Giardia lamblia AKA Giardia intestinalis or Giardia duodenalis
")
Giardia lamblia (AKA Giardia intestinalis or Giardia duodenalis)
 and bile ducts")
• cosmopolitan, monoxenous human parasite, which inhabits small intestine (duodenum) and bile ducts • trophozoites attach to surface of the epithelial cells with special „adhesive disc” and they cause some pathological changes of intestinal mucous membrane

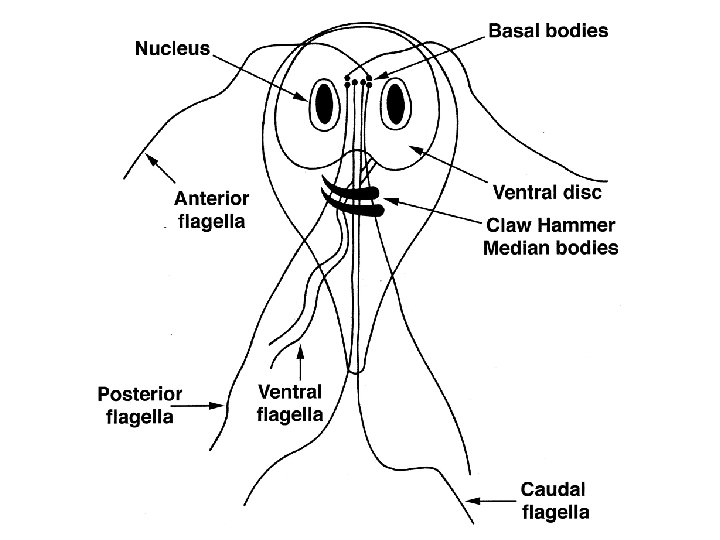
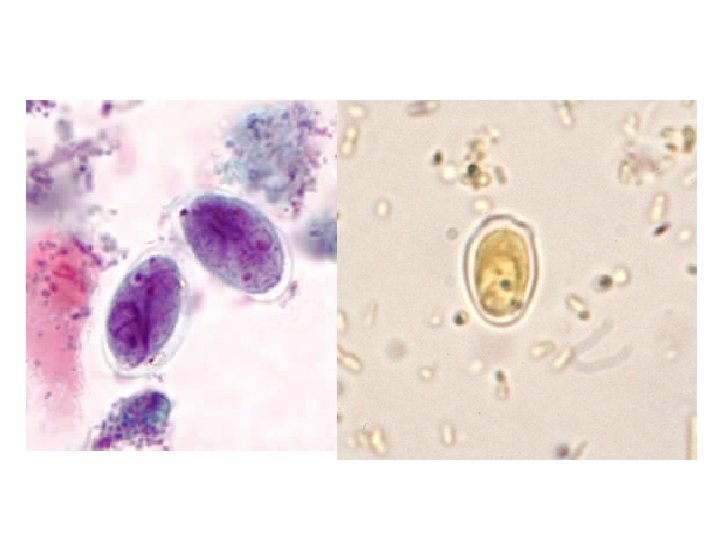
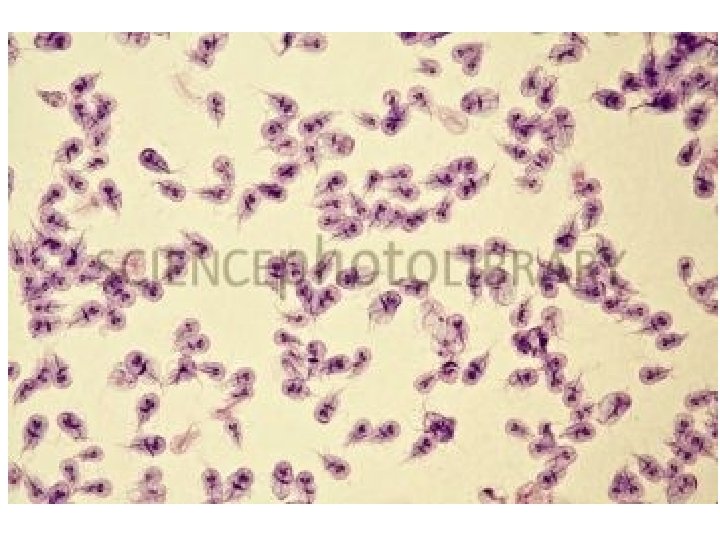
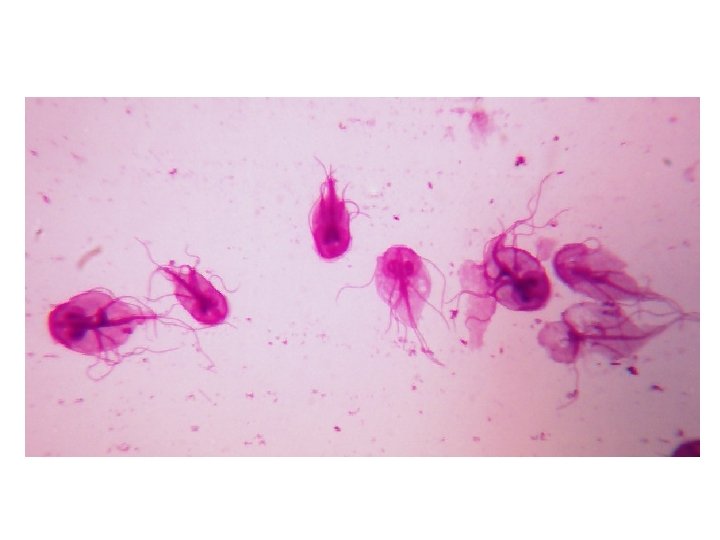
MORPHOLOGY • it forms bi-nucleate trophozoite and cyst • trophozoite: oval or pear-shaped, 12 -15 µm long, 5 -15 µm wide • cyst: ovoid, 8 -12 µm by 7 -10 µm in size
 disc • Nu – two nuclei •")
• AD – ventral adhesive (sucking) disc • Nu – two nuclei • k – kariosome • Ax – two axonemes (serves as the "skeleton”) • Fg – four pairs of flagella • MB – two large median bodies (unique to the species of Giardia)

FOUR PAIRS OF FLAGELLA in trophozoite
 •")
• CW – cyst wall (with cytoplasm retracted away form the CW) • Nu – nuclei (two in young cysts, four when matured) • k - kariosome • Ax - axoneme • MB – median bodies (4 in fully mature cysts)


EPIDEMIOLOGY • most common in the warm climate • the prevalence may be up to 25% in various population groups in some temperate areas • it infects nearly 2% of adults and 6% to 8% of children in developed countries worldwide, while nearly 33% of people in developing countries have had giardiasis

• children are more susceptible than adults! • several animals may serve as reservoir host of this parasite • domestic animals may transmit dieases directly to humans, however the type of Giardia that infects humans is usually not the same type that infects dogs and cats • it is found mostly in different water sources: lakes, streams
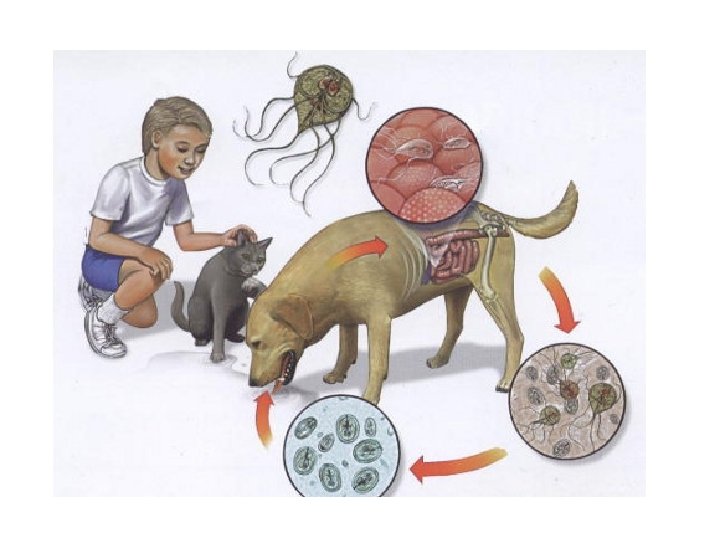

