GI Topics Appendicitis Diverticulitis Obstruction Mesenteric Ischemia Thomas

GI Topics: Appendicitis Diverticulitis Obstruction Mesenteric Ischemia Thomas Vu Brookdale Emergency Medicine Residency Conference July 1 st, 2020

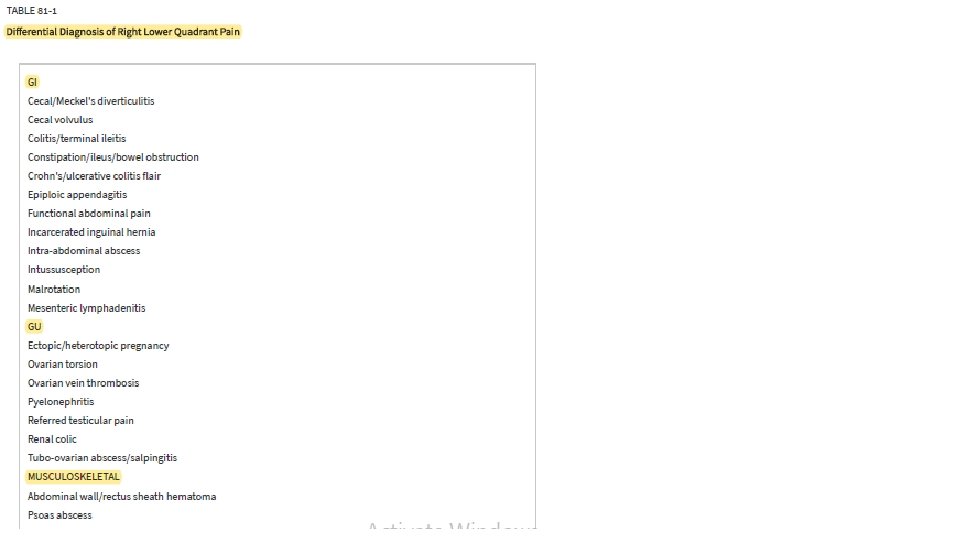
1. 8 yo. M presents with abd pain, has low grade fever and is tender RLQ. Labs show normal wbc. US performed, no evidence of appendicitis. XR KUB shows constipation. • Provider discharges patient with miralax, diagnosis = constipation. Is this appropriate? 2. 85 yo. M h/o diverticulitis presents with left lower abdominal pain, fever, vomiting, and found to be tachycardic in triage. Labs show WBC 13. 5. • Provider provides dose of IV antibiotics, prescribes oral antibiotics and discharges patient. Is this appropriate? 3. 45 yo. F h/o hysterectomy, cholecystectomy p/w abdominal pain. Found to have a large bowel obstruction, WBC 22, elev lactic acid. • Provider believes it to be secondary to previous abdominal surgeries, orders NG tube, admits to medicine with surgery consult. Is this appropriate?

Appendicitis • Background • Clinical Features • Diagnostics • Management

Appendicitis – Background • 250 -300 K appy’s/year in US • Lifetime risk: 12% M, 25% F • Most Common Ages: 10 -19 yo • 1: 1500 pregnancies (#1 non OB surgical emergency in pregnancy)

Appendicitis – Background • Luminal obstruction of appendix, typically by fecalith • Other causes – lymphatic tissue, gallstone, tumor, parasites • Increased pressures, vascular insufficiency; can lead to perforation • Early – visceral innervation, periumbilical/central abdominal discomfort • Later – parietal peritoneal irritation @ RLQ (Mc. Burney’s)

Quiz 1

Appendicitis – Background • 50% patients with “atypical” presentations due to anatomic variations: • Retrocecal appendix = R flank or pelvic pain • Malrotation = LLQ pain • Pregnancy Uterus Displacement = RUQ pain (RLQ still #1 area)

