Giardia lamblia Intestinal flagellate Giardia lambilia lives in
 Intestinal flagellate Giardia lambilia lives in small intestine Giardiasis Diarrhea “traveler’s")
Giardia lamblia (蓝氏贾第鞭毛虫) Intestinal flagellate Giardia lambilia lives in small intestine Giardiasis Diarrhea “traveler’s diarrhea”

1. Morphology Nucleus 核 Sucking disk 吸盘 Inverse Pear-shaped 9 21× 5 25μm Flagellum (two anterior, posterior, ventral and tail flagella) 鞭毛 Median body 中体 Axostyle 轴柱 Trophozoite

Front side flagella Behind side flagella ventral flagella Ventral surface Tail flagella Lateral surface



Cyst: ball-shaped or oval , thick wall , 2 -4 nuclei, 10 14µm × 7. 5 9µm Nucleus Axostyles Flagella

Cyst in stool (Stained with haematoxylin

2. Life Cycle Mature cyst Passed in feces Contaminated food and water By mouth Ingested by man or animals Excystation in duodenum 2 trophzoites Cyst Attaching to duodenum, upper small intestine, multiply by binary fission

2. Life Cycle

characteristics of life cycle Infective stage: Mature cyst Mode of infection : Mouth, Fecal-Oral transmission (hand to mouth) Colonizing sites: duodenum, upper small intestine
 Pathogenic mechanism (not clear) 1) Different virulence: • mechanical blockage")
3. Pathogenesis (1) Pathogenic mechanism (not clear) 1) Different virulence: • mechanical blockage of the intestinal mucosa • lesion of the intestinal mucosa by suckers of G. l • toxicity to the intestinal mucosa by the secretion and excretion of G. l Malabsorption (of fat and carbohydrate)
 Physiological / immunity status • e. g. Intestinal Ig. A deficiency ,susceptible")
2) Physiological / immunity status • e. g. Intestinal Ig. A deficiency ,susceptible to the infection (2) Pathologic changes There are shortening of microvilli (微绒毛), epithelial cell damage, and low-grade inflammation of the duodenal mucosa
 Clinical Manifestation Incubation period: 1~2 w(45 d) 1)Acute giardiasis onset of diarrhea")
(3) Clinical Manifestation Incubation period: 1~2 w(45 d) 1)Acute giardiasis onset of diarrhea (Water--like stools ) stools suddenly with terrible odour abdominal cramping, bloating (胃胀气), abundant flatus, nausea (恶心) and vomiting, low-grade fever, usually last 1 to 3 weeks • In young children, it may persist for months characterized by fatty and greasy stool, significant malnutrition and weight loss.
Chronic phase: Intermittent bouts of mushy stools with foul smelling, abdominal pain, nausea, weight")
2)Chronic phase: Intermittent bouts of mushy stools with foul smelling, abdominal pain, nausea, weight loss, may persist for a long period (years). In children, it may result in undergrown.
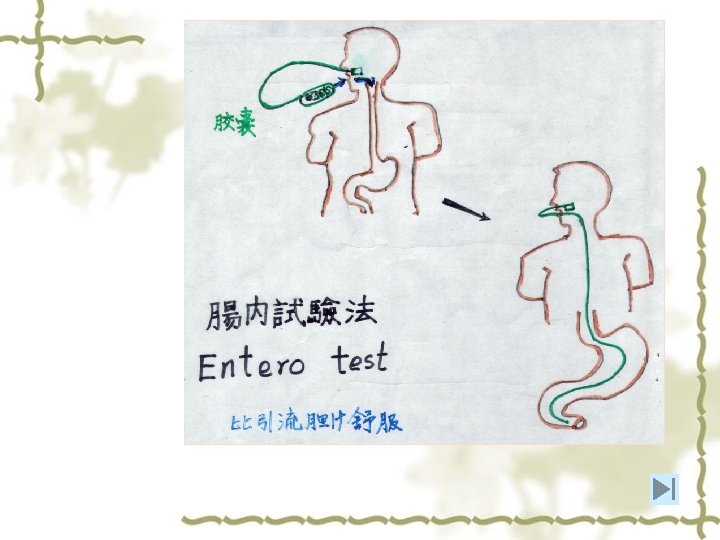
Parasitic Diagnosis 1)Stool examination:as same as in E. h 2)Duodenal fluid")
4. Diagnosis (1)Parasitic Diagnosis 1)Stool examination:as same as in E. h 2)Duodenal fluid or bile examination: ①Duodenal aspiration(十二指肠引流) ② Duodenal capsule technique (肠检胶囊法) (2)Immunologic test:mainly Ab detection (3)Molecular method: DNA probe、 PCR
Distribution: World wide The infection rate is 1~20%. • Higher in")
6. Epidemiology (1)Distribution: World wide The infection rate is 1~20%. • Higher in areas of poor sanitation (rural higher than urban area) and in day care settings • There were several outbreaks in European and American countries. • Estimated incidence in China of 2 -10%

Transmission 1)The source of infection: The hosts who can pass the cyst: patient and")
(2)Transmission 1)The source of infection: The hosts who can pass the cyst: patient and carrier, animals (cat, dog, cattle, sheep, pig, beaver, etc. ) large number of cysts shed (some patients shed up to 900 x 106 per day) 2)The route of infection: Contaminated water and food, Spread by insects By mouth The cysts are resistant to adverse environmental conditions : üCan remain infective in water for 2 -4 days (up to 16 d, including in tap water) and in the digestive tract of cockroach for 12 d. üBut susceptible to high temperature and dryness
Susceptible • All populations are susceptible to populations: • But higher frequency of infection")
3)Susceptible • All populations are susceptible to populations: • But higher frequency of infection in < 5 year and 25 -39 year age groups, and travelers, and immunodeficiency persons So called: “hikers disease”, “traveler’s diarrhea” Transmission is also found in homosexual males ( STD )
 Chemotherapy: Metronidazole, tinidazole (2) Block of routes of")
6. Prevention and Treatment (1) Chemotherapy: Metronidazole, tinidazole (2) Block of routes of transmission Adequate disposal of human stools Safe and adequate water supply ( filtration, boiling) Control of flies and cockroaches (3) Protection of susceptible population Public health education Good personal hygiene
- Slides: 22