Goals of Therapeutic Exercises Assis Prof Neveen Abdel


Goals of Therapeutic Exercises Assis. Prof. Neveen Abdel Latif

Objectives At the end of this lecture you should able to 1. Identify goals of Therapeutic Exercises 2. Investigate Scientific Bases of Therapeutic Exercises 3. Recognize Types of Movement 4. Define Forms of Muscle Contraction 5. Investigate Cooperating Muscle Groups

Goals of Therapeutic Exercises 1 - Improves range of motion 2 - Reduce Pain 3 - Restore joint flexibility 4 - Improve muscle mass, strength & endurance 5 - Reduction of limb edema 6 - Increase body function

7 - Improves balance control 8 - Increases cardiovascular strength and endurance 9 - Helps preventing further injury 10 - Aid in weight loss 11 - Gain self confidence.

Axial & Appendicular Skeleton

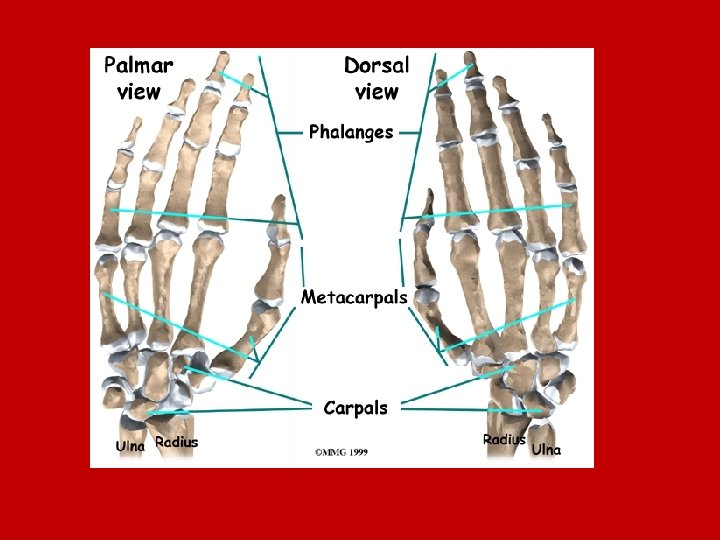
Bones are protective and supportive framework for the body. There are 206 bones of the human body The skeletal system consists of bones, cartilage, and the membranes that line the bones. Types of Bones • There axial and appendicular bones. (arms and legs) • There are 33 bones in the spine. These include: • 7 cervix (neck); • 12 thorax; • 5 lumbar; • 5 sacral; • 4 coccyx.
 consists of 12 pairs of ribs: • 7 pairs ‘true’ ribs")
The thorax (chest) consists of 12 pairs of ribs: • 7 pairs ‘true’ ribs (joined directly to the sternum (”breast-bone”)); • 3 pairs ‘false’ ribs (joined to the sternum (”breast-bone”) by cartilage); • 2 pairs ‘floating’ ribs (not connected to the sternum (”breast-bone”) at all, connected to the diaphragm. ;

Joints ØJoints are where bones come together & are complex structures made up of many parts. ØFunction of Joints ; hold the bones together and allow for movement of the skeleton. All of the bones form joints (except the hyoid bone in the neck).
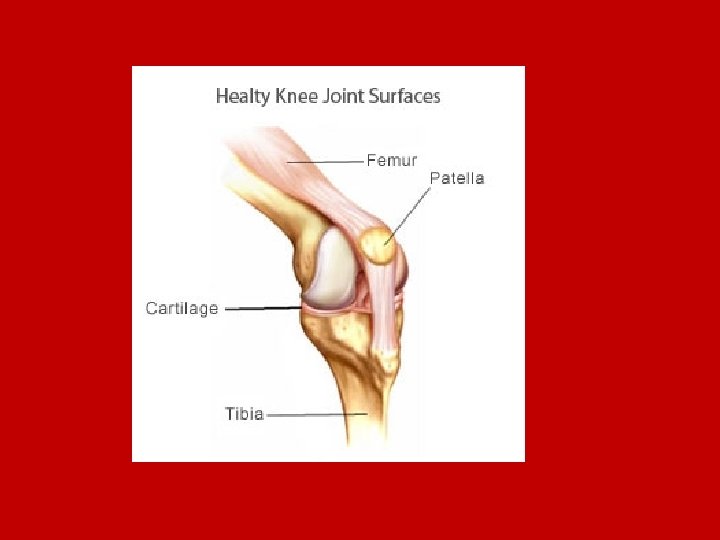