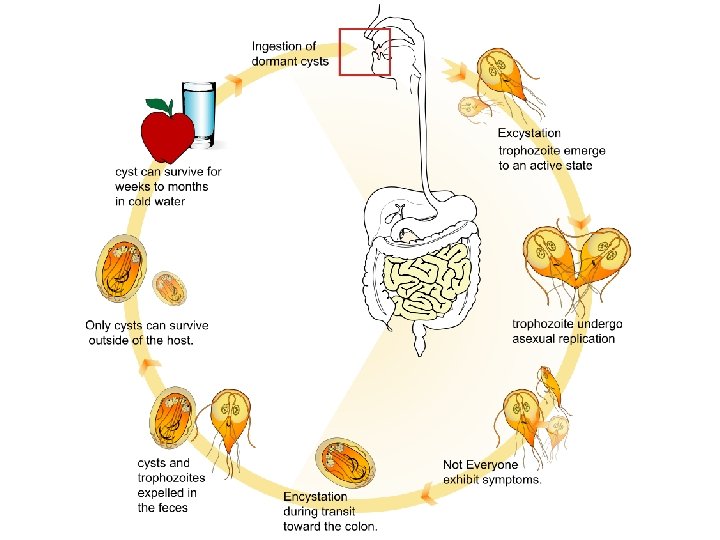
• the infective stage for humans is CYST • cysts are passed in the feces and, in contrary to trophozoites, they can remain viable for months in extrenal environment (like water) • an infected person might shed 1 -10 billion (usually 300 milions) cysts daily in the feces and this might last for several months • HOWEVER, swallowing as few as 10 cysts might cause someone to become ill
 and water contaminated with cysts")
• SOURCES OF INFECTION ARE MAINLY: food (vegetables) and water contaminated with cysts – indirect transmission • Giardia may be passed person-to-person or even animal-to-person (very rarely!) direct transmission by hand to mouth (oral route) • symptoms of giardiasis normally begin 1 to 3 weeks after a person has been infected

LIFE CYCLE

DISEASE • is called giardiasis/ giardiosis • signs and symptoms may vary and can last for 1 to 2 weeks or longer • in most cases it is asymptomatic giardiasis is the most frequently diagnosed intestinal parasitic disease in the US and among travelers with chronic diarrhea

Acute symptoms include: • diarrhea and gas • light colored, greasy stools • stomach or abdominal cramps and pains • dehydration (loss of fluids) • upset stomach or nausea/vomiting • loss of weight (failure to absorb fat, lactose, vitamin A and B 12)

• other, less common symptoms include: itchy skin, swelling of the eye and joints, and nervous complaints • in children, severe giardiasis might delay physical and mental growth, slow development, and cause malnutrition (anaemia) • sometimes, the symptoms of giardiasis might seem to resolve, only to come back again after several days or weeks

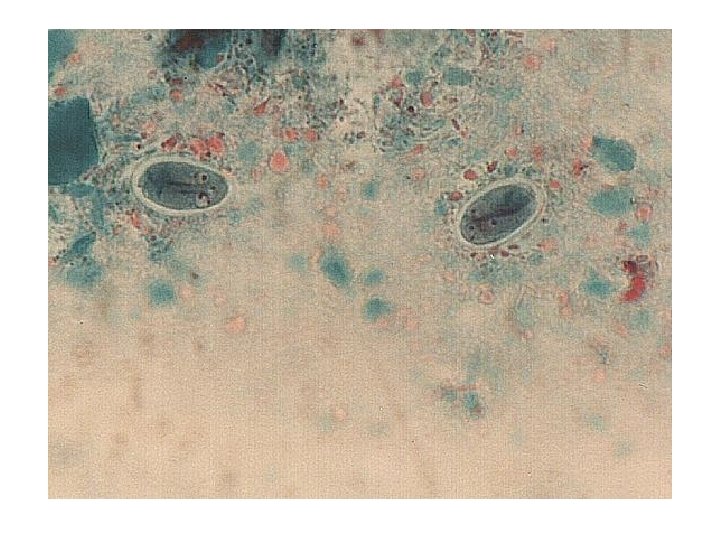
DIAGNOSIS direct microscopic identification of: • cysts in stool (smear of feces, permanent stained fecal smears, by means of concentration techniques) • trophozoites in loose stool • trophozoites in the duodenal contents (with Enterotest capsule)

ENTEROTEST

cysts of G. lamblia in stained stool specimen

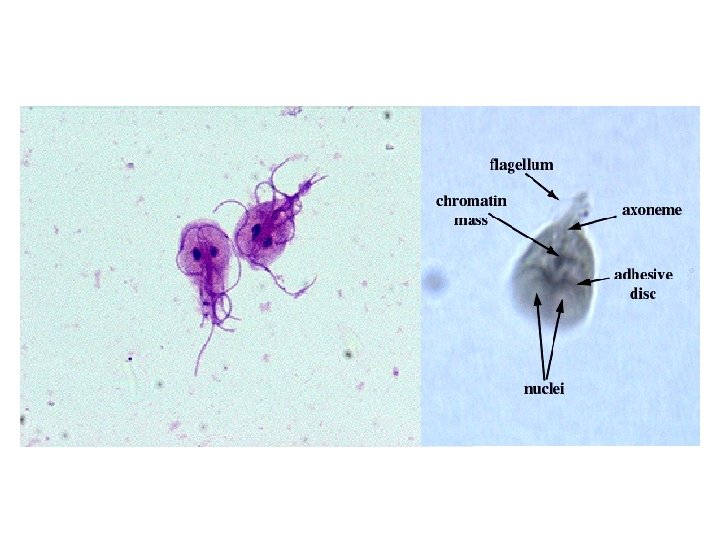
trophoziotes of G. lamblia

TREATMENT • several drugs can be used to treat Giardia infection • effective treatments include metronidazole and tinidazole • alternatives to these medications include paromomycin, quinacrine and furazolidone

PREVENTION the ways of prevention are: • high level of social sanitation • proper personal hygiene • boiling only drinking water • consumption exclusively of clean food • treatment of infected persons as humans acts as reservoirs for the infection

Tapeworms = Cestodes SEGMENTED WORMS

• tapeworms exhibit a great variety of sizes: - D. latum: up to 10 m (even more in big animals) - T. solium: 2 -8 m - T. saginata: 4 -10 m - E. granulosus: 3 -6 mm

