization of bleeding time in about 50% of uremic patients. § As many as 50% of patients fail to respond. § risk of transmission of infectious agents
 or DDAVP § a derivative of vasopressin with")
Therapy § Desmopressin (1 -deamino-8 -D-argininevasopressin) or DDAVP § a derivative of vasopressin with less vasoconstrictor effect, has been used successfully in some forms of von Willebrand disease § Intravenous administration of 0. 3 to 0. 4 µg/kg over 20 to 30 minutes improves bleeding time within 1 hour, and this effect is maintained for 4 to 8 hours § induces the release of v. Wf from its endothelial storage pools § Repeated use of desmopressin may deplete these stores of v. Wf, resulting in tachyphylaxis after two or three doses

Therapy § Estrogen § von Willebrand disease and hereditary hemorrhagic telangiectasia sometimes improve during pregnancy § The beneficial effect of high-dose estrogens has been attributed to the stimulation of an alternative enzymatic route which reduces the L-arginine concentration in cells. § 0. 6 mg/kg per day IV for 4 or 5 days, or oral estrogens, 50 mg/kg per day, cause slower but more sustained improvements in bleeding time § The onset of action is about 6 hours after the initial intravenous dose or 2 days after initiation of oral treatment

Therapy § Correction of Anemia § Unless there is coincidental severe thrombocytopenia, platelet transfusions are generally ineffective. § transfusion of red cells corrects the prolonged bleeding time promptly after a hematocrit of about 30% is reached § The risks associated with repeated red cell transfusions can be circumvented with human erythropoietin therapy. § 50 to 100 U/kg 3 times per week can improve the anemia of renal insufficiency to the target

Summary § multifactorial nature ; flexible therapeutic strategy § Bleeding time is the best guide to assess the bleeding risk and to monitor the efficacy of treatment in a given patient. § adequacy of dialysis and the hematocrit influence the bleeding risk § erythropoietin to avoid the risks associated with transfusions § prophylactic red cell transfusion for actively bleeding or urgent surgical intervention § desmopressin for short-term interventions such as vascular access placement or renal biopsy

Summary § recurrent gastrointestinal or other internal hemorrhage occurs, desmopressin may still be useful acutely, but the sustained effect of estrogens makes them a more appealing option § elective surgery, particularly if the risks of bleeding are high (eg, in orthopedic surgery), pretreatment with estrogens is usually advisable § Emphasis on dialytic adequacy and appropriate hematocrit should not be overlooked when therapeutic interventions

References 1. Uremic Bleeding: Pathogenesis and Therapy. The American Journal of the Medical Sciences. Volume 316(2) August 1998 p 94 -1041) 2. Management of Bleeding with Uremia and Liver Disease. Current Opinion in Hematology. Volume 6(5) Sep. 1999 P 329 -333 3. Estrogen for Uremic Bleeding. Hospital Pharmacy. Volume 33(8) Aug. 1998 P 999 -1005

Have A Nice Day
- Slides: 17