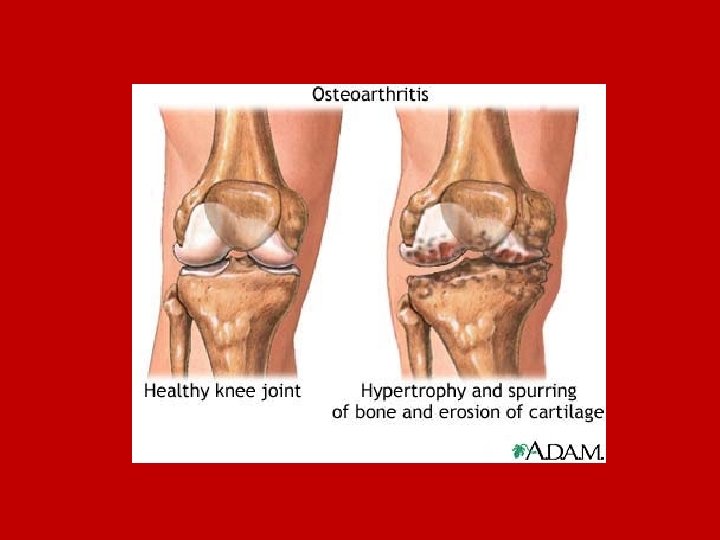
Limited ROM is a reduction in a joints normal range of movement, that may result from: • Mechanical problems • Swelling • Muscle spasticity • Joint pain • Inflammation (bursitis, tendonitis, etc. ) • Injury (sports injuries, fractures, dislocations) • Disease (many types of arthritis can lead to decreased range of motion)

Planes of Motion Movement is defined by referring to the three planes and the three axis

Sagittal Plane va vertical plane which passes through the body front to back, so dividing it into two symmetrical halves (left and right sides). v. Movements in this plane are the up and down movements of flexion and extension
 va vertical plane which passes from side to side dividing the")
Frontal Plane (coronal) va vertical plane which passes from side to side dividing the body into two halves (Anterior & Posterior). v. Movements in this plane are sideways movements, called abduction and adduction

Transverse Plane van horizontal plane which is parallel to the diaphragm dividing the body into two halves (superior & inferior). v. Movements in this plane are rotational in nature, such as internal and external rotation, pronation and supination
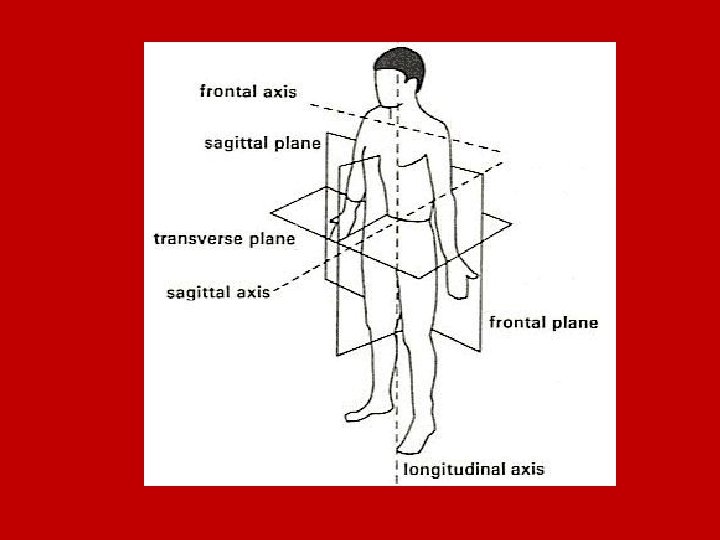