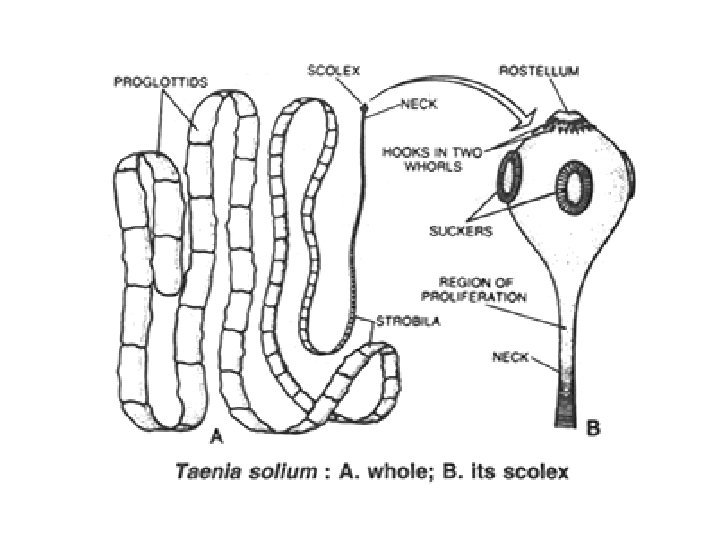
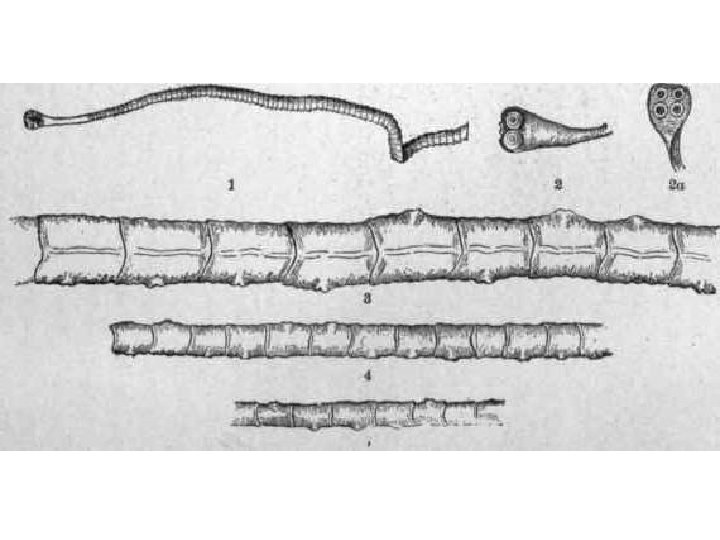
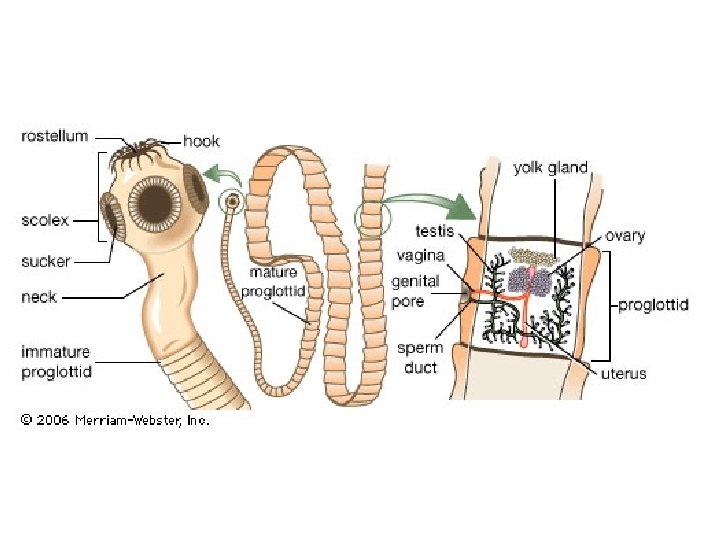
the body always consists of: • a scolex • a neck • the stobila (proglottids)

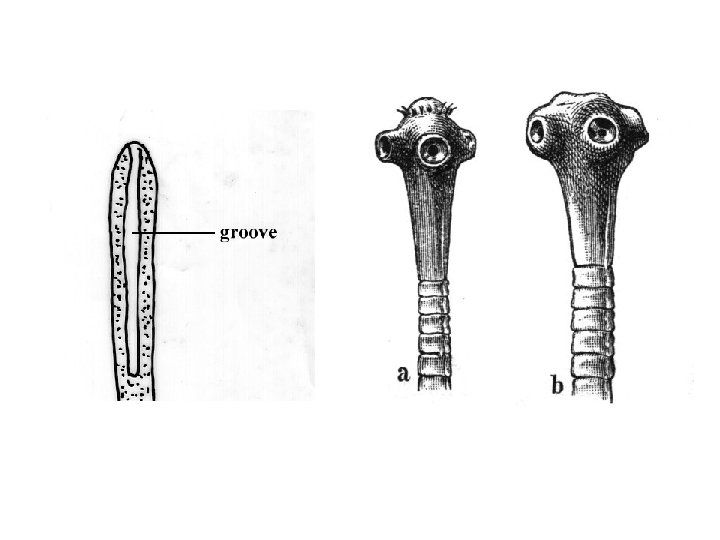
the scolex may be equipped with three types of attaching organs: - suctorial grooves = BOTHRIA - cup-like sucking disks = ACETABULARIA - hooks

• the cestodes are all hermaphroditic organisms ! • each individual proglotid contains a complete set of reproductive organs: both male and female - meaning each segment can produce fertilized eggs! • although these develop at different rates, with the male organs usually developing first (protandry phenomena characteristic for tapeworms)

the different morphology and life cycles determine the distinction of two tapeworm groups Cestoda Pseudophyllidea Cyclophyllidea - Diphyllobothrium sp. - Taenia sp. - Echinococcus sp. - Hymenolepis sp.

LIFE CYCLES

• tapeworms require one or more intermediate host (with the exeption of Hymenolepis nana) • the intermediate host may be of different taxonomic group (from arthropods to mammals), while the definitive host is a vertebrate

• life cycle begins when the segments of the tapeworm break off and pass through in the feces • each segment contains eggs that hatch out in the feces

tapeworms’ eggs Diphyllobothrium latum Taenia sp.
 are eaten by an intermediate host and develop")
• the eggs (containing oncosphere) are eaten by an intermediate host and develop into larvae (different types of larva!)

• a mature tapeworm develops in the intestine of the definitive host after eating of the tissues of infected intermediate host containing larvae

MAN MAY SUFFER BOTH AS THE DEFINITIVE HOST AND THE INTERMEDIATE HOST OF TAPEWORMS

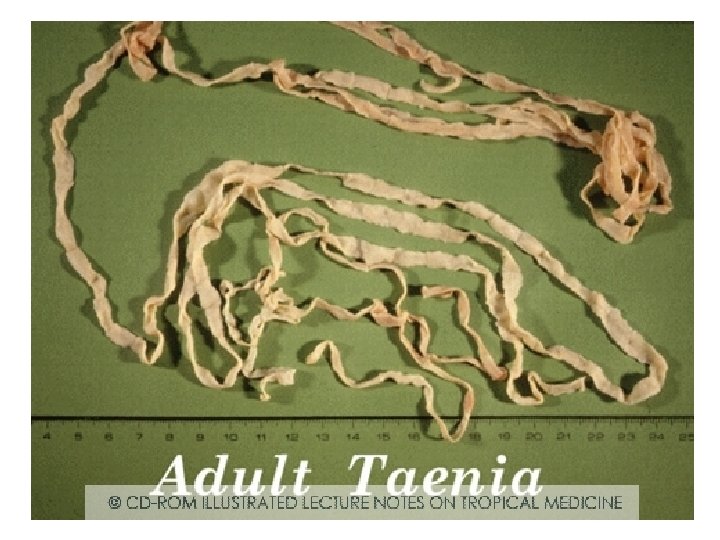
Taenia saginata = beef tapeworm

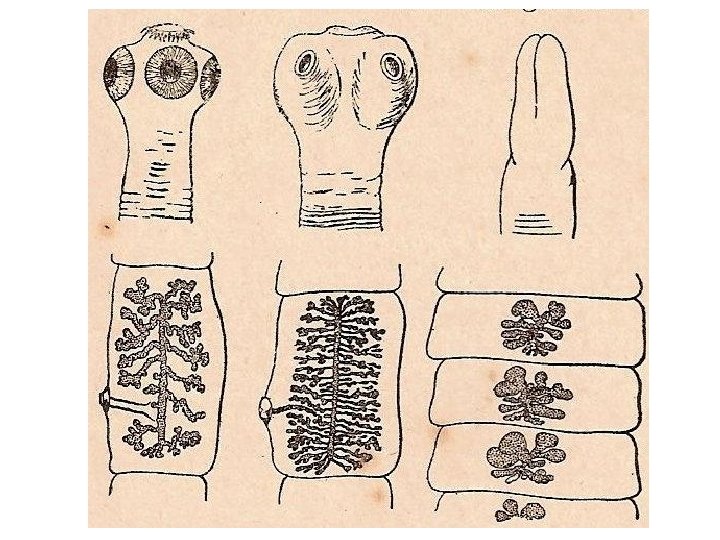
MORPHOLOGY • may measure up to 10 m in length • consists of about 800 proglottides (immature, mature and gravid) • pear-shaped scolex is equipped with 4 suckers without rostellum or hooks • gravid proglottide is rather longer than wider and filled with characterictic branched uterus

