GIST cology Oncology Oncology F ALMashat Dep of

 with specific histological")







")









:")
")














- Slides: 37
GIST cology @@@@@ Oncology @@@@@ Oncology @@@@ F. AL-Mashat Dep of surgery Kauh & Kahoc
Definition cology @@@@@ Oncology @@@@@ Oncology @@@@ c-Kit–positive mesenchymal tumours (MT) with specific histological & IHC characteristics occuring in GIT
History cology @@@@@ Oncology @@@@@ Oncology @@@@ ① 20 y most MT of gut were considered to be of smooth muscle or perineural origin ② Mazur & Clark (1983): GIST ③ Kindblom(1998): Interstitial cell of Cajal GIPACT ④ Today, most gut MT previously designated leiomyomas, leiomyoblastomas & leiomyosarcomas are GIST ⑤ True gut leiomyomas & schwannomas remain to be identified
Epidemiology cology @@@@@ Oncology @@@@@ Oncology @@@@ ■ The most common MT of gut ■ 0. 1 - 3% of gut cancers ■ Incidence: 20/10 people/year ■♂=♀ ■ Predominantly 5 - 7 decades. Rare < 40 y ■ Spectrum: Benign - highly Malignant ■ Majority Benign. 10 – 30 % Malignant ■ Currently many clinicians and pathologists believe that all GISTs have at least some malignant potential
Manifestations cology @@@@@ Oncology @@@@@ Oncology @@@@ ■ Difficult early diagnosis, often asymptomatic ■ Small: asymptomatic and discovered incidentally (1/3) ■ Many: “silent” until they grow large enough to bleed or rupture ■ Stomach (60% - 70%) and small intestine (20% 30%) ■ Other sites : oesophagus, omentum, mesentery, colon, and rectum ■ 30% malignant: metastatic or infiltrating ■ Met: usually to liver. Peritonium infrequent. Nodes & extra-abdominal rare ■ Symptoms: location , size & growth pattern ■ Most common: palpable abdominal mass( 50% to 70%) , may be associated with vague G I pain and discomfort. ■ The second: G I haemorrhage (one third). ■ Less common, non-specific: anorexia, weight loss, nausea, bowel obstruction , obstructive jaundice , ■ 10 % present with met
Diagnosis cology @@@@@ Oncology @@@@@ Oncology @@@@ ① CT: Standard. Extraluminal mass + central necrosis ② MRI ③ Barium & Endoscopy ④ Biopsy/ FNA: Peritoneal seeding. Only unresectable ⑤ 18 FDG-PET: Follow-up ⑥ Surgery: well defined extraluminal mass, frequently lobulated
Schematic structure of the c-Kit tyrosine kinase cology @@@@@ • . Oncology @@@@@ Oncology @@@@@ Oncology @@@@ The extracellular domain of the c-Kit receptor binds to the ligand SCF. Tyrosine protein, which is where Glivec binds to c-Kit kinase activity resides in the intracellular domain of the
c-Kit signal transduction cology @@@@@ Oncology @@@@@ Oncology @@@@ Binding of the ligand SCF to the c-Kit tyrosine kinase receptor causes the receptor to dimerise, auto-phosphorylate, and become activated. Recruitment of other signalling proteins into a signalling complex then initiates a signal transduction cascade with some final steps occurring in the nucleus.