The Three Axis Frontal Axis - passes horizontally from side to side at right angles to the sagittal plane Sagittal Axis - passes from front to back at right angles to the frontal plane Longitudinal Axis - passes from head to foot at right angles to the transverse plane
 Angular motion is comprised of flexion, extension, adduction, and abduction.")
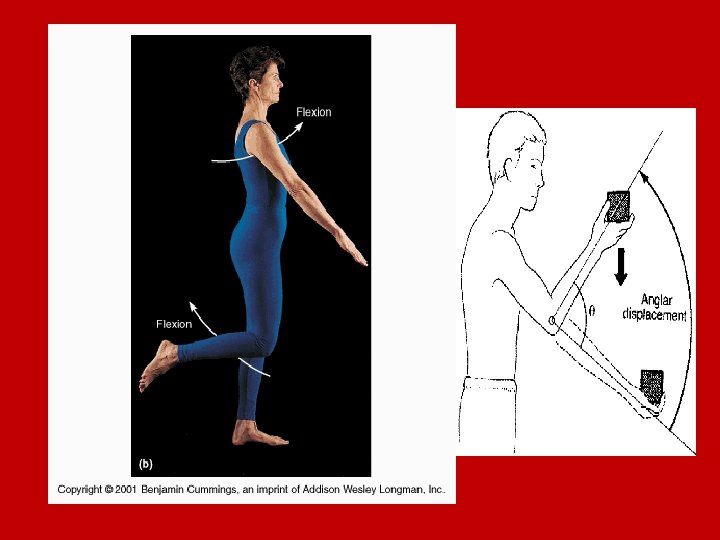
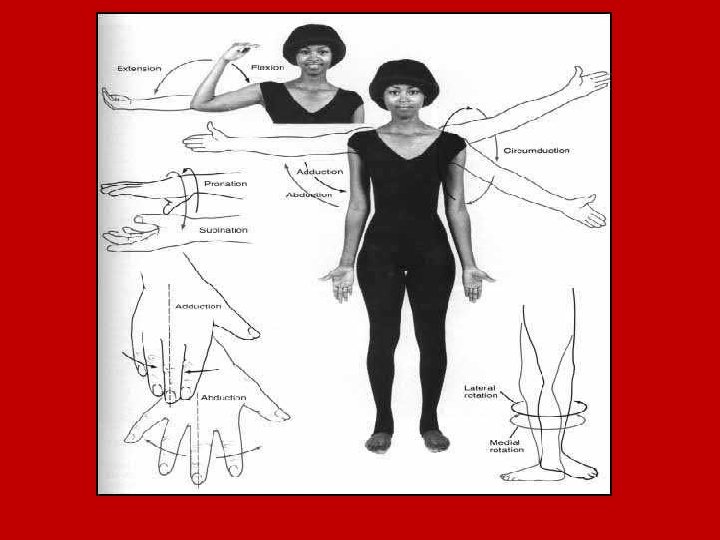
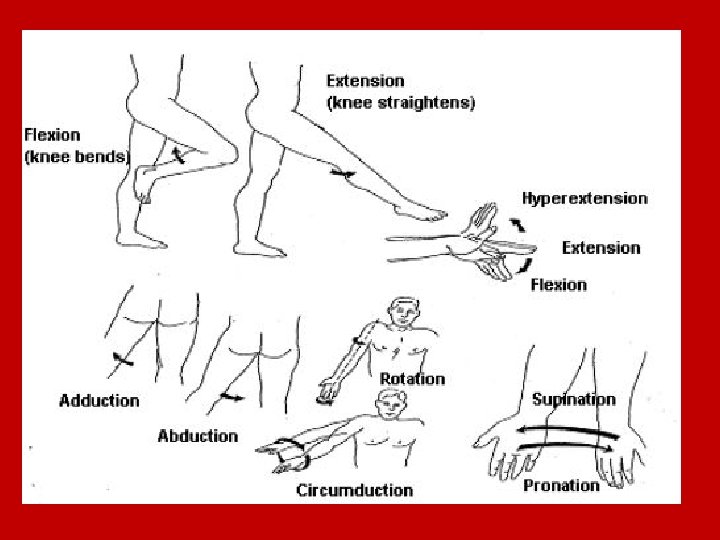
Types of Movement A) Angular motion is comprised of flexion, extension, adduction, and abduction. In angular movement Increase or decrease the angle between 2 bones.
 that reduces the angle between the")
ØFlexion is movement in the anteriorposterior plane (sagittal) that reduces the angle between the articulating elements. ØExtension occurs in the same plane as flexion but reverses the movement of flexion & increases the angle between articulating elements. Hyperextension is a continuation of movement past the anatomical position, which can cause injury.