Appendicitis – Clinical Features • Early – nonspecific malaise, indigestion, bowel irregularity, anorexia ( common but not universal) • Then periumbilical/central abdominal pain, +/- fever / vomiting • Then migrates to RLQ • Can have flank pain, dysuria, hematuria if close to urinary tract
 and movement •")
Appendicitis – Clinical Features • Worsens with deep inspiration (peritoneal irritation) and movement • Can have pain remittance if perforation (intraluminal obstruction release) • Rebound, involuntary guarding if peritonitis

Quiz 2

Appendicitis – Clinical Features • Rovsings – RLQ/Mc. Burney’s pain elicited when palpating LLQ • Psoas – abd pain upon extension of R leg at the hip while laying on left side • Obrturator – pain elicited with internal/external rotation of flexed R thigh at the hip

Quiz 3

Appendicitis – Clinical Features • Increasing Likelihood • Rigidity, + Psoas, Fever, or Rebound • Children (<18 yo) • Fever = LR +3. 4 • Also RLQ pain/TTP • Absence Fever = LR -0. 32 • Decreasing Likelihood • Prior similar pain, absence of RLQ pain, absence of classic migration • Adult • RLQ Pain, TTP Sn 81%, Sp 53% • LR +8 • Fever LR +1. 94 No H/P finding sufficient to rule in/out In children or adults
")
Appendicitis – Diagnostics • Still largely a clinical diagnosis • Scoring Systems (Alvarado, Samuel) • Alvarado Sn ~72% compared to clinical judgement 93% of appendicitis as most likely diagnosis

Appendicitis – Diagnostics Labs • WBC • Increase may be earliest marker of inflammation • Normal not uncommon, some also leukopenic • No clear consensus on utility • ESR / CRP • Not high enough Sn / Sp • Combined WBC + CRP: Sn 98% but not Sp • Adjunts: UA, Upreg

Quiz 4

Appendicitis – Diagnostics Imaging • Not always necessary in straightforward cases, children • US • Initial imaging of choice for pregnant and children; also nonobese • Safe, fast, well tolerated, costeffective • Normal Appendix Features: absence of peristalsis, lack of change in configuration, small • Appy Findings: thickened, noncompressible appendix >6 mm in diameter, sometimes identifies appendicolith, surrounding edema • Better at ruling in than out • Limits: operator skills, retrocecal appy, perf, excessive guarding, bowel gas, gravid uterus, obese • Sn 86%, PPV 95%

Appendicitis – Diagnostics

Appendicitis – Diagnostics Imaging • CT Abd Pelv • Findings: dilated >6 mm appendix thickened wall, peri-appendiceal inflammation, +/appendicolith/abscess • Sn >94%, PPV >95% • Non contrast equally as good? • Sn 93 -95%, PPV 92% • MRI • Consider for pregnant women if available but avoid IV gadolinium (crosses placenta)

Quiz

Appendicitis – Management • Early surgical consultation before imaging in high suspicion cases can help management • Appendectomy • Antibiotics – • • Zosyn 4. 5 g or Unasyn 3 g or Cefoxitin 2 g or Flagyl 500 mg + Cipro 400 mg • Adjunts • Analgesics, Anti-emetics • Nonoperative? Not standard

Appendicitis – Management Disposition: • Surgery if diagnosed • Can be same-day surgery and discharge without admission • Not clear diagnosis but suspicion stays high, extended ED or hospital stay with serial exams • Alternatively if stable & reliable can be d/c if scheduled return to ED or PCP (w/in 12 hrs) • Able to tolerate pain and PO • Special considerations: Pregnant women, children

Quiz

Welcome to Brookdale Dr. Rebecca Siegel!

Quiz

Welcome to Brookdale Dr. Bahar Pourshariati!