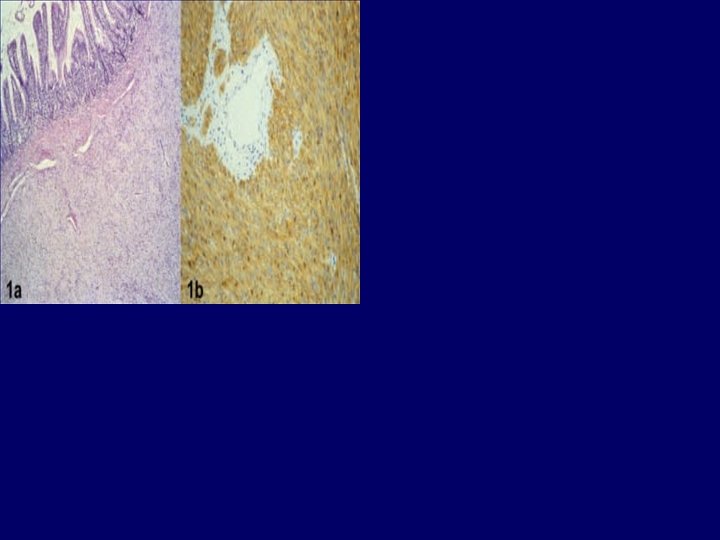
Pathology cology @@@@@ Oncology @@@@@ Oncology @@@@ ① Cells may resemble mesenchymal, neural, & smooth muscle ② Spindle cell (70%) , less commonlly Epithelioid or Mixed cell phenotype ① 1 cm to > 40 cm ② extraluminal with frequent mucosal ulceration ③ well circumscribed & pseudo-encapsulation ④ frequent necrosis, cystic degeneration & focal haem
Immunohistochemistry cology @@@@@ Oncology @@@@@ Oncology @@@@ ■ +ve c-Kit (90 – 100 %) ■ recommended: c-Kit be performed on all intraabdominal sarcoma-like tumours ■ performed on fixed paraffin or frozen ■ CD 34: 70% - 80%. expressed in many tumours, so modestly specific ■ Actin (30 %) & Keratin (<10 %) ■ Desmin & S-100: -ve ■ Vimentin: +ve ■ Ki 67: may aid in prognosis and monitoring
cology @@@@@ Oncology @@@@@ Oncology @@@@ Histological & I H C ( KIT, CD 34) are the defining features of GIST
Treatment cology @@@@@ Oncology @@@@@ Oncology @@@@ • • Until now limited treatment options, such as radiation and surgery, which have shown only limited success. • The recent introduction of Glivec (imatinib) molecularly targeted therapy for treatment of patients with unresectable or metastatic GISTs has led to significantly better outcomes and helped spur renewed interest in reliable and accurate diagnosis of this difficult malignancy. Glivec specifically targets the surface tyrosine kinase receptor c-Kit (CD 117), which is now recognised as the hallmark immunohistochemical cell marker of GIST. • Before Glivec • The majority of GISTs (~95%) are highly resistant to radiation and systemic therapy, and, until now, surgery has been the only effective treatment option. Unfortunately, many GISTs are unresectable, and metastatic GISTs are essentially incurable, with a median survival of 10 to 21 months, and for these tumours, palliative surgery or chemotherapy has been the only therapeutic option
Prognostic factors cology @@@@@ Oncology @@@@@ Oncology @@@@ ■ Display gifferent degrees of aggressiveness ■ Biological behaviour prediction: conflicting reports ■ Criteria: ① Siz: <5 cm ② Mitosis: >5/hpf ③ Necrosis ④ Mi. B 1: >10% ⑤ Invasive character ⑥ Symptoms ⑦ Histology ⑧ IHC ⑨ Met ⑩ Node invasion
cology @@@@@ Oncology @@@@@ Oncology @@@@ The two most easily applicable criteria for predicting recurrence: Size and Mitosis
Fletcher et al 2002 cology @@@@@ Oncology @@@@@ Oncology @@@@ ① Very low risk: <2 cm <5/50 HPF ② Low risk Excellent : 2– 5 cm <5/50 HPF ③ Intermediate: <5 cm 6– 10/50 HPF 5– 10 cm <5/50 HPF ④ High risk : >5 cm >5/50 HPF >10 cm any mitotic rate any size >10/50 HPF Recurrence