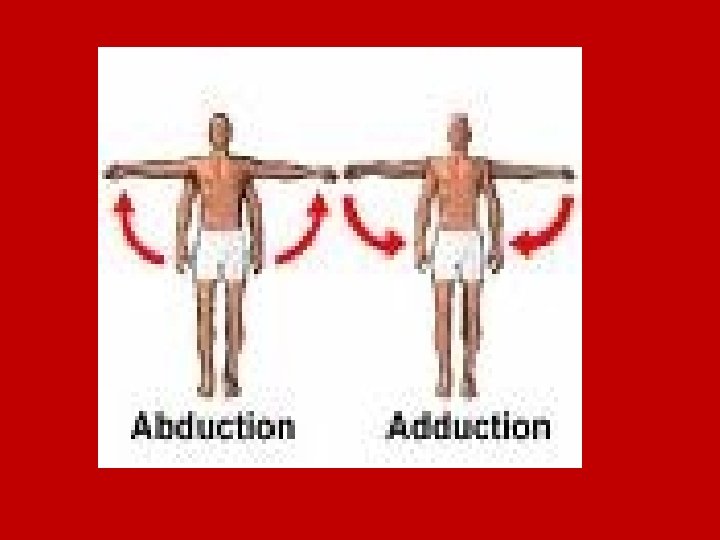
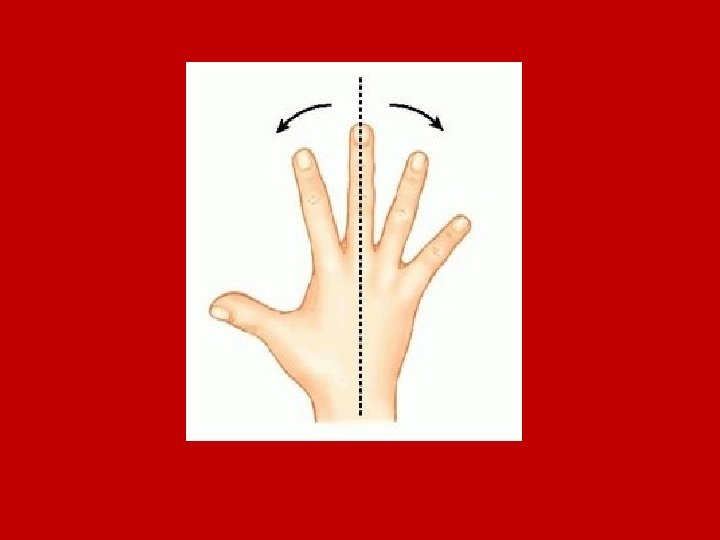
ØAbduction is movement away from the center, as spreading the toes or fingers apart. (coronal plane) ØAdduction is movement toward the midline of the body, as bringing the fingers and toes together. (coronal plane)
")
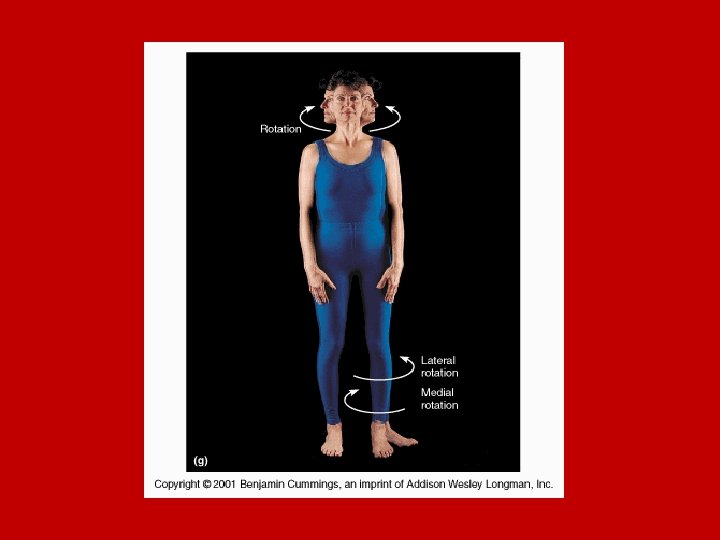
ØRotation involves turning the body or a limb around the longitudinal axis (transverse plane) as rotating the arm to screw in a light bulb.

ØCircumduction is a special type of angular motion, described as making circular movements as moving the arm in a circle or cone shape.

