GI Grand Rounds Johanna Chan Gastroenterology Fellow Baylor

GI Grand Rounds Johanna Chan Gastroenterology Fellow Baylor College of Medicine 12/13/2012

No conflicts of interest No financial disclosures

HPI • RFC: nausea, vomiting, abdominal pain • 61 yo WM with HCV/Et. OH cirrhosis, admitted with nausea and nonbloody emesis x 3 wks • Dull, diffuse abdominal pain, no radiation • Worse with eating and drinking • Early satiety • Poor PO intake x 3 weeks • No fever, chills, constipation, diarrhea, dysuria, edema

Past Medical History • HCV genotype 3 a ▫ Nonresponder to pegylated interferon and ribavirin in 2004 • HCV/Et. OH cirrhosis, Child Class A • Bladder carcinoma s/p TURBT 1999 • BPH
 • No")
Medications • Omeprazole 20 mg PO daily (recently prescribed at urgent care) • No other OTC medications, including NSAID or aspirin use

Other history • Family history negative for GI malignancy, liver disease • Social history ▫ Current 1 pack/day smoker since teen years ▫ Prior h/o IVDA, none since 1990 s ▫ Prior heavy Et. OH since teen years, quit in 1980 s

Exam • • T 98, BP 108/75, HR 78, RR 12, O 2 sat 98% RA Gen: uncomfortable but nontoxic, NAD, AAOx 4 HEENT: PERRL, EOMI, dry MM, OP clear Neck: supple, no LAD, flat neck veins CV: RRR no m/r/g Lungs: CTAB, no wheeze/crackles Abd: markedly distended, diffusely tender, no guarding, +BS, dull to percussion • Ext: WWP no c/c/e

Labs 125 55 94 147 4. 4 45 5. 6 11. 1 17. 6 52. 3 77% PMNs Total protein 7. 4 Albumin 3. 6 Total bili 3. 1 ALT 109 AST 123 Alk phos 39 187 INR 1. 1 PTT 32 MCV 99