Taenia saginata - scolex

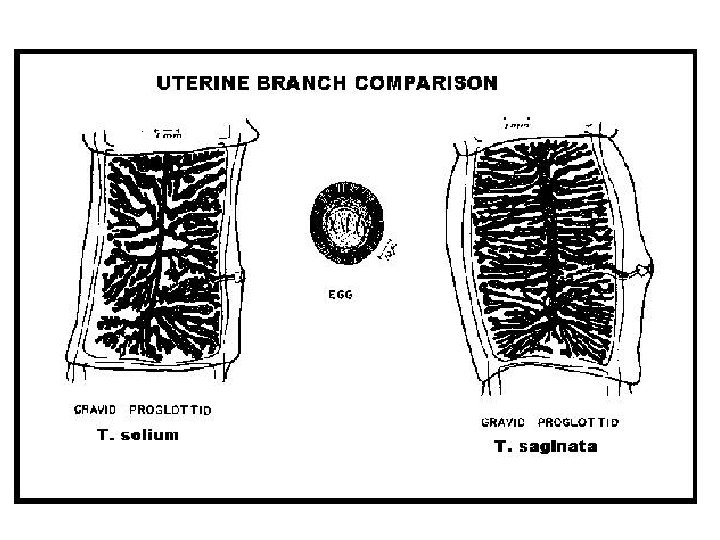
Taenia saginata – gravid proglottide important feature of T. saginata

Taenia spp. egg
")
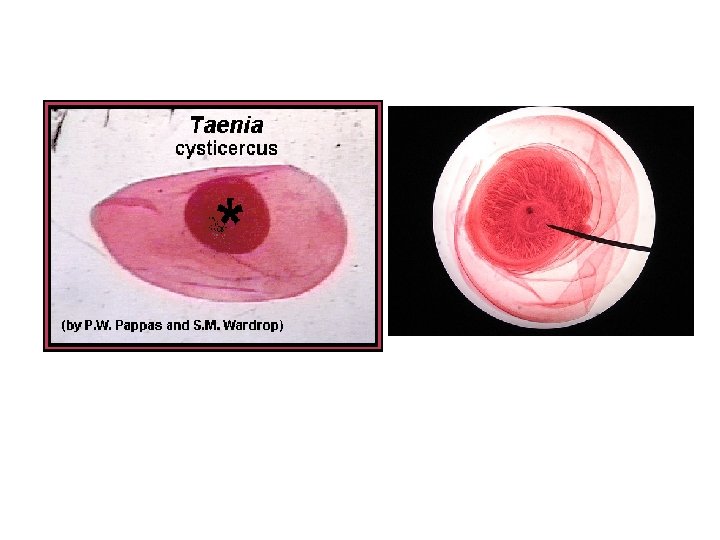
Taenia saginata – second larval stage - bladder cysticercus (cysticercus bovis)

EPIDEMIOLOGY • infections with T. saginata occur worldwide, wherever contaminated raw beef is eaten, particularly in Eastern Europe, Russia, eastern Africa and Latin America. • the infections are more often in areas of low sanitation, where the infection of cattle is frequent (in environment contaminated with human feces)

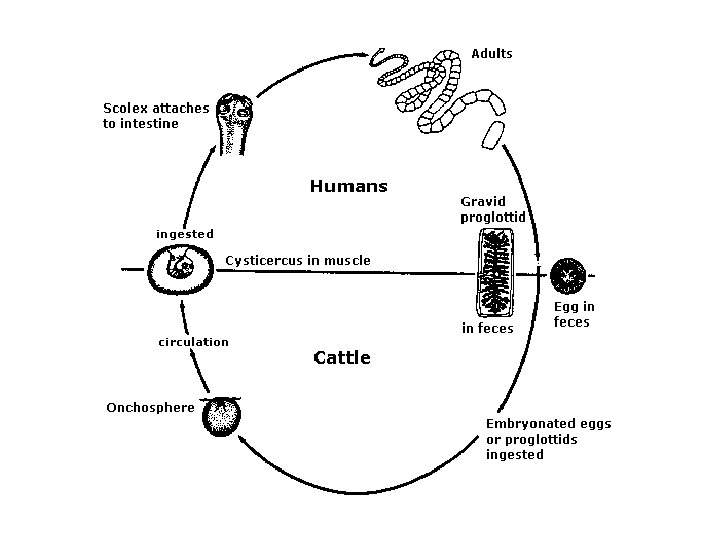
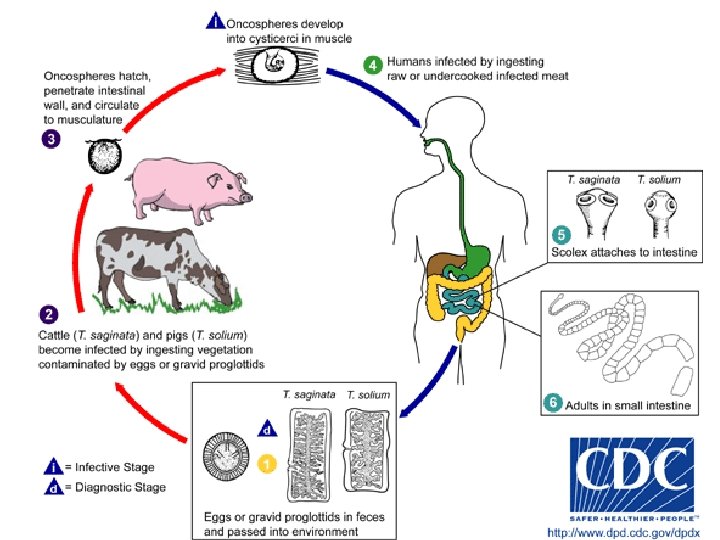
• T. saginata involves cattle as intermediate host and human as definitive host • source of infection for human is raw and undercooked beef containing cysticerci (oral route of infection) • strobilar forms develop during 2 to 3 months and eggs can be detected in the stool 2 to 3 months after the tapeworm infection is established

LIFE CYCLE

DISEASE • called taeniosis, teaniarhynchosis, beef tapeworm infection • usually asymptomatic • if clinical symptoms occur they are: loss of appetite, weight loss, digestive problems including abdominal pain and upset stomach, rarely also the inflammation of small intestine, diarrhea and appenditicis

• patients with T. saginata taeniasis often experience more symptoms that those with T. solium because the T. saginata tapeworm is larger in size • the most visible symptom of taeniasis is the active passing of proglottids (tapeworm segments) through the anus and in the feces • in rare cases, tapeworm segments become lodged in the appendix, or the bile and pancreatic ducts

DIAGNOSIS • made by examination of stool samples and based on the detection of gravid proglottides and eggs • the differential species diagnosis between T. saginata and T. solium is important (based on number of lateral uterine branches in gravid proglottide)

TREATMENT • praziquantel or niclosamide

PREVENTION • the most important way to prevent taeniasis is to cook meat to safe temperatures (a food thermometer should be used to measure the internal temperature of cooked meat) • beef meat inspection!!! and treatment of infected persons are important for control of the disease

USDA recommends the following for meat preparation: • for Whole Cuts of Meat (excluding poultry) cook to at least 145°F (63°C) as measured with a food thermometer placed in the thickest part of the meat, then allow the meat „to rest” for three minutes before carving or consuming. • for Ground Meat (excluding poultry) - cook to at least 160°F (71°C); ground meats do not require a rest time.