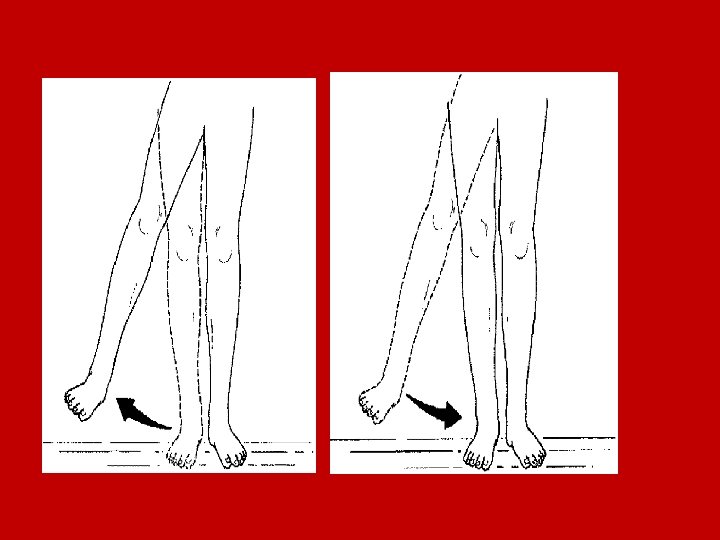
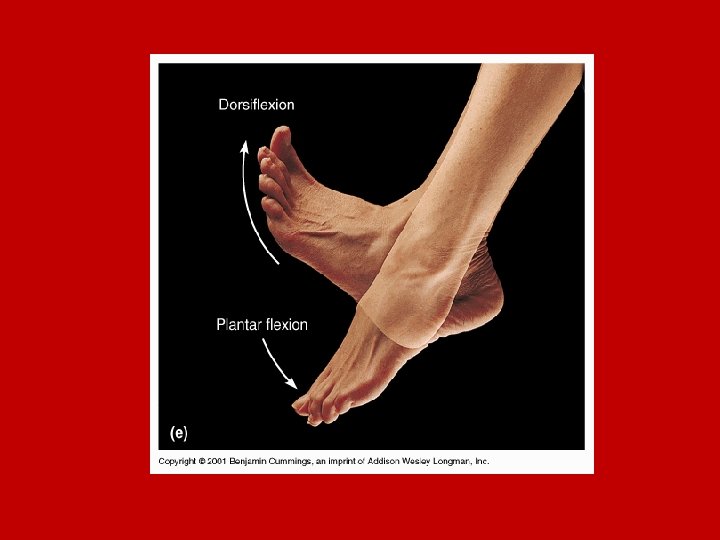
Dorsiflexion / Plantar flexion refers to movements of the foot. ØDorsiflexion is extension of the foot at the ankle i. e the movement of the ankle while elevating the sole, as if standing on heel. Ø Plantar flexion is flexion of the foot i. e elevating the heel, as if standing on tiptoes.

ØEversion - lateral or outward rotation of the foot. ØInversion - medial or inward rotation of the foot.

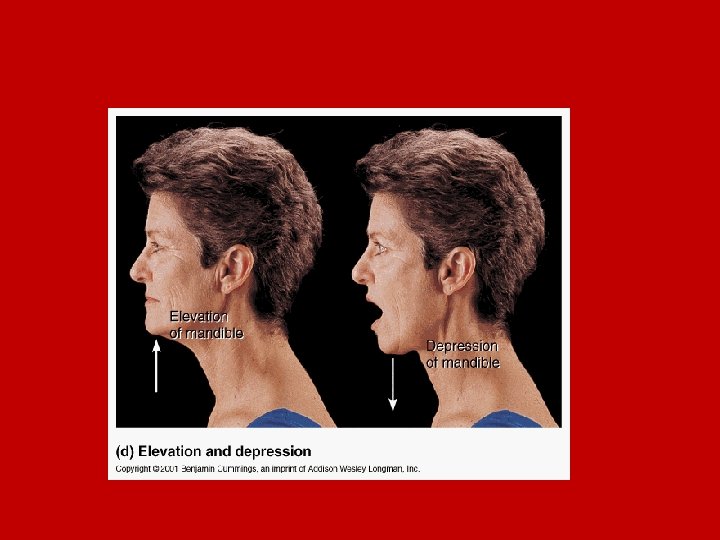
Ø Elevation / Depression occurs when a structure moves in a superior or inferior direction, as the mandible is depressed when the mouth is opened and elevated when the mouth is closed.

ØOpposition is a movement of the thumb in relation to other digits to enables it to grasp and hold an object.