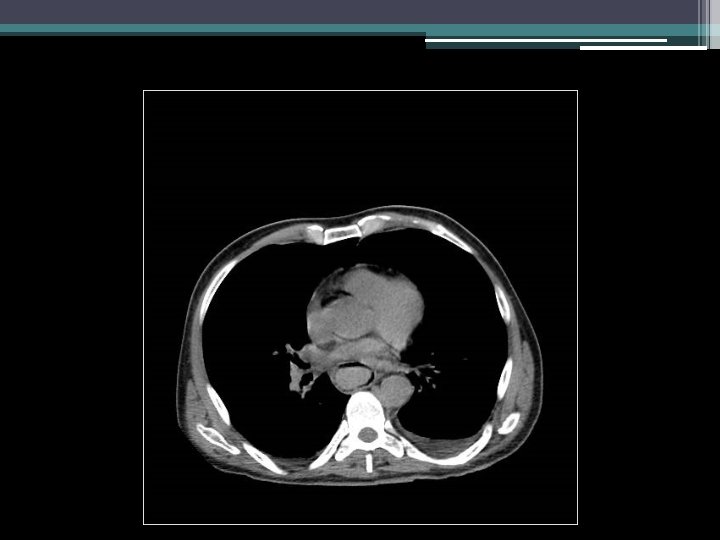
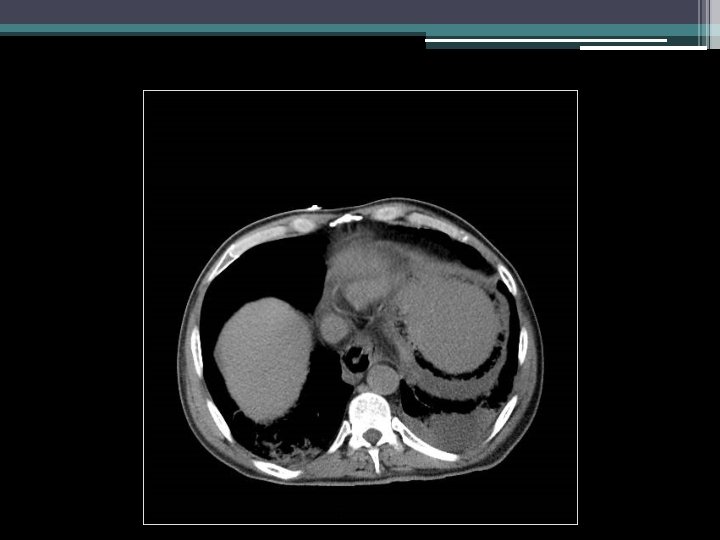
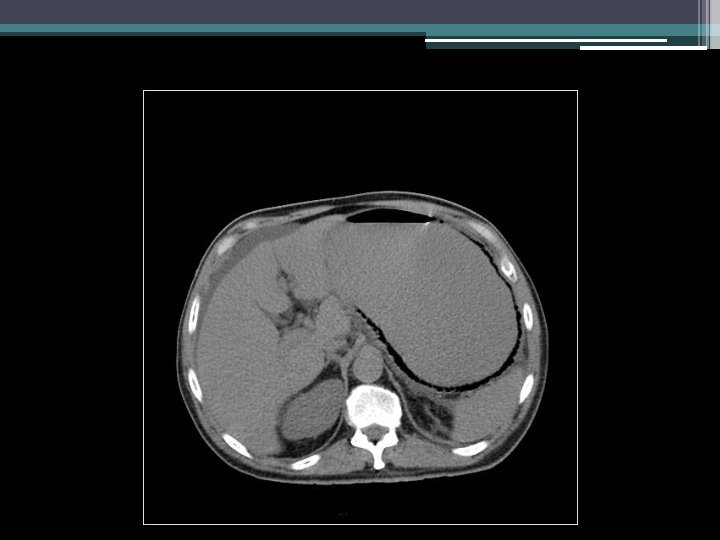
Imaging
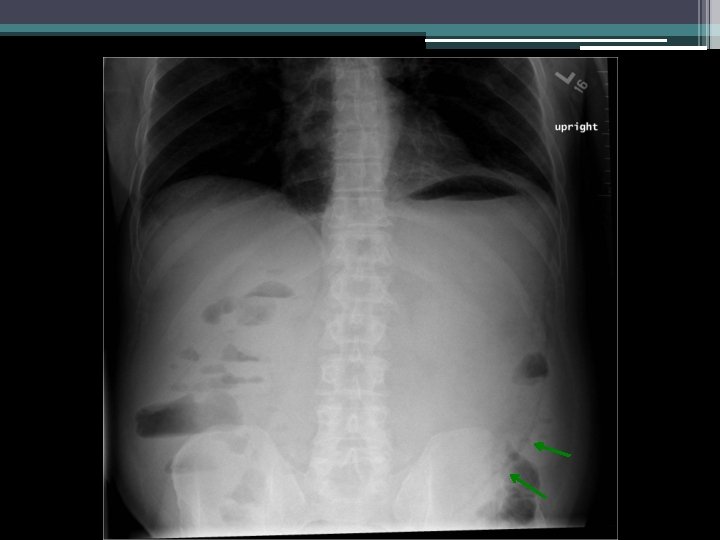


