GI Imaging Densities l Xray allows visualization of







 Esophogram l Barium Swallow l UGI series l Modified Barium")


 l Cricopharyngeus muscle spasm l Reflux esophagitis")





































- Slides: 49
GI Imaging
Densities l X-ray allows visualization of different densities -Air -Fat -Water -Metal
Visualization of the Esophagus l Different density required for visualization i. e. : contrast
Contrast Agents l Water Soluble – Gastrografin – Low-osmolality l Inert – Barium sulfate
Single vs. Double Contrast l Improved mucosal visualization
Fluoroscope l Real-time -ray video l Multiple sequential images l Spot films x
Barium Studies l (Video) Esophogram l Barium Swallow l UGI series l Modified Barium Swallow
Gastroesophageal Reflux
GERD & Barium l Visualization of refluxing barium l Patient position l Valsalva l Usefulness is arguable
GERD Secondary Signs l Hiatal Hernia (HH) l Cricopharyngeus muscle spasm l Reflux esophagitis l Benign stricture l Barrett’s esophagus l Aspiration pneumonia
Hiatal Hernia l Extension of stomach into chest through esophageal hiatus l 2 types: – Sliding 95% – Para-esophageal 5% § l May Not associated with GERD be more prominent when supine
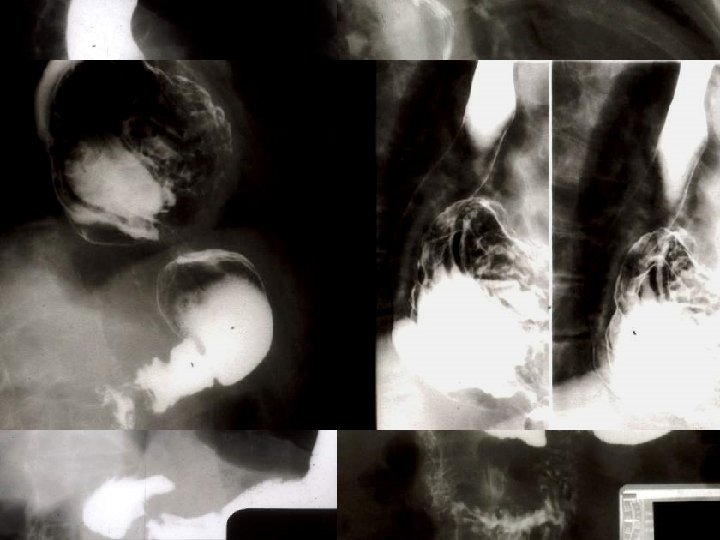
Cricopharyngeous Muscle l Posterior wall of pharyngoesophageal junction l Normally relaxes with swallowing to allow passage of food l Incomplete relaxation can be seen as protective mechanism in GER patients l Smooth impression at C 5 -6 level
Cricopharyngeous Muscle Spasm
Reflux Esophagitis l Begins distally l Thickened folds l May have associated linear ulcers
Benign Stricture l Distal or mid-esophagus l Smooth walls l May be partially distensible
Barrett’s Esophagus l In approx. 10% of untreated reflux patients l Metaplasia of normal squamous epithelium to a gastric columnar epithelium l Nodular or granular mucosa l Look for focal ulceration, stricture, and cancer (15% or 30 x increase)
Barrett’s Esophagus
Aspiration Pneumonia l Appearance will vary with amount of aspirate, patient position, reaction to aspiration l Often bilateral, associated atalectasis l Posterior and basal areas more common
Aspiration Pneumonia
Aspiration
Esophageal Cancer
Detection l Barium studies are not as sensitive as endoscopy, but more readily available l Suspect cases referred on to endoscopy l CT, MRI not suitable for screening
Barium Swallow Patterns 1. Annular constricting l Most common l Many variations Polypoid mass 3. Infiltrative 2. l In submucosa, may simulate benign stricture 4. Ulcerated mass
Esophageal Cancer
Esophagobronchial fistula
Tumor Staging l CT most commonly used l Endoscopic ultrasound in some centers
Computed Axial Tomography
Computed Axial Tomography
CT Staging l Wall thickness l Infiltration of paraesophageal fat planes l Regional invasion (trachea, pleura, pericardium, vertebrae etc…) l Lymphadenopathy l Distant Metastases
Normal CT
Invasive Cancer
Endoscopic Ultrasound l Smaller lesions l Assess wall involvement
Esophageal Motility
Normal Motility l Best seen prone l 3 phases: – Oral, pharyngeal, esophageal
Esophageal Phase l Primary wave: – Initiated by swallowing reflex l Secondary Wave: – As response to esophageal distension
Normal Swallow
Abnormal Motility l Non-specific finding l Seen in reflux esophagitis, radiation injury, caustic ingestion, myxedema, diabetes mellitus…
Corkscrew esophagus l Tertiary esophageal waves – Non-propulsive – Corkscrew or beaded appearance
Scleroderma l Fibrosis of smooth muscle l Dilated esophagus with widely patent GEJ l Resultant reflux l Reflux esophagitis => ulceration => stricture (mild) => Barrett’s => neoplasm
Scleroderma
Achalasia l Diffusely decreased or absent peristalsis l Lower esophageal sphincter fails to relax l Smooth, tapered distal esophageal narrowing l Some passage of food in upright position
Achalasia
Neuromuscular Disorders l Most common => stroke l Parkinsonism, Alzheimer’s, multiple sclerosis, CNS neoplasms, traumatic injury l Modified barium swallow
Zenker’s Diverticulum
Zenker’s l Herniation at posterior midline above UES l Horizontal & oblique fibers of inferior constrictor muscles => Killian’s dehiscence l Associated incomplete cricopharyngeus muscle relaxation l Neck at superior aspect of sac l Midline, but lateral extension with growth
Zenker’s Diverticulum
Zenker’s Diverticulum