ØPronation / Supination refers to the rotation of the distal end of the radius across the anterior surface of the ulna. This rotation moves the wrist and hand from palm-facing-front (supination) to palm-facing-back (pronation).

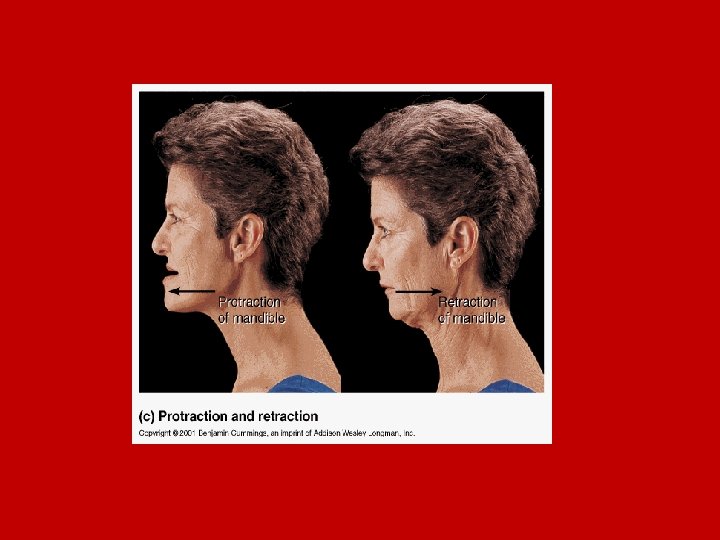
ØProtraction entails moving a part of the body anteriorly in the horizontal plane, as in jutting the face forward to gain distance at a finish line. Nonangular ØRetraction is the reverse movement of protraction as in pulling the jaw back towards the spine. Nonangular
 Gliding movement occurs when two opposing surfaces slide past each other; as between")
B) Gliding movement occurs when two opposing surfaces slide past each other; as between carpals, tarsals and the clavicle and sternum.

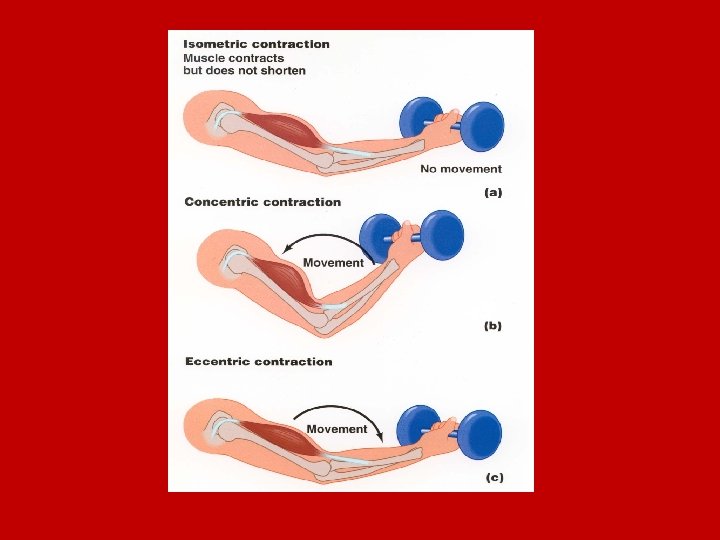
Forms of Muscle Contraction
 Isometric contraction means that muscles contract, but there is no motion in the")
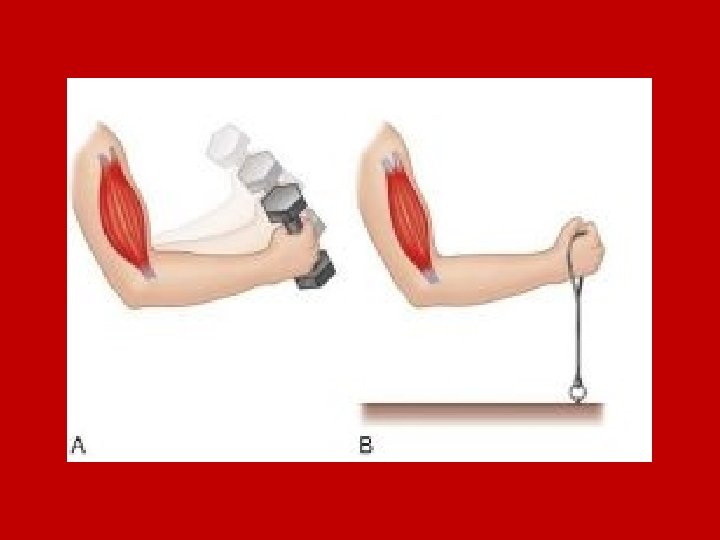
1) Isometric contraction means that muscles contract, but there is no motion in the joint. The muscle fibers maintain a constant length throughout the entire contraction. It is effective for developing total strength of a particular muscle or muscle group.
 Isotonic contraction (constant load) i. e contraction causes a joint to move. A")
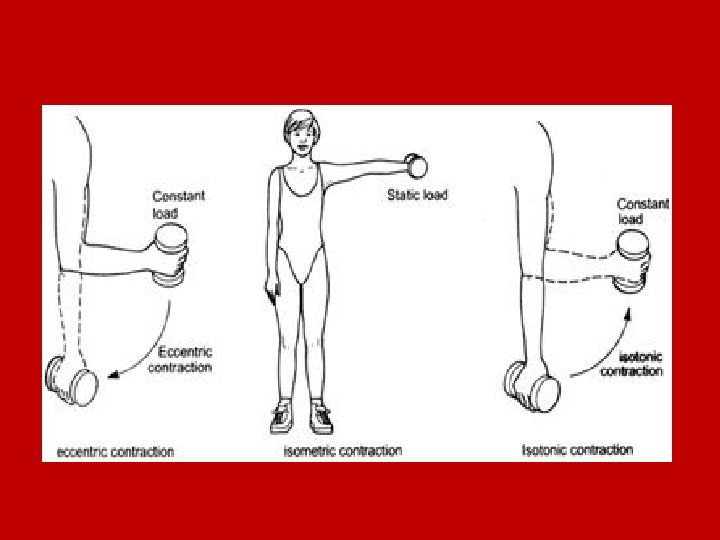
2) Isotonic contraction (constant load) i. e contraction causes a joint to move. A classic example of an isotonic exercise is weight training with dumbbells and barbells. concentric contraction eccentric contraction