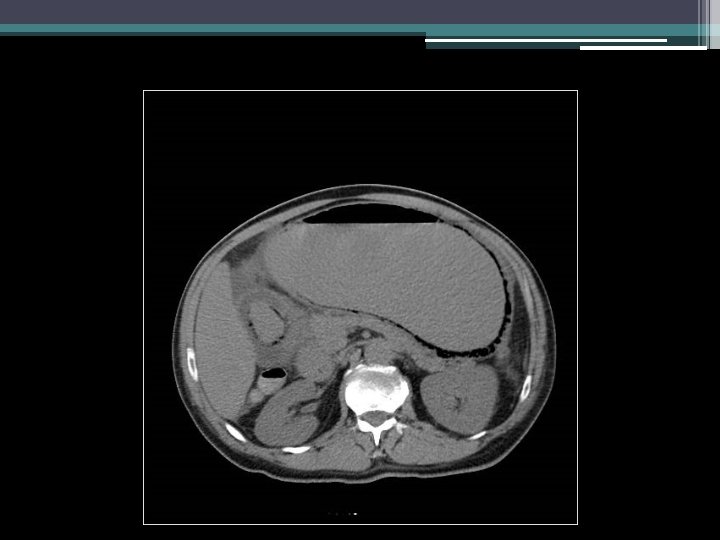
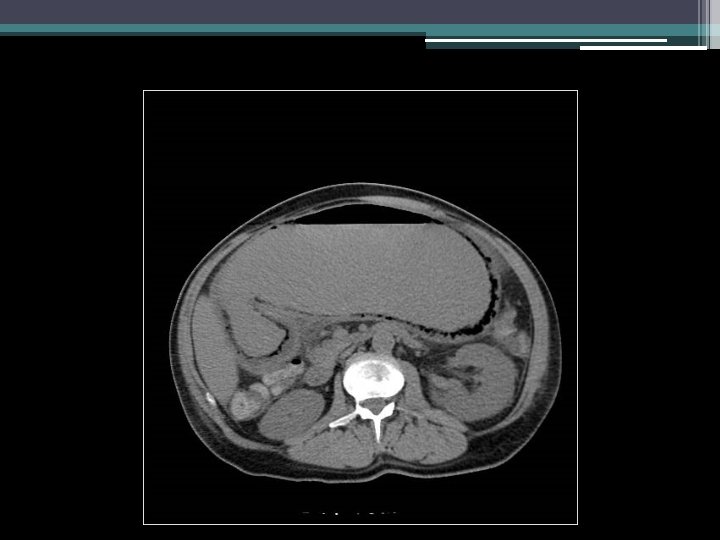
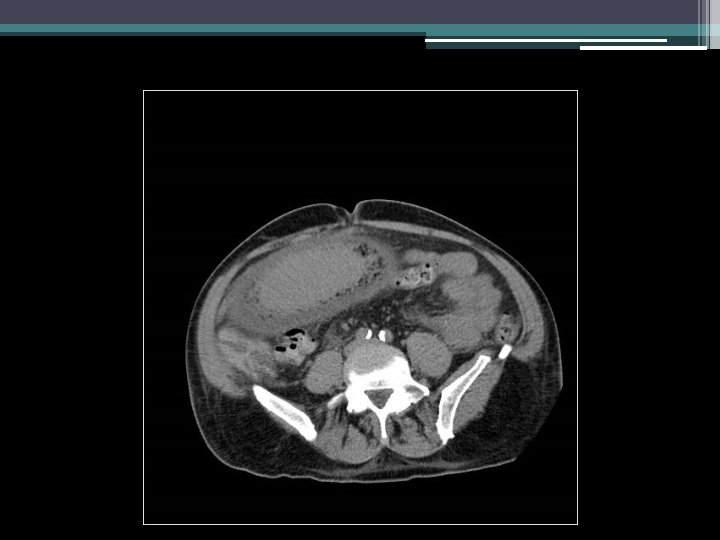

Initial thoughts?

Differential diagnosis?
 NPO +/- NG tube decompression B) Broad-spectrum")
Next steps in management? • • A) NPO +/- NG tube decompression B) Broad-spectrum antibiotics C) Consult surgery D) Endoscopy (and timing? )

Clinical course • • • NPO, IV ceftriaxone and flagyl General surgery consult Negative blood and urine cultures Remained clinically well and nontoxic Symptoms improved Tolerated clear liquids for 2 -3 days

Clinical course • • Return of nausea and vomiting NG tube decompression: >3 L nonbloody output Saline load test markedly positive Repeat KUB