Taenia solium = pork tapeworm
 • scolex is")
MORPHOLOGY • usually 4 m in lenght (up to 8 m) • scolex is equipped with 4 suckers, rostellum and double crown of hooks (about 30) • gravid proglottides are longer than wider like T. saginata, but they have less letaral uterine branches!!I • eggs are indistinuishable from T. saginata

Taenia solium - scolex

Taenia solium – gravid proglottide important feature of T. solium
")
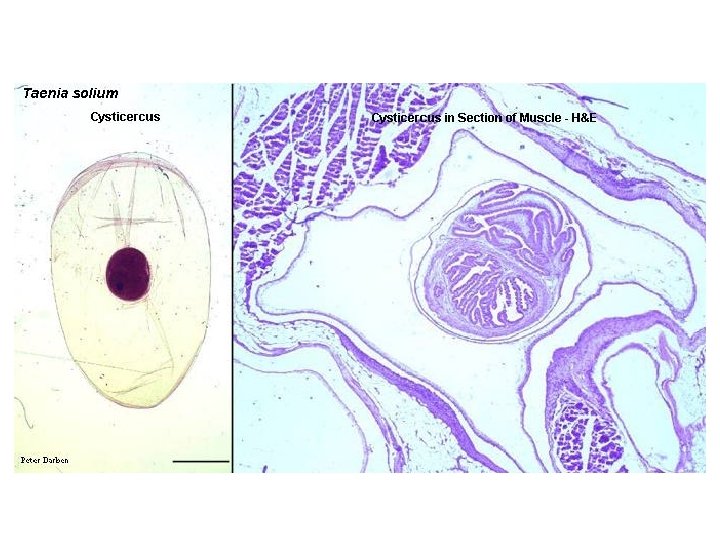
Taenia solium – second larval stage - bladder cysticercus (cysticercus cellulose)

EPIDEMIOLOGY • infections are found worldwide • more prevalent in under-developed communities with poor sanitation and where people eat raw or undercooked pork • higher rates of illness have been seen in people in Latin America, Eastern Europe, sub-Saharan Africa, India, and Asia

• T. solium involves pigs as intermediate host and human as definitive host • source of infection for human is raw and undercooked pork containing cysticerci (oral route of infection) • strobilar forms develop during 2 to 3 months and eggs can be detected in the stool 2 to 3 months after the tapeworm infection is established

 AND !!! cysticercosis • the intestinal taeniosis")
DISEASE • called taeniosis (pork tapeworm infection) AND !!! cysticercosis • the intestinal taeniosis is similar to that caused by T. saginata • however, when T. solium eggs are ingested (accidentally) a disease called cysticercosis may occur, which can be a very serious disease


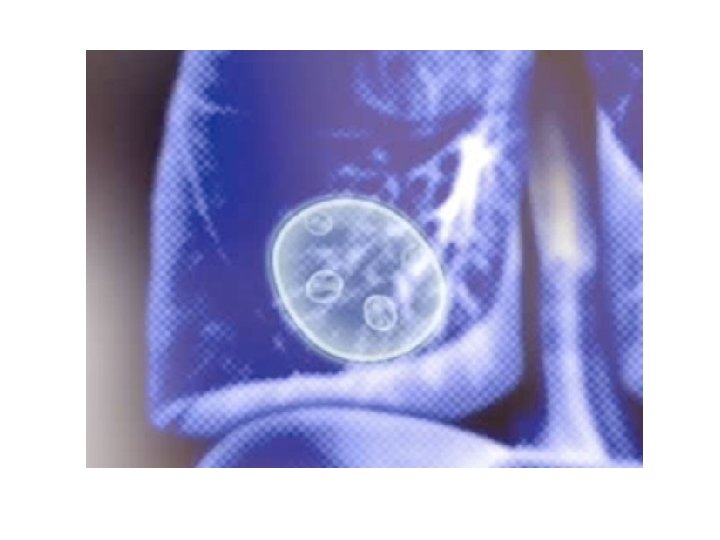
• cysticercosis is a parasitic tissue infection caused by larval cysts of the pork tapeworm • these larval cysts infect brain, muscle, eye or other tissues and are a major cause of adult onset seizures, increased intracranial pressure and various levels of altered mental status in most lowincome countries

brain with larvae

neurocysticercosis

• an individual acquires cysticercosis from ingesting eggs excreted by a person who has an intestinal tapeworm • several means of transmission of this infection are known: 1. EGZOINFECTION: eating food (water, vegetables) contaminated with T. solium eggs

• people living in the same household with a tapeworm carrier have a much higher risk of getting cysticercosis than others asymptomatic tapeworm carrier might accidentally contaminate food i. e. while preparing it for others
")
2. EGZOAUTONIFECTION - people with poor hygiene who have taeniasis (with or without symptoms) will shed tapeworm eggs in their feces and might accidentally ingest them 3. ENDOAUTONIFECTION - eggs may get into small intestine during antiperistalsis in carriers of the adult forms of the tapeworm

DIAGNOSIS • the same like T. saginata made by examination of stool samples and based on the detection of gravid proglottides and eggs • the differential species diagnosis between T. saginata and T. solium is important (based on number of lateral uterine branches in gravid proglottide)

• diagnosis of cysticercosis requires some additional methods like X-ray examination, biopsy, computerized tomography (CT scans) and MRI • on suspicion of cysticercosis, differentiation with other parasitic (i. e lung fluke) viral, bacterial and mycotic etiological agents should be done • immunological test may be also helpful

TREATMENT • praziquantel or niclosamide • in case of cysticercosis surgical removement of cysticercus larvae may be needed – even if the cyst were destroyed by medication they still can cause serious inflammatory process, specially in the brain

PREVENTION • the most important way to prevent taeniasis is to cook meat to safe temperatures (a food thermometer should be used to measure the internal temperature of cooked meat) • pork meat inspection!!! and treatment of infected persons are important for control of the disease

Echinococcus granulosus

• the disease results from being infected with the larval stage of a tiny tapeworm and is one of the most serious human disease caused by larval cestode • human is intermediate host for Echinococcus granulosus !!!

MORPHOLOGY • strobilar form of this tapeworm is VERY SMALL: 2 -6 mm in lenght • it consists of scolex equipped with four suckers and rostellum with a double crown of hooks, neck and three proglottides: immature, mature and gravid


 contain oncospheres surrounded by their envelopes and are")
• infective eggs (30 -40µm) contain oncospheres surrounded by their envelopes and are similar to Taenia eggs