Concentric Contraction Concentric muscle action means that the muscle is shortening. Eccentric Contraction Eccentric muscle action means that the muscle is lengthening
 Isokinetic contraction (constant speed) the speed is constant no matter how much effort")
3) Isokinetic contraction (constant speed) the speed is constant no matter how much effort is exerted. Such exercises are used to test and improve muscular strength and endurance, and are most commonly utilized by professional athletes. This type of exercise requires rather expensive equipment

v v v Summary of Muscle Contraction isometric- same length; static contraction i. e no ROM isotonic - same tension throughout ROM. dynamic contraction i. e ROM concentric- ms shorten (force of contraction > resistance) positive work. eccentric- ms lengthening (force of contraction < resistance); negative work tends to result in greater muscle soreness isokinetic - same angular velocity

Cooperating Muscle Groups When muscles cause a limb to move through the joint's range of motion, they usually act in the following cooperating groups:

Agonists; referred to as prime movers since they are the muscles that are primarily responsible for generating the movement. Antagonists; these muscles act in opposition to the movement generated by the agonists and are responsible for returning a limb to its initial position.

Synergists; These muscles perform, or assist in performing, the same set of joint motion as the agonists. Synergists are sometimes referred to as neutralizers because they help cancel out, or neutralize, extra motion from the agonists to make sure that the force generated works within the desired plane of motion.

Fixators; These muscles provide the necessary support to assist in holding the rest of the body in place while the movement occurs. Fixators are also sometimes called stabilizers.

As an example, when you flex your knee, the hamstring contracts, and, to some extent, so does the gastrocnemius (calf) and lower buttocks. Meanwhile, the quadriceps are inhibited (relaxed and lengthened somewhat) so as not to resist the flexion. In this example, • the agonist(prime mover) is hamstring. • the antagonist is quadriceps • synergists is calf and lower buttocks

Agonists and antagonists are usually located on opposite sides of the affected joint (like your hamstrings and quadriceps, or your triceps and biceps) synergists are usually located on the same side of the joint near the agonists. Larger muscles often call upon their smaller neighbors to function as synergists

The following is a list of commonly used agonist/antagonist muscle pairs: 1. Pectorals/latissimus dorsi ms. 2. Anterior deltoids/posterior deltoids (front and back shoulder) 3. Trapezius/deltoids. 4. Abdominals/spinal erectors. 5. Left and right external obliques (sides) 6. Quadriceps/hamstrings. 7. Biceps/triceps 8. Forearm flexors/extensors