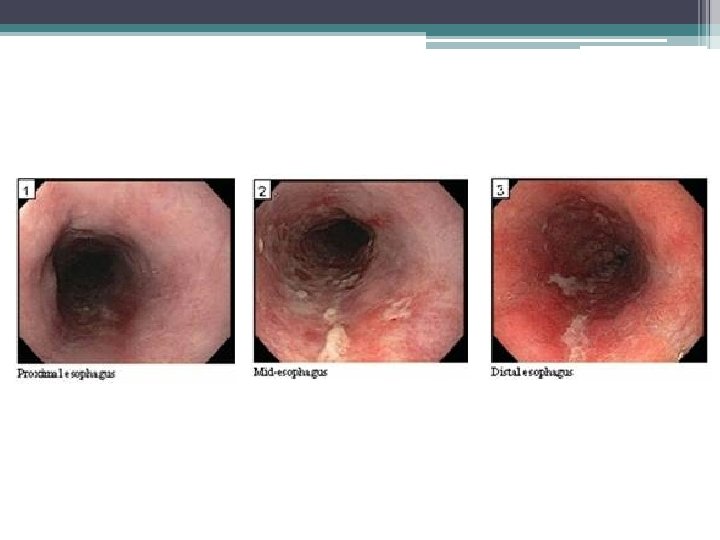
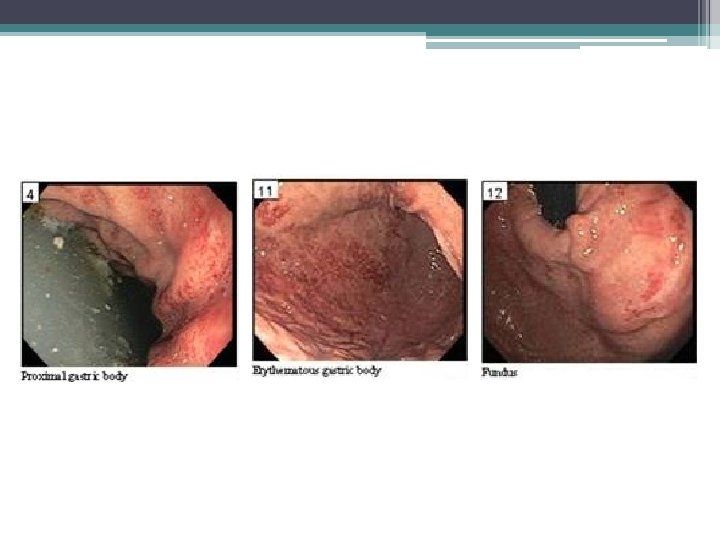
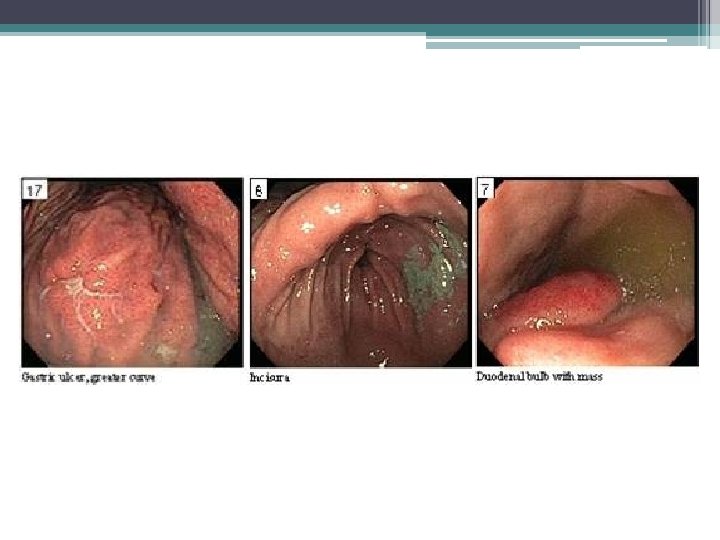
Endoscopy

Gastric emphysema • Diagnosis: gastric emphysema due to gastric outlet obstruction • Pneumatosis intestinalis ▫ Gastric pneumatosis Gastric emphysema Emphysematous gastritis ▫ Pneumatosis coli
? • Differential diagnosis of PI? •")
Clinical questions • What is pneumatosis intestinalis (PI)? • Differential diagnosis of PI? • Management of PI? ▫ Indications for surgery? ▫ Role for endoscopy? • Relation to gastric outlet obstruction?