Diverticulitis • Background • Clinical Features • Diagnostics • Management

Diverticulitis – Background • Diverticulosis incidence increasing with age: 5% in 40 s, 30% in 50 s, >70% by age 85 • Diverticula: small herniation @ vasa recta (vasculature) penetrates circular muscle layer of colon • Diverticulitis: inflammation, translocation of bacteria, microperforation / abscess / phlegmon formations

Diverticulitis – Background • Most common bacteria – Bacteroides, Peptostreptococcus, Clostridium, Fusobacterium, E coli & other G neg rods • Altered bowel motility leads to high intraluminal colonic pressures, diverticula formation • Risk factors: smoking, obesity, lack of active lifestyle • US almost exclusively left-sided desc/sigmoid colon

Quiz 5

Diverticulitis – Clinical Features • Classic – LLQ, fever, leukocytosis • RLQ can be in Asian populations • Intermittent or constant • Change in bowel habits (diarrhea or constipation), n/v, anorexia, urinary sx • TTP mild to moderate, or peritonitis with rebound/guarding

Quiz 6

Diverticulitis – Diagnostics Labs – rarely diagnostic • Can help excludes other disease • Imaging not needed - If previous history diverticulitis confirmed and is similar to previous presentations • Imaging needed – If not previously confirmed, episode differs from previous • Exclude other pathologies, evaluate for complications

Diverticulitis – Diagnostics Imaging • CT – preferred modality; helps eval severity of disease, complications • Increased soft tissue density within pericolic fat, presence of diverticula, bowel wall thickening >4 mm, soft tissue mass (phlegmon), pericolic fluid collection (abscess) • US – operator dependent • Limited by habitus; hard to diagnose complications