Deltoids vs. Latissimus dorsi

Pectorals vs. Trapezius
: muscles responsible for a given")
Summary of Cooperating Muscle Groups v. Agonists (Prime Mover): muscles responsible for a given movement v. Anagonists: muscles act in opposition to the agonists v. Stabalizers: muscles that hold or fix a joint or part while the movers produce movement around it v. Neutralizer: muscles which contract to prevent unwanted actions
 in front of True statement and (F) in front")
Quiz put ( T ) in front of True statement and (F) in front of False statement 1. Recent injury is one of the indication of relaxed passive movement. 2. Complete evaluation must be done before the beginning of relaxed passive movement. 3. Relaxed passive movement is used to increase the restricted ROM to full rang.

4. Antagonist muscles act in opposition to the agonists. 5. Neutralizer muscles that hold or fix a joint or part while the movers produce movement around it. 6. when you flex your knee , quadriceps muscle is agonist muscles. Answer (F , T , F, T , F, F)



Factor Affecting Strength of Normal Muscles

1 - Type of Muscle Fiber Is one of the most influential factors. There are two basic types of muscle fibers: "slow twitch" and "fast twitch. " Slow twitch muscle fibers are best used for cardiovascular (aerobic) activities. They produce small levels of force for long periods of time and thus are better suited for endurance activities. Fast twitch fibers are best used for anaerobic activities. They produce high levels of force for short periods of time and are best suited for power activities such as weightlifting.

Most men and women have an equal combination of both slow twitch and fast twitch fibers. However, some people inherit a high percentage of slow twitch fibers that enhance their performance in endurance activities, such as long distance runners. Most world class marathon runners have a very high amount of slow twitch fibers. Conversely, world class sprinters have relatively fast twitch muscle fibers. Although both fiber types respond positively to strength training exercises, the fast twitch types experience greater increases in muscle size and strength, and thus may obtain greater and/or faster results from a strength training program.

2 - Age Another factor over which we have little control is age. Studies show that people of all ages can increase their muscle size and strength as a result of a safe and effective strength training program. However, the rate of strength and muscle gain appears to be greater from age 10 -20, the years of rapid growth and development. After reaching normal physical maturity, muscular improvements usually do not come as quickly.

3 - Gender does not affect the quality of our muscle, but does influence the quantity. Although men's and women's muscle tissue are characteristically the same, men generally have more muscle tissue than women do because muscle size is increased by the presence of testosterone, the male sex hormone. The larger the muscles, the stronger the person; this is why most men are stronger than most women.

4 - Limb and Muscle Length Another strength factor that is naturally determined is limb length. Persons with short limbs tend to be able to lift more weight because of advantageous leverage factors. Similarly, differences in strength development may come about because of variation in muscle length. Some people have long muscles, and some people have short muscles. Persons with relatively long muscles have greater potential for developing size and strength than persons with relatively short muscles.

5 - Point of Tendon Insertion Muscle strength is also influenced by the point of tendon insertion. For example, for two people with the same arm and muscle length, if one person's biceps tendon attaches to the forearm farther from the elbow joint than the other person's, that person will have a biomechanical advantage and be able to lift more weight than the other in biceps exercises such as the biceps curl.

6 - Other Important Factors The most influential factor in achieving good results is using a very slow, controlled lifting movement and lifting to the point of muscle fatigue. It is imperative that you not only train with intensity on a well-balanced program, but also give your muscles enough resting time between training sessions. Overtraining is a common mistake people make; it happens not only when you do not allow your muscles enough rest, but also when you train with too many sets for each muscle group.

Another mistake people make is doing the same program over and over again even after they have reached a plateau. Any time you stop gaining strength or muscle size or you get bored, it is crucial that you change the program, so that you can go through a whole new phase achieving new results.

Weightlifting provides many important benefits that cannot be achieved by any other exercise or activity. Physiologically, the benefits of consistent strength training include an increase in muscle size and tone, increased muscle strength, and increases in tendon, bone, and ligament strength. Strength-training also improves psychological health by increasing selfesteem, confidence, and self-worth. If you understand accept your body, you will be able to work with it, not against it. Everyone can improve their strength, appearance, and performance level by consistently implementing an effective strength training program.
- Slides: 75