Glucocorticoids Excessive thyroid hormone Diuretics Furosemide Cyclosporine Seizure







 � Cheese � Ice cream (1/2")





 is FDA approved for prevention and treatment of osteoporosis. � Alendronate �")





: Monoclonal antibody that against RANKL Approved for treatment of osteoporosis. 60")








- Slides: 33
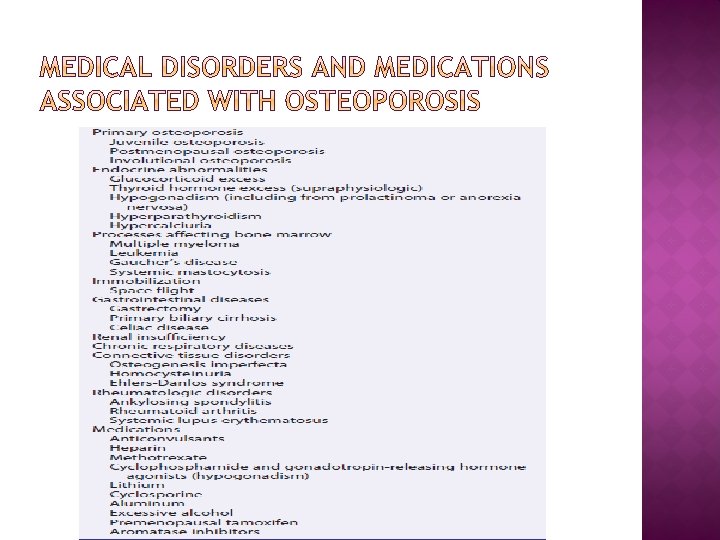
� Glucocorticoids � Excessive thyroid hormone � Diuretics: Furosemide � Cyclosporine, � Seizure medications: Phenytoin, phenobarbital � Psychotropic: � Heparin methotrexate, tacrolimus Lithium,
� Initial evaluation: CBC Ø Ca, p, Cr Ø Alkaline phosphatase, aminotransferases Ø 25 -hydroxyvitamin D Ø TSH Ø 24 -hour urine for Ca and creatinine Ø
� Osteoporosis diagnosed when a radiograph shows signs of demineralization or compression fractures of vertebral bodies. � Techniques for evaluating bone mass: � Dual-energy � Quantitative � Ultrasound x-ray absorptiometry (DEXA) (CT) of spine.
� All postmenopausal women < 65 yr who have one or more additional risk factors for osteoporosis � All women > 65 yr regardless of additional risk factors � To document reduced bone density in patients with vertebral abnormalities or osteopenia on radiographs � To diagnose low bone mass in glucocorticoid-treated individuals � To document low bone density in patients with asymptomatic primary or secondary hyperparathyroidism
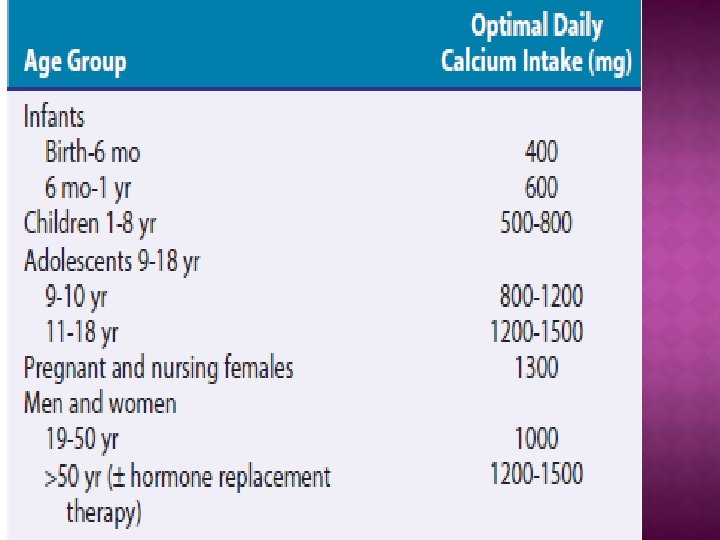
Calcium: � Goals of therapy for osteoporosis reduce bone resorption and enhance bone formation. � Bone loss occurs when Ca intake and absorption insufficient to balance daily Ca losses. � In absence of kidney stones or an underlying disorder of Ca metabolism, Ca intakes safe.
�Calcium carbonate: contains 40% elemental Ca should be taken with meals because of poor absorption in achlorhydric patients in absence of food.
�Calcium citrate: contains 24% elemental Ca, better bioavailability and is more absorbed well on an empty stomach in patients with achlorhydria.
Milk � Yogurt � Orange juice (with Ca) � Cheese � Ice cream (1/2 cup) � Soy milk (1 cup) � Beans (1/2 cup cooked) � Dark, green vegetables (1/2 cup cooked) � Almonds � Orange (1 medium) � � 300 mg � 250 mg � 300 mg � 195 to 335 mg � 100 mg � 300 mg � 60 to 80 mg � 50 to 135 mg � 70 mg � 60 mg
SELECTIVE ESTROGEN RECEPTOR MODULATORS �Tamoxifen: Ø Estrogen antagonist that binds to estrogen receptor Ø Estrogen-agonist effects on bone Ø Small increase in bone density of spine over 2 years, Ø No effect on radial bone density Ø 45% reduction at hip and 29% at spine fracture.
� Raloxifene: � FDA approved for prevention and treatment of osteoporosis � Estrogen agonist on bone � Antagonist effects on breast and uterus. � Increased BMD in lumbar spine by 2. 4%, in hip by 2. 4%, in total body 2% � Over 2 -year, significant reduction in vertebral fractures
�a potent inhibitor of osteoclastmediated bone resorption. � Human and salmon calcitonin available � Salmon calcitonin commonly used because greater potency. � Parenteral calcitonin (100 IU SC or IM three times a week or daily) � Maintain bone density or produce a small increase in bone mass in spine
� Nasal spray calcitonin absorbed through nasal mucosa � Approximately 40% as potent as parenterally administered (50 to 100 IU of injectable calcitonin comparable with 200 IU of nasal spray calcitonin). � Nasal calcitonin (200 IU/day) increases spinal bone density � No effect on proximal femur bone mass; � 36% reduction in vertebral fractures over 5 years.
� Adverse effects of parenteral calcitonin: nausea flushing local irritation at injection site � Calcitonin intranasally well tolerated � Rhinitis and nasal dryness and crusting potential side effects. � Calcitonin may beneficial analgesic response in presence of osteoporotic fractures.