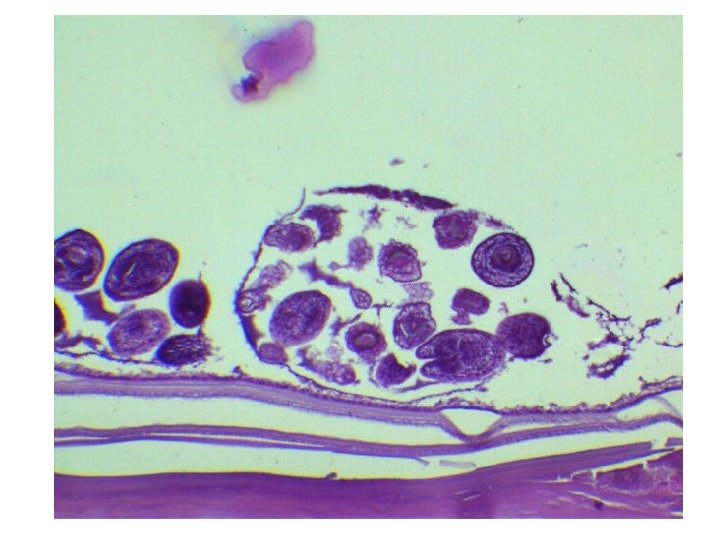
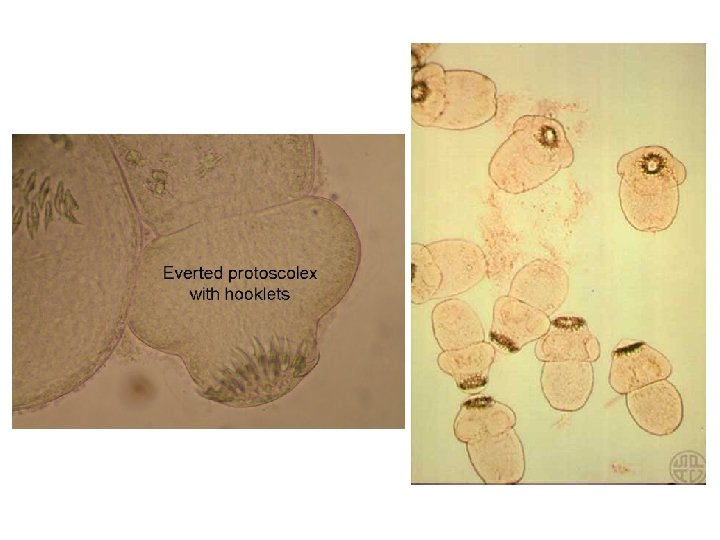
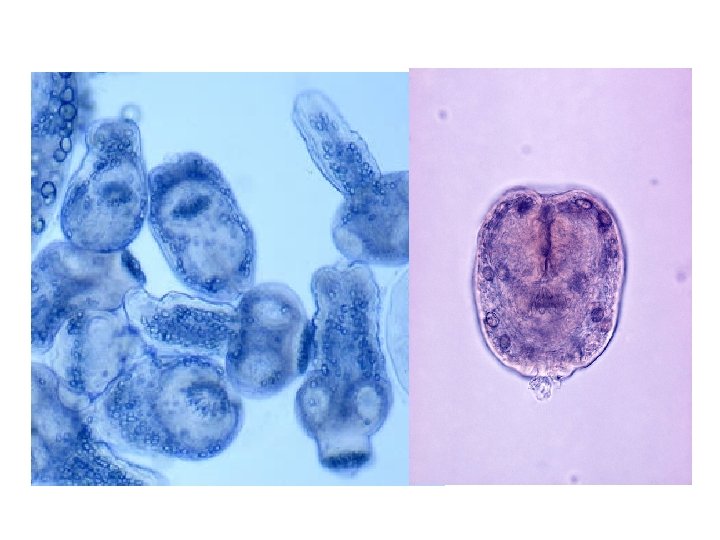
• second larval stage is the bladder uniocular hydatid cyst that is filled with fluid and may reach up to 20 cm!!! in diameter an hold as much as 15 liters of fluid • it possesses external laminated acellular cuticula and inner germinal layer from which the daughter cysts and brood capsules derive
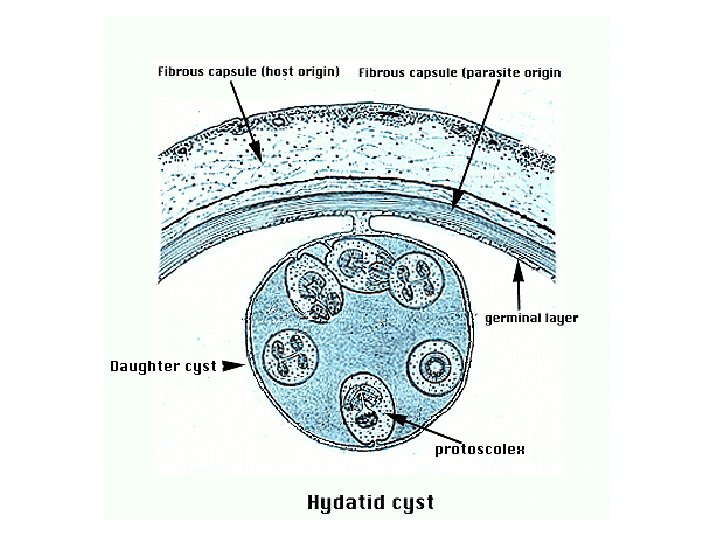
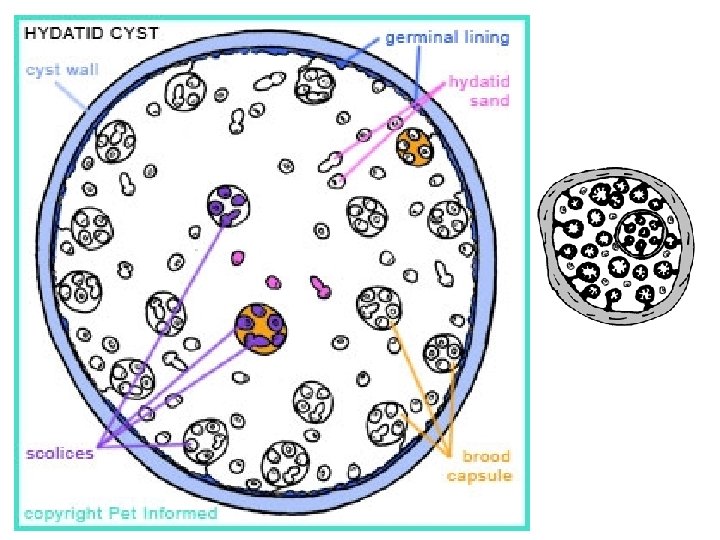
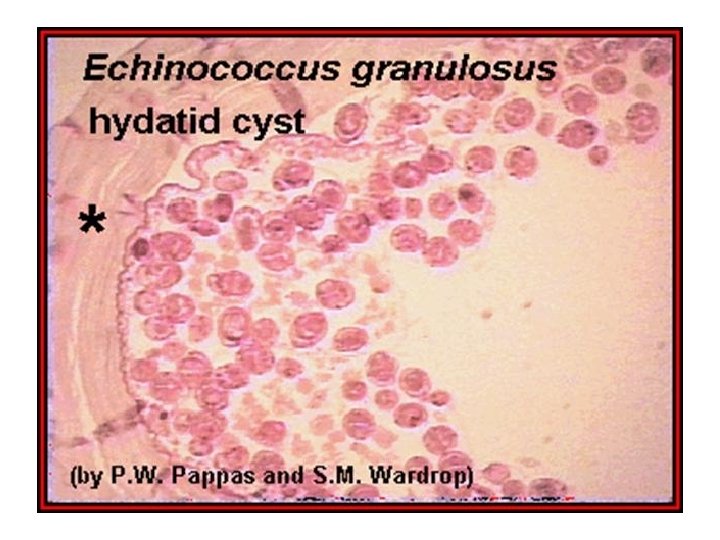
 that may sink")
• inside the capsules the protoscolices develop (millions of them) that may sink to the bottom of the bladder forming socalled hydatid sand