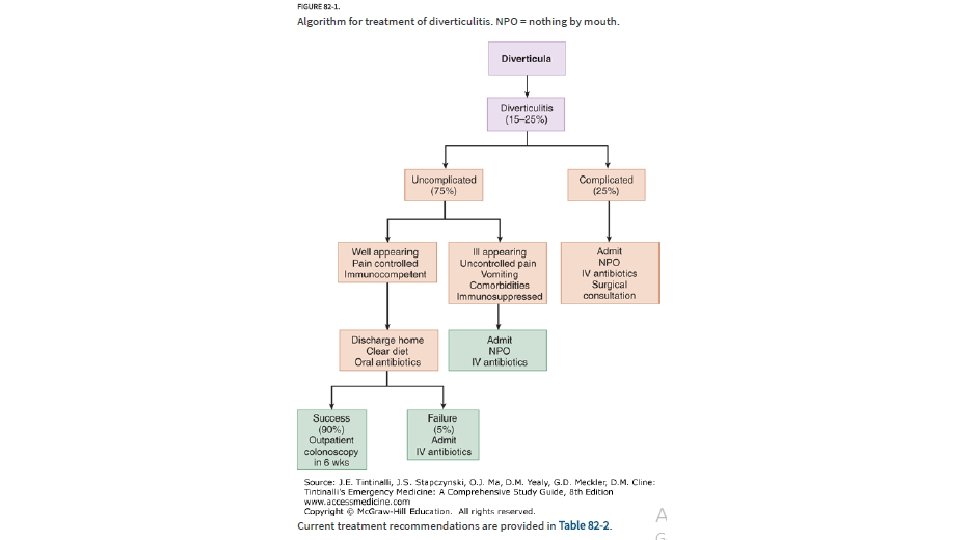
Diverticulitis – Management

Quiz 7

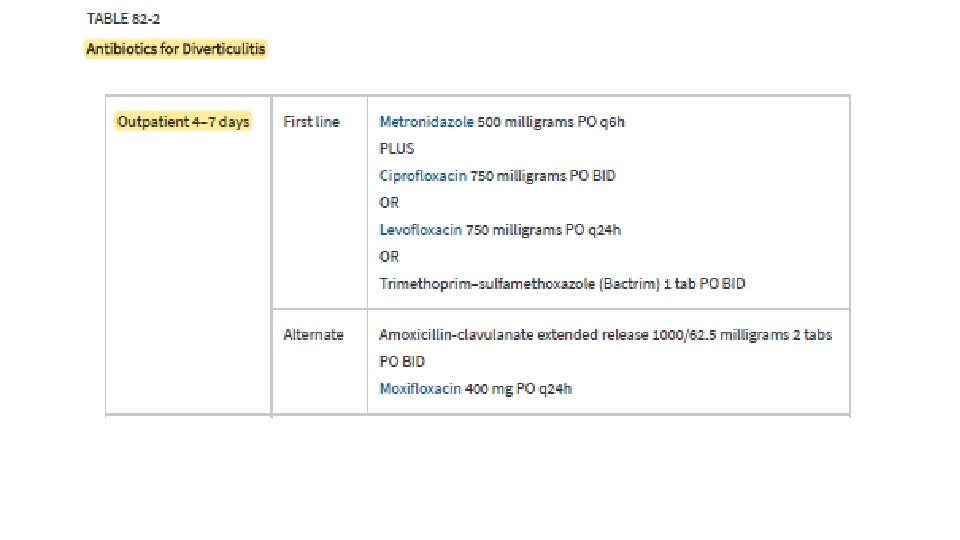
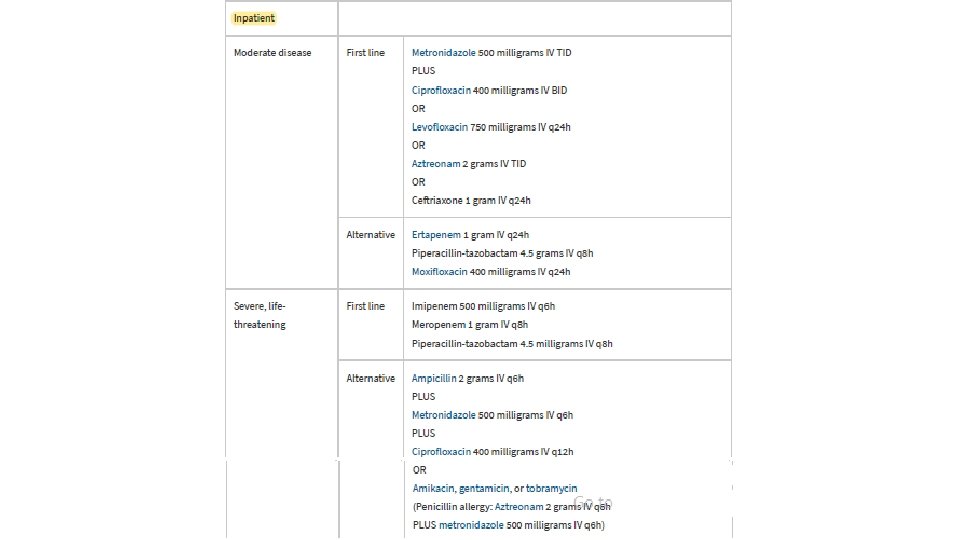
Diverticulitis – Management Uncomplicated • Bowel rest/liquid diet, Oral Antibiotics, +/- Dietary Modifications • ? Hold antibiotics? Possibly no additional benefit, but no consensus yet Complicated • Bowel rest, + IV Abx, + Admit • Hinchey Classification Scheme • Abscess/Phlegmon: +/-Percutaneous Drainage • Perforation: + Volume Resuscitation +/- Ex Lap

Diverticulitis – Management Uncomplicated • Bowel rest/liquid diet, Oral Antibiotics, +/- Dietary Modifications • ? Hold antibiotics? Possibly no additional benefit, but no consensus yet Complicated • Bowel rest, + IV Abx, + Admit • Hinchey Classification Scheme • Abscess/Phlegmon: +/-Percutaneous Drainage • Perforation: + Volume Resuscitation +/- Ex Lap

Diverticulitis – Management Epiploic Appendagitis • Small fat filled sacs sitting near colon linen that become inflamed • Possibly due to increasing obesity • Due to torsion or venouns • Higher rates of recurrence, thrombosis complications, surgical • Sharp abdominal pain, n/v interventions • Mimics appy, diverticulitis, chole Meckel’s • Typically incidental CT finding • Crampy abd pain, n/v, bleeding • Benign, self-limiting course Young Patients (<40 yo) • Small proportion but growing • Dx: Radionuceotide or CT • Tx: Surgical • Tx: Pain management