�Alendronate (Fosamax) is FDA approved for prevention and treatment of osteoporosis. � Alendronate � (10 mg/day) produces: 8. 8% and 7. 8% increase in bone density in spine and femoral trochanter � Alendronate (70 mg) most commonly used dose for treatment of osteoporosis.
� Adverse � GI effects of bisphonates: symptoms: stomach pain esophagitis � Myalgias and arthralgias, � Osteonecrosis of jaw � Subtrochanteric fractures
�Risedronate: � Increased bone mass � Reduced risk of new vertebral fractures � Significant reduction in risk of hip fracture � Approved for prevention and treatment of osteoporosis(35 mg once a week) � Risedronate well tolerated even in patients with mild GI symptoms.
�Ibandronate: � Approved for treatment and prevention of osteoporosis. � Vertebral � 150 fractures reduce about 50%. mg/month � Intravenous ibandronate in a dose of 3 mg every 3 months
�Zoledronic acid approved for treatment and prevention of osteoporosis. � 5 mg once a year by intravenous infusion, � Risk of vertebral fractures reduce 68%, hip fractures 40%
� Side effects: arthralgias and myalagias; � Patients should have serum Ca and 25 -OHD levels monitored and replaced to NL levels before treatment.
� Denosumab (Prolia): Monoclonal antibody that against RANKL Approved for treatment of osteoporosis. 60 mg subcutaneously every 6 months for 36 months Vertebral fractures reduce 68%, hip fractures 40%, Well tolerated, Adverse events: skin infection Before treatment Ca and 25 -OHD should be checked and replaced if needed up to normal levels.
� PTH significantly increase bone mass in spine, � Fortéo � 20 approved for treatment of osteoporosis. μg/day for 21 months. � Lumbar spine bone mass increased between 9% and 13% , � Hip bone mass increased slightly.
� Risk of new vertebral fractures reduce nearly 70%. � Fortéo is given daily injection. � Individual may experience headache, nausea, flushing with initiation of treatment, but these side effects become less severe after few weeks.
�PTH: Ø Stimulates new bone formation Ø Increases bone mass Ø Reduces new vertebral and nonvertebral fractures
� Subcutaneous injection daily for 18 to 24 months. � Other routes of administration: intranasal skin patch.
� Physiologic doses of vitamin D important to NL bone mineralization. � Individuals 50 years of age and older should take at least 600 to 1000 IU of vitamin D daily � Low vit D levels increase risk of bone loss and fracture.
� Low 25 -OHD levels during the winter and spring associated with decreases in bone density. � Daily treatment with 700 IU of cholecalciferol and 500 mg of Ca carbonate reduced rate of bone loss in: femoral neck, spine, total body � Decreased incidence of nonvertebral fractures by 50%. � Patients require a vit D intake that in 25 -OHD level of at least 30 ng/m. L.
� Patients starting GC therapy at a dose equivalent to prednisone ≥ 5 mg/day for 3 mo or longer should: � Modify risk factors for osteoporosis (stop smoking, decrease alcohol consumption) � Start regular weight-bearing physical exercise � Initiate intake of Ca (total 1500 mg/day) and vit D(400 -800 I U/day) � BMD to predict risk of fracture and bone loss � Initiate bisphonate therapy (alendronate 5 mg/day or 35 mg/wk, or risedronate 5 mg/day or 35 mg/wk)
� If T-score is < − 1: � Risk factor modification including reducing risk of falls � Regular weight-bearing physical exercises � Ca and vit D supplementation � Bisphonate therapy (alendronate 10 mg/day or 70 mg/wk, or risedronate 5 mg/day or 35 mg/wk); � If bisphonates contraindicated or not tolerated, calcitonin as second-line agent, intravenous bisphonate (pamidronate or zolendronate), parathyroid hormone � Repeat BMD measurement annually or biannually