What is pneumatosis intestinalis? • First described in 1754 by Du Vernoy • Presence of extraluminal bowel gas within bowel wall • Breakdown of mucosal and immunological barrier of intestine, especially in the setting of increased intraluminal pressure Galundiuk S et al. DCR. 1986; (29)5: 358 -363. Heng Y et al. Am J of Gastroenterol. 1995; (90)10: 1747 -1758. Koss LG. Arch Pathol. 1952; (53): 523 -549.
 Incidence")
What is pneumatosis intestinalis? • • 0. 03% in general population (autopsy series) Incidence rising with increasing CT use Most asymptomatic, incidentally detected Complications occur in up to 3% of patients ▫ Pneumoperitoneum, bowel obstruction, volvulus, intussusceptions, hemorrhage Galundiuk S et al. DCR. 1986; (29)5: 358 -363. Heng Y et al. Am J of Gastroenterol. 1995; (90)10: 1747 -1758.
 – 10 -15% by review of 213")
Differential diagnosis for PI • Idiopathic (rare) – 10 -15% by review of 213 cases • Secondary ▫ ▫ Bowel necrosis Mucosal disruption Increased mucosal permeability Pulmonary disease Koss LG. Arch Pathol. 1952; (53): 523 -549. Pear BL. Radiology. 1998; 207(1): 13 -19.

DDx PI: Bowel necrosis • • • Ischemia/infarction Necrotizing enterocolitis Neutropenic colitis Volvulus Sepsis In the stomach, emphysematous gastritis or ingestion of caustic agents

DDx PI: Mucosal disruption • Over-distention (peptic ulcer, pyloric stenosis, annular pancreas, or distal obstruction) • Ulceration, erosions, trauma • Iatrogenic (feeding tubes, stent perforation, sclerotherapy, or surgical or endoscopic trauma) • Connective tissue disease: scleroderma, SLE • Medications that cause bowel distention: sortibol, lactulose

DDx PI: Increased mucosal permeability • Mucosal erosions or defects in intestinal crypts (inflammatory bowel disease) • Immunocompromise (due to steroids, chemotherapy, radiation therapy, or AIDS) with defects in bowel wall lymphoid tissue • Acute graft vs. host disease

DDx PI: Pulmonary disease • • • Chronic obstructive pulmonary disease Asthma Cystic fibrosis Barotrauma After chest tube placement Increased intrathoracic pressure (retching, vomiting, PEEP)

Management of PI • • • Exclude acute intra-abdominal emergency Antibiotics Elemental diet (for pneumatosis coli) High-flow oxygen or hyperbaric oxygen therapy Endoscopic therapy (particularly obstructive symptoms) *No randomized controlled data

Indications for surgery • Clinical indications of bowel ischemia • Combination of PI and serum lactate >2 mmol/L associated with >80% mortality (Hawn et al) • Radiographic signs: ▫ Hepatic portal and portomesenteric venous gas ▫ Vascular distribution suggesting ischemia ▫ Additional abnormal bowel wall findings • Others: obstruction, ileus, toxic megacolon, severe collagen vascular disease Hawn MT et al. Am Surg. 2004; (70)1: 19 -23. Wayne E et al. J Gastrointest Surg 2010; 14: 437.

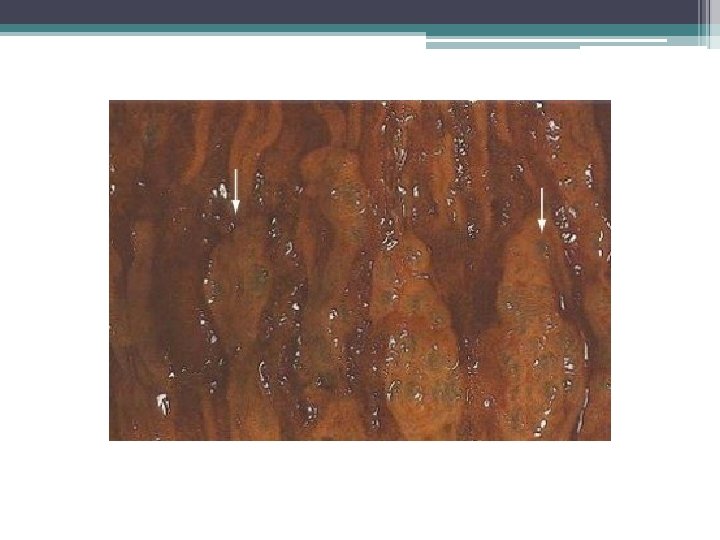
Role for endoscopy • Non-surgical cases • Diagnosis of underlying etiology • Gastric emphysema ▫ Submucosal “bubbles” with pale/bluish mucosa ▫ Deflate when biopsied ▫ Edema, erosions • Emphysematous gastritis ▫ Edematous, friable, ulceration with exudates ▫ Histology: fibrin thrombi, gas-forming organisms, bacterial infiltration, microabscesses Cordum NR et al. Am J Gastroenterol 1997; 92: 692.