Diverticulitis – Management Epiploic Appendagitis • Small fat filled sacs sitting near colon linen that become inflamed • Possibly due to increasing obesity • Due to torsion or venouns • Higher rates of recurrence, thrombosis complications, surgical • Sharp abdominal pain, n/v interventions • Mimics appy, diverticulitis, chole Meckel’s • Typically incidental CT finding • Crampy abd pain, n/v, bleeding • Benign, self-limiting course Young Patients (<40 yo) • Small proportion but growing • Dx: Radionuceotide or CT • Tx: Surgical • Tx: Pain management

Diverticulitis – Management Epiploic Appendagitis • Small fat filled sacs sitting near colon linen that become inflamed • Possibly due to increasing obesity • Due to torsion or venouns • Higher rates of recurrence, thrombosis complications, surgical • Sharp abdominal pain, n/v interventions • Mimics appy, diverticulitis, chole Meckel’s • Typically incidental CT finding • Crampy abd pain, n/v, bleeding • Benign, self-limiting course Young Patients (<40 yo) • Small proportion but growing • Dx: Radionuceotide or CT • Tx: Surgical • Tx: Pain management

Quiz

Welcome to Brookdale Dr. Rasheeda Rickman!

Quiz

Welcome to Brookdale Dr. Bannet Muhoozi!

Obstruction • Background • Clinical Features • Diagnostics • Management

Obstruction – Background • Inability of GI tract to pass food and bowel contents due to mechanical blockage or adynamic ileus • 15% of ED visits for abdominal pain • Due to intrinsic or extrinsic factors

Obstruction – Background • Bowels become congested, lack of absorption, develop vomiting • Volume depletion, hemoconcentration, electrolyte imbalance • Then, renal failure or shock • Bowel distension causes increased intraluminal pressures exceeding venous pressure • Leads to ischemia, septicemia, bowel necrosis, shock 70% mortality

Quiz 8

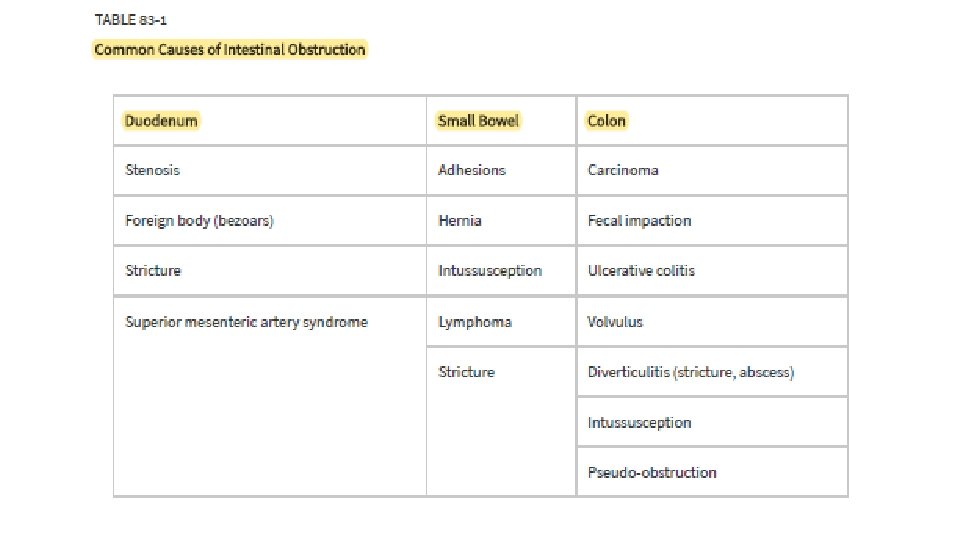
Obstruction – Background Small Bowel Obstruction • 4 x more common than LBO Large Bowel Obstruction • #1 Adhesions (weeks to months, • #1 Neoplasms years after surgery) • Rarely adhesions • #2 Hernia Incarceration • Other: Diverticulitis (Excess Edema), Sigmoid Volvulus • Other: Cancer, Polyps, Bariatric (Elderly, Bedridden, Psych, or on surgery, Gallstones, Anticholinergics) Lymphomas/Intussusception, Bezoars, Radiation Enteritis, Trauma