Bucher et al 2004 cology @@@@@ Oncology @@@@@ Oncology @@@@ Minor criteria ① Size ≥ 5 cm ② Mitosis ≥ 5 /50 hpf ③ Necrosis ④ Infiltration of adjacent structures (i. e. mucosa or serosa) ⑤ Mi. B 1 index ≥ 10% Major criteria ① Node invasion ② Met Low malignant potential (LMP): 5 -y - 95% < 4 minor criteria High malignant potential (HMP): 5 -y - <20% 4 or 5 minor or 1 major
cology @@@@@ Oncology @@@@@ Oncology @@@@ Both scales need to be Validated in large prospective GIST trials
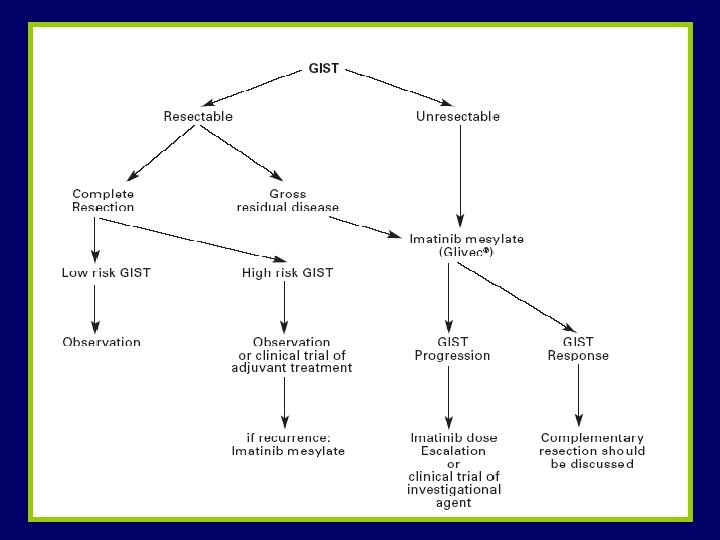
Treatment cology @@@@@ Oncology @@@@@ Oncology @@@@ Surgical resection: Choice ■ Resectability rate (RR): 50 – 90 % ? ? Non specialised centres: high RR Specialised centres: advanced ■ Completeness of resection correlates with survival
Extent of resection cology @@@@@ Oncology @@@@@ Oncology @@@@ ① En bloc (R 0) ② ≤ 2 cm: Wedge(gastric) or Segmental(bowel) ③ Large: extensive en bloc including adjacent structures / organs ④ Incomplete: Palliative. Risk of bleeding
Synchronous liver met cology @@@@@ Oncology @@@@@ Oncology @@@@ ■ Resection advocated when applicable, since a complete & long term response to Glivec not demonstrated ■ Non-resectable: complementary resection should be done after response to Glivec
Lymph node dissection cology @@@@@ Oncology @@@@@ Oncology @@@@ GIST, even with high malignant potential, metastasise to lymph nodes Infrequently to warrant node dissection
cology @@@@@ Oncology @@@@@ Oncology @@@@ There is no indication for Chemo & Radio after resection because: Unresponsive
Molecular targeted therapy cology @@@@@ Oncology @@@@@ Oncology @@@@ ■ Several protein kinases are overexpressed due to gene mutations ■ Targeted for selective pharmacological inhibitors Breakthrough Imatinib mesylate (Glivec)
cology @@@@@ Oncology @@@@@ Oncology @@@@ ■ Glivec: powerful & selective inhibitor of all ABL tyrosine kinases: c-kit, c-ABL, bcr-ABL & PDGFRA ■ Efficacy assessed in CML ■ Mechanism: A- Inhibits KIT & PDGFRA by reversible binding (vast majority of KIT mutants & wild KIT are sensitive) B- Inhibits ligand-stimulated native PDGFRA & PDGFRA mutant
Prognosis cology @@@@@ Oncology @@@@@ Oncology @@@@ ■ Overall 5 y surv: 48 - 80 % LMP: 95% HMP: 0 – 30 % ■ No long-term surv data available for malignant GIST in Glivec era ■ Major improvement: 1 y 90% vs < 50% before Glivec
cology @@@@@ Oncology @@@@@ Oncology @@@@ ■ Recurrence: LMP: extremly rare HMP: > 80 % ■ Follow - up: ☊ LMP: yearly ☊ HMP: closer. 50% recur during 1 year ☊ PET: The most reliable ☊ CT: Valuable for recur
cology @@@@@ Oncology @@@@@ Oncology @@@@