Gastric emphysema in relation to gastric outlet obstruction • Well-reported in the pediatric literature • Most commonly due to pyloric stenosis ▫ Also duodenal stenosis, tumor, protracted vomiting • Mortality rate for gastric pneumatosis 41% in adults, 6% in children D’Cruz R et al. J Pediatr Surg 2008 ; 43: 2121 -3. Taylor D et al. Int Pediatr 2000; 15: 117 -20.
: E 227.")
Lim RK et al. CMAJ 2010. 182(5): E 227.

Patient case follow-up • Esophagus, biopsy ▫ Gastric-type mucosa with mild chronic and focally acute inflammation ▫ Intestinal metaplasia • Stomach ulcer, biopsy ▫ Reactive gastropathy • Stomach, random biopsy ▫ Reactive gastropathy with focal chronic inflammation • Duodenum “mass”, biopsy ▫ Mild chronic focally active duodenitis, suggestive of Brunner’s gland hyperplasia

References • Braumann C, Menenakas C, and Jacobi CA. “Pneumatosis intestinalis – a pitfall for surgeons? ” Scandinavian Journal of Surgery. 2005; (94)1: 47 -50. • Cordum NR, Dixon A, Campbell DR. Gastroduodenal pneumatosis: endoscopic and histologic findings. Am J Gastroenterol 1997; 92: 692. • Galundiuk S and Fazio VW. “Pneumatosis cystoides intestinalis: a review of the literature. ” Diseases of the Colon and Rectum. 1986; (29)5: 358 -363. • Hawn MT, Canon CL, Lockhart ME, et al. “Serum lactic acid determines the outcomes of CT diagnosis of pneumatosis of the gastrointestinal tract. ” Am Surg. 2004; (70)1: 19 -23. • Heng Y, Schuffler MD, Haggitt RC, and Rohrmann CA. “Pneumatosis intestinalis: a review. ” American Journal of Gastroenterology. 1995; (90)10: 1747 -1758. • Ho LM, Paulson EK, and Thompson WM. “Pneumatosis intestinalis in the adult: benign to life-threatening causes. ” American Journal of Roentgenology. 2007; (188)6: 1604 -1613.
 • Hoer J, Truong S, Virnich N, Fuzesi L, Schumpelick V. “Pneumatosis")
References (con’t) • Hoer J, Truong S, Virnich N, Fuzesi L, Schumpelick V. “Pneumatosis cystoides intestinalis: confirmation of diagnosis by endoscopic puncture a review of pathogenesis, associated disease and therapy and a new theory of cyst formation. Endoscopy. 1998; (30)9: 793 -799. • Koss LG. “Abdominal gas cysts (penumatosis cystoides intestinorum hominis): an analysis with a report of a case and a critical review of the literature. ” Arch Pathol. 1952; (53): 523 -549. • Pear BL. “Pneumatosis intestinalis: a review. ” Radiology. 1998; 207(1): 1319. • Pieterse AS, Leong AS, Rowland R. “The mucosal changes and pathogenesis of pneumatosis cystoides intestinalis. Hum Pathol 1985; 16: 683. • Wayne E, Ough M, Wu A et al. “Management algorithm for pneumatosis intestinalis and portal venous gas: treatment and outcome of 88 consecutive cases. ” J Gastrointest Surg 2010; 14: 437.

Thank you!

Additional slides
 with rim of histiocytes, multinuclear giant cells, lymphocytes,")
Histology • Histology: pseudocysts (no epithelium) with rim of histiocytes, multinuclear giant cells, lymphocytes, neutrophils, eosinophils, granulomas, fibrosis
- Slides: 49