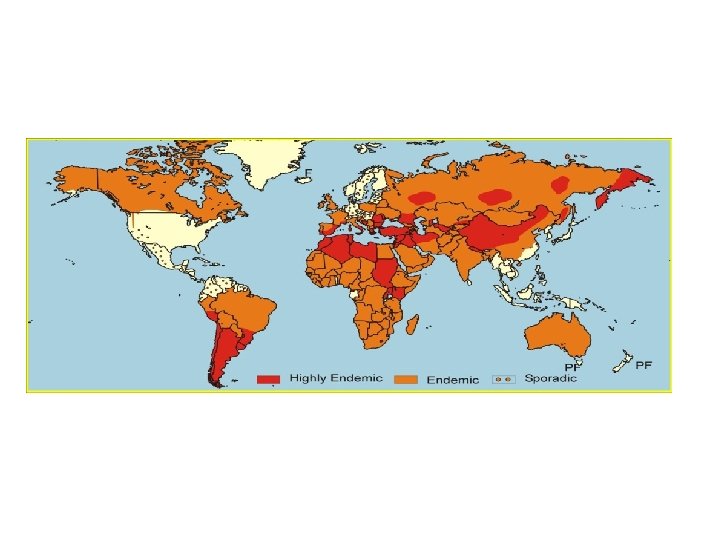
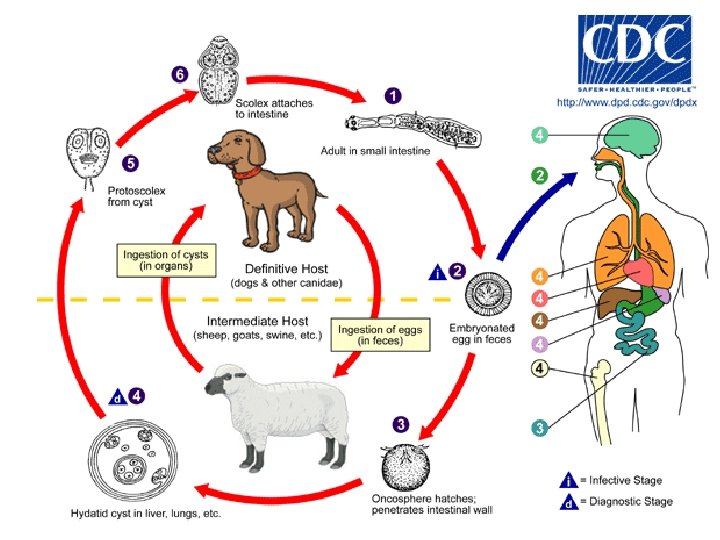
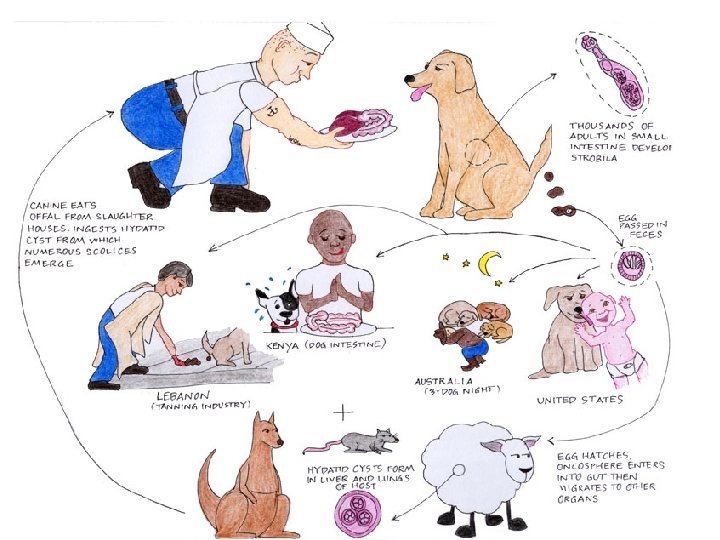
EPIDEMIOLOGY • cosmopolitan tapeworm found in Africa, Europe, Asia, Central and South America, and in North America • the intermediate hosts may be herbivorous mammals (specially sheep) and also MAN • the definitive host are carnivores, particularly DOGS

Map of distribution

• main source of human infection are infected dogs and food or water contaminated with their eggs • transmission of this tapeworm to human is ONLY by INGESTION of the infective EGGS (oral route) • oncospheres hatch in the human intestine and migrate to organs, like liver or lungs where they develop
, hydatid disease, hydatidosis • it often remains asymptomatic")
DISEASE • called cystic echinococcosis (CE), hydatid disease, hydatidosis • it often remains asymptomatic until hydatid cysts containing the larval parasites grow large enough to cause discomfort, pain, nausea and vomiting

• the cysts are mainly found in the liver and lungs but can also appear in the spleen, kidneys, heart, bone and central nervous system (including the brain and eyes) • the sypmtoms are related with the organs that are affected !!!


• the cysts grow over the course of several years before reaching maturity and the rate at which symptoms appear typically depends on the location of the cyst • cyst rupture - most frequently caused by trauma may cause mild to severe anaphylactic reactions, even death, as a result of the release of cystic fluid

DIAGNOSIS • imaging techniques, such as CT scans, ultrasonography, and MRIs are used to show the presence of E. granulosus cysts (if they are calcified) • after a cyst has been detected, serologic tests (immunological methods) may be used to confirm the diagnosis

• radiological and ultrasonografic examination may be also confirmed by direct microscopic indentification of the hydatid sand • diagnosis may require fine-needle biopsy that should be made with care because of danger of anaphylactic shock



TREATMENT • surgery remains the most effective treatment to remove the cyst and can lead to a complete cure • some cysts are not causing any symptoms and are inactive - those cysts often go away without any treatment
")
• chemotherapy, cyst puncture, and PAIR (percutaneous aspiration, injection of chemicals and reaspiration) are also used to support or replace surgery and seems to be effective treatments for cystic echinococcosis

PREVENTION • based on health education, maintenance of high personal hygiene - avoidance of any food or water that may have been contaminated by fecal matter from dogs • in endemic regions, household dogs should be regularly de-wormed

Roundworms = Nematodes

• elongated • cylindrical • tapered at both ends • exhibit a great variety of size (from a few mm to many cm in length)

• the body is nonsegmented and covered with non-cellular CUTICLE that is secreted by underlaying hyperdermis • the cuticle is shed four times during nematode development as the FOUR MOLTS take place
 is elongated and complete with a mouth")
• the digestive system (alimentary track) is elongated and complete with a mouth at the anterior end an anus near the posterior end

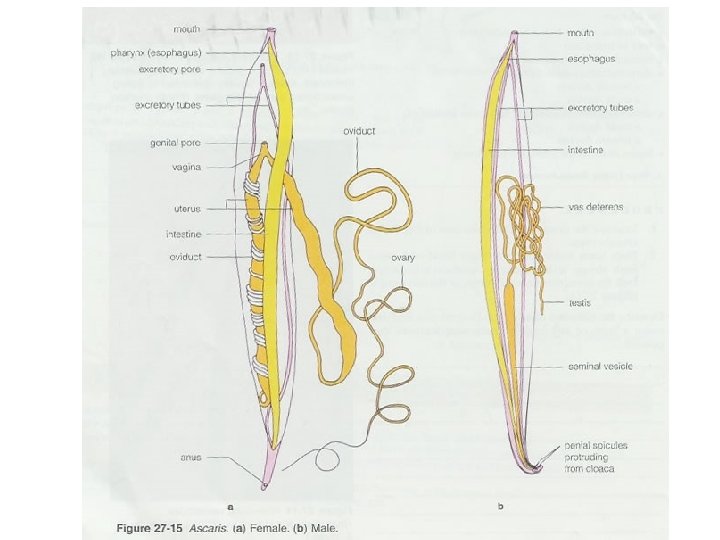
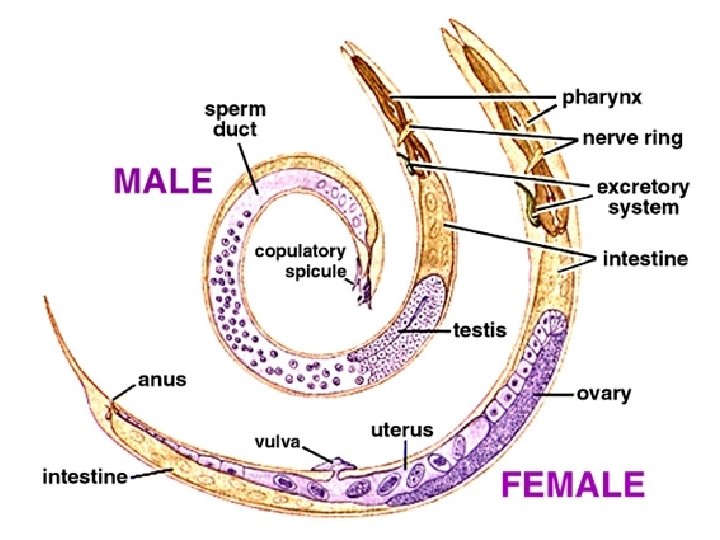
• most nematodes are DIOECIOUS and show sexual dimorphism • the males are usually smaller and they have characteristic curved tail