Obstruction – Background Small Bowel Obstruction • 4 x more common than LBO Large Bowel Obstruction • #1 Adhesions (weeks to months, • #1 Neoplasms years after surgery) • Rarely adhesions • #2 Hernia Incarceration • Other: Diverticulitis (Excess Edema), Sigmoid Volvulus • Other: Cancer, Polyps, Bariatric (Elderly, Bedridden, Psych, or on surgery, Gallstones, Anticholinergics) Lymphomas/Inutssusception, Bezoars, Radiation Enteritis, Trauma

Quiz

• Coronal views

Obstruction – Clinical Features • No historical feature reliably predicts SBO • Almost all have abdominal pain • Crampy, intermittent, diffuse • Inability pass flatus, constipation • Partial SBO can still pass flatus/stool • Abd distension, tenderness • Varying degrees of each • High pitch bowel sounds/rushes • Presence of stool on rectal exam does not exclude

Obstruction – Diagnostics Labs • Screening CBC and Chem • Very elevated WBC can suggest bowel gangrene, abscess, peritonitis, mesenteric vascular occlusion • Chem – can show vol depletion • Procalcitonin – may predict bowel ischemia

Obstruction – Diagnostics Imaging • Flat & Upright, Lateral Decub XRs • Air fluid levels, distended bowels, coiled spring sign • Not sensitive enough to rule out • CT • Modality of choice, high sensitivity • Localizes; identifies severity, cause • Oral and IV contrast • Can do without IV if allergy/renal • Often can still diagnose without oral

Obstruction – Diagnostics Imaging • Flat & Upright, Lateral Decub XRs • Air fluid levels, distended bowels, coiled spring sign • Not sensitive enough to rule out • CT • Modality of choice, high sensitivity • Localizes; identifies severity, cause • Oral and IV contrast • Can do without IV if allergy/renal • Often can still diagnose without oral

Quiz 9

Obstruction – Management • Vigorous IVF • Most SBO - can be managed nonoperatively • NGT – • not always required, typically depends on surgeon preference • Surgical Emergencies: Closed Loop Obstruction, Bowel • Most LBO – most require surgery Necrosis, Cecal Volvulus • Tumor resection if malignancy • Endoluminal stents • BS Abx – Zosyn, Carbapenem Dispo – Admit to surgery or to medicine with surgery consult

Quiz
 to Brookdale Dr. Amy Plasencia!")
Welcome (Back) to Brookdale Dr. Amy Plasencia!

Quiz

Welcome to Brookdale Dr. Shruti Kamat!

Mesenteric Ischemia • Background • Clinical Features • Diagnostics • Management

Mesenteric Ischemia – Background • #1 occlusion site = SMA • Typically involves small bowel (jejunum) & right colon • Left colon with collateral flow, less commonly involved • Mean age = 70 yo; Women >>Men

Mesenteric Ischemia – Background Four Distinct Types 1. Arterial Embolism 3. Venous Thrombosis 2. Arterial Thrombosis 4. Nonocclusive • Risks/Causes: Dysrhythmia (A. Fib), Valve Disease, MI • Risks/Causes: Atherosclerotic Disease • Risks/Causes: Prior thrombosis, Hypercoagulable (pregnancy, CA) • Risks/Causes: Hypovolemic state, Heart Failure / Cardiogenic Shock, Sepsis, Diuretic Use

Quiz 10

Mesenteric Ischemia – Clinical Features • **Pain out of proportion to exam • Abdomen soft, no guarding • Pain often around poorly localized, or left sided @ watershed areas (splenic flexture, recto-sigmoid junction) • Severe, generalized, colic • Bloody stools

Mesenteric Ischemia – Diagnostics Labs • General abdominal labs with elevated Lactic Acid/WBC, Hyperphosphatemia Imaging • CTA Abdomen/Pelvis (bowel wall edema most common finding) • Mesenteric Angiogram = gold standard Portal Vein Gas Bowel Wall Edema Pneumatosis Intestinalis

