Global T inversion Elias Hanna MD LSU Cardiology

Global T inversion Elias Hanna, MD LSU Cardiology
 in most")
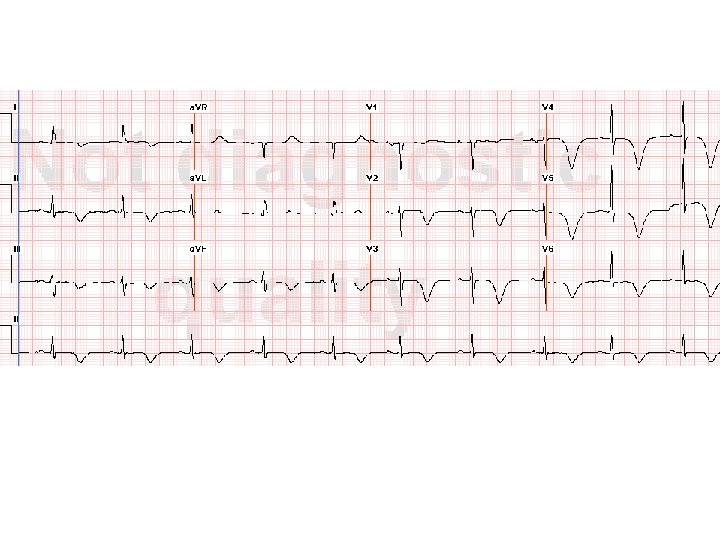
• Normal sinus rhythm • Global T wave inversion (>10 mm) in most leads with prolonged QTc (~560 msec)
 T-wave inversion? • T wave is inverted in most of")
What is Global (Diffuse) T-wave inversion? • T wave is inverted in most of the standard leads except a. VR, which shows a reciprocal upright T wave. • The QT interval is often prolonged, and T-wave inversion is often symmetric and “giant” (> 10 mm, i. e, > 2 big boxes). • This is different from Wellens T waves, wherein the T abnormality is limited to the anterior leads (esp V 2 -V 4) and ST segment is slightly upsloping

Causes of Global T-wave inversion Most common 1 -Myocardial ischemia 2 -Intracranial hemorrhage or any intracranial process 3 -Hypertrophic cardiomyopathy 4 -High catecholamine states: cocaine use, pheochromocytoma, Takotsubo (stress-induced) cardiomyopathy 5 -Other: peri/myocarditis, high-grade AV block, PE

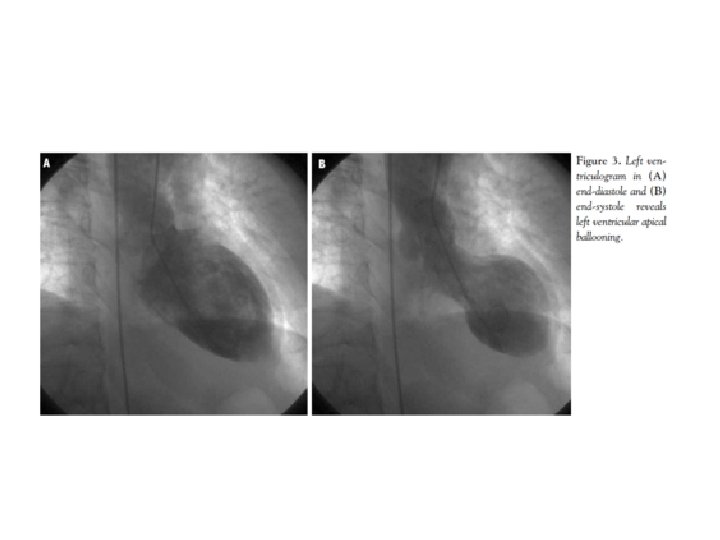
• Coronary angiography shows non-obstructive CAD • Echocardiogram and Lvgram show apical dyskinesis with preserved basal contractility and EF ~20% • Acute non-ischemic HF Low EF with apical dyskinesis Mild troponin increase Takotsubo Cardiomyopathy Deep T inversion No CAD

• Takotsubo cardiomyopathy OR: • Stress-mediated cardiomyopathy • Apical ballooning syndrome • Broken heart syndrome

• 95% of Takotsubo cases are seen in Females>55 yo. It is very uncommon in men or <50 yo • Usually presents as CP with mild increase in troponin and ST-elevation in the anterior leads, mimicking STEMI • ST elevation is followed by deep T inversion with prolonged QT. If diagnosed at this stage, Takotsubo mimicks NSTEMI • HF presentation is less common (17%)

• Functional MR is seen in 20% of cases, related to tethering of the mitral valve • Very good prognosis with a low risk of early death or compplications (VT, stroke, cardiogenic shock) • ~1% risk of death • LV dysfunction always resolve within 2 months, usually 1 -2 weeks • Recurrence 11% over 4 yrs
- Slides: 11