• the reproductive system is tubular • the females have usually paired, while males single reproductive organs

• most parasitic nematodes are monoxenous - have simple life cycle • very rarely they have complex life cycles

• nematoda that cause human disease are of extreme medical importance – humans are mainly the definitive host (for those medically important) • they mostly locate in alimentary track • sometimes they locate in other organs and tissue

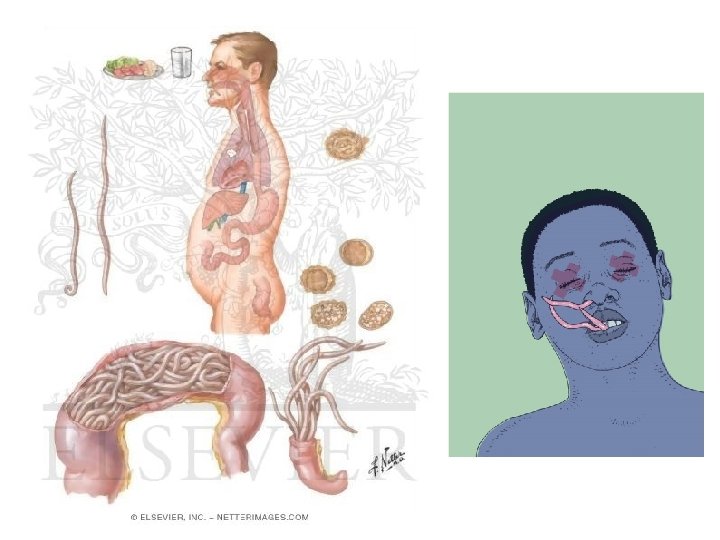
2. Ascaris lumbricoides = the common roundworm

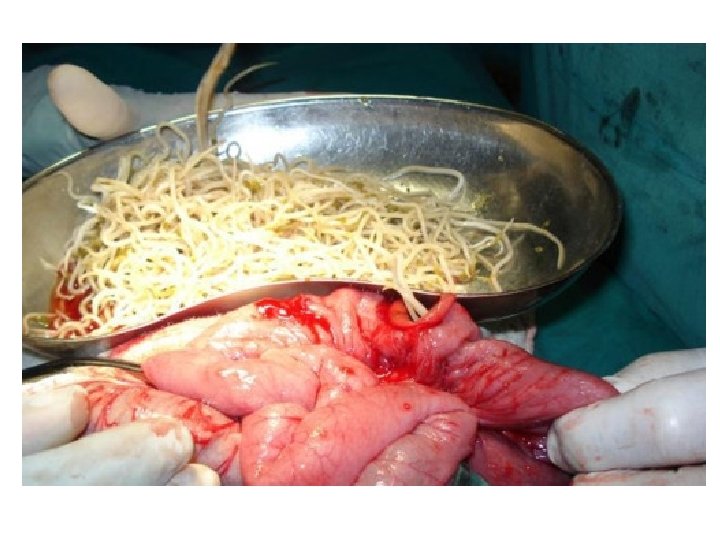
MORPHOLOGY • it is the largest roundworm parasitizing the human intestine • adult females: 20 to 35 cm • adult male: 15 to 30 cm



unfertilized egg – nonoperculated, oval in shape

fertilized egg – shorter and equipped with thick yellow-brown shell



EPIDEMIOLOGY • world-wide monoxenous parasite • an estimated 1300 millions of people in the world are infected with Ascaris lumbricoides (carriers!) • Ascaris, hookworm and whipworm are known as soil-transmitted worms and together, they account for a major burden of disease worldwide

• Ascaris infection is one of the most common intestinal worm infections • it is found in association with poor personal hygiene, poor sanitation and in places where human feces are used as fertilizer

Geographic Distribution

LIFE CYCLE

• sources of infection are soil and raw vegetables contaminated with feces of carriers containing infective eggs (fertilized!) – eggs must develop in extrenal environment • the parasite is transmitted by eating raw vegetables (contaminated) – oral route • in children, direct transmission by eating contaminated soil may happen
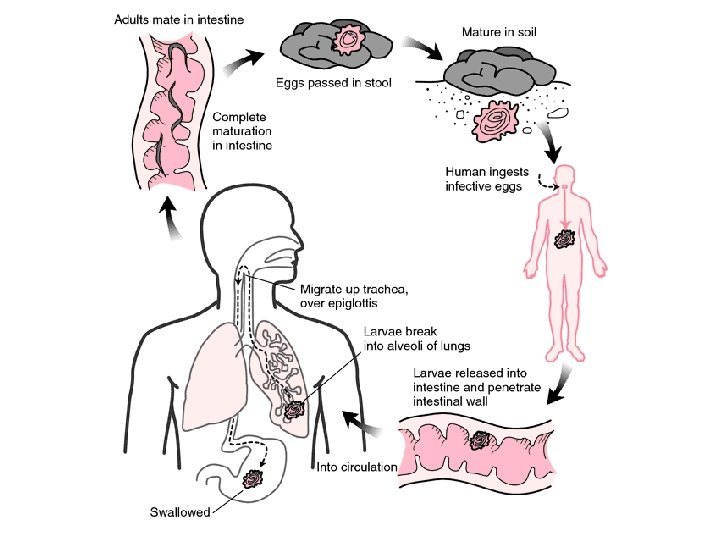

DISEASE • people infected with Ascaris often show no symptoms • in intestinal phase some non-specific symptoms may occur and they include abdominal discomfort and pain, vomiting and both obstruction, and diarrhea • perforation of intestine may also occur

• heavy infections can cause intestinal blockage and impair growth in children • the ectopic sites may be also included, like appendix, bile duct or pancrea

• other symptoms such as cough, asthmalike symptoms and damage of the lungs are due to migration of larvae through the body • each Ascaris developmental stage may also cause allergic reactions or make infected persons more susceptile to other infections (i. e. viral) • it very dangerous for small children, in which can be fatal

DIAGNOSIS • the standard method for diagnosing ascariasis is by identifying Ascaris eggs using a microscope or finding the adults in a stool sample • eggs may be difficult to find in light infections thus a concentration procedure is recommended • radiografic methods are also helpful


TREATMENT • ascariasis is treatable with medication prescribed by doctors • albendazole and mebendazole are the drugs of choice for treatment • the drugs are effective - infections are generally treated for 1 -3 days and appear to have only few side effects

PREVENTION the best way to prevent ascariasis is to always: KEEP GOOD HYGIENE PRACTISE 1. avoid ingesting soil that may be contaminated with human feces, including where human fecal matter or wastewater is used to fertilize crops

2. wash, peel or cook all raw vegetables and fruits before eating, particularly those that have been grown in soil that has been fertilized with manure 3. wash your hands with soap and warm water before handling food 4. teach children the importance of washing hands to prevent infection …
- Slides: 155