Mesenteric Ischemia – Management General • IVF resuscitation • BS IV Abx • 2 nd Gen Ceph + Flagyl OR • Levofloxacin + Flagyl OR • Zosyn • Anticoagulation – Heparin • If no contraindications • Some recommend delay 48 hrs

Quiz 11

Mesenteric Ischemia – Management Four Distinct Types 1. Arterial Embolism 3. Venous Thrombosis • Papaverine (Antispasmodic) infusion • Heparin/warfarin alone or in OR combination with surgery • Surgical embolectomy OR • Mesenteric Artery Bypass Surgery OR • TPA intra-arterial thrombolysis with IR 4. Nonocclusive • +/- Resection of bowel after any of above • +/- 24 -48 hr second look surgery 2. Arterial Thrombosis • Angio +/- stent placement or surgical revascularization with/without stent placement OR • Surgical revascularization • • Transcatheter vasodilation via: PGE 1, alprostadil PGI 2, epoprosternol Antispasmodic

Mesenteric Ischemia – Management Dispo • Admit with consult of one or more of the following: • IR • Vascular • Surgery

Quiz

Welcome to Brookdale Dr. Abrar Justin Ahmed!

Quiz

Welcome to Brookdale Dr. Brandon Buchel!

Quiz

Welcome to Brookdale Dr. Ama Asare!

1. 8 yo. M presents with abd pain, has low grade fever and is tender RLQ. Labs show normal wbc. US performed, no evidence of appendicitis. XR KUB shows constipation. • Provider discharges patient with miralax, diagnosis = constipation. Is this appropriate? 2. 85 yo. M h/o diverticulitis presents with left lower abdominal pain, fever, vomiting, and found to be tachycardic in triage. Labs show WBC 13. 5. • Provider provides dose of IV antibiotics, prescribes oral antibiotics and discharges patient. Is this appropriate? 3. 45 yo. F h/o hysterectomy, cholecystectomy p/w abdominal pain. Found to have a large bowel obstruction, WBC 22, elev lactic acid. • Provider believes it to be secondary to previous abdominal surgeries, orders NG tube, admits to medicine with surgery consult. Is this appropriate?

Quiz Review 1. Mcburney’s Point • 1/3 distance ASIS to umbilicus 2. Physical signs of Appy 3. Absence of RLQ does not rule out appendicitis 4. US findings of Appendicitis • Thickened, non-compressible, • Rovsings –RLQ/Mcburneys pain >6 mm, edema, +/- appendicolith elicit when palpating LLQ • Psoas - abd pain upon extension of 5. Symptoms of Diverticulitis R leg at the hip while laying on left • Vomiting, constipation, anorexia, side urinary symptoms • Obturator – pain elicited with internal/external rotation of flexed 6. Diagnosing Diverticulitis R thigh at the hip • CT/imaging not always needed

Quiz Review 7. Diverticulitis Management • Uncomplicated do not require admission • Complicated need antibiotics • Abscess/phlegmon/perf may need invasive interventions 9. NG Tube – Not always needed • Most SBOs treated non-op, most LBO need interventions • Definitely needs surgery – closed loops, necrosis, cecal volvulus; add Abx 10. M. Ischemia Features 8. Causes of Obstruction • SBO #1 = Adhesions, LBO #1 = Neoplasms; others (both) polyps, gallstones, intussusception, bezoars, radiation enteritis, trauma • Pain out of proportion to exam, generalized, associated bloody stools 11. M. Ischemia Mgmt • IVF, BS IV Abx, Anticoagulation • Additional treatment depends on type – embolectomy vs bypass vs stent vs vasodilation • Typically needs bowel resection

Quiz

Resources • Tintinalli 8 e Chapter 81 – Acute Appendicitis • Tintinalli 8 e Chapter 82 – Diverticulitis • Tintinalli 8 e Chapter 83 – Bowel Obstruction
- Slides: 89