GI Grand Rounds Johanna Chan Gastroenterology Fellow Baylor

GI Grand Rounds Johanna Chan Gastroenterology Fellow Baylor College of Medicine 3/21/13

No conflicts of interest No financial disclosures

HPI • RFC: hematemesis, melena • 67 yo East Asian F p/w 4 -5 days of burning epigastric pain, black emesis, melena • Presented to ER with dizziness, lightheadedness, fatigue • No prior similar episodes, no NSAIDs, no Et. OH, no known H. pylori, no risk factors for chronic liver disease • No other associated symptoms, weight changes

Past Medical History • HTN • Previously on medication, now diet controlled

Medications • None • No OTC medications, including NSAIDs

Other history • Family history ▫ Mother and father died “of old age” ▫ Siblings alive and healthy ▫ No GI malignancy • Social history ▫ ▫ Denies all Et. OH Lifelong nonsmoker No IV drug use or other illicits Married, housewife

Exam • • • T 98. 5, BP 121/62, HR 83, RR 12, O 2 sat 99% RA 4’ 11”, 100 lbs Gen: NAD, AAOx 4, conversational HEENT: PERRL, EOMI, MMM, OP clear Neck: supple, no LAD CV: RRR 2/6 SEM RUSB Lungs: CTAB Abd: S/NT, NABS, slightly distended Ext: WWP no c/c/e Rectal: no blood, no stool in rectal vault

Labs 136 101 23 131 4. 1 26 0. 6 6. 9 7. 9 25. 9 69% PMNs Total protein 7. 3 Albumin 3. 8 Total bili 0. 4 ALT 26 AST 29 Alk phos 90 368 INR 1. 2 PTT 28 MCV 91

Endoscopy

Endoscopy

Endoscopy

Pathology • • Stomach antrum, biopsy Adenocarcinoma, signet ring cell type Focally invasive in muscular wall of stomach HER-2 negative

 •")
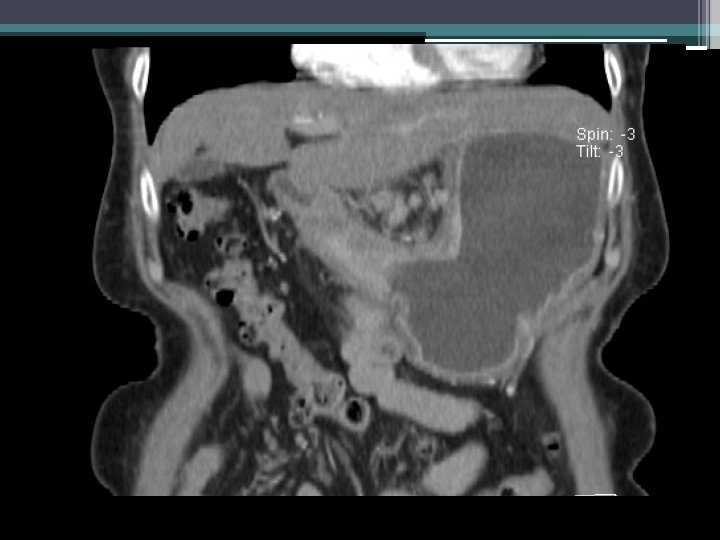
Imaging • Pyloric/antral mass (2. 7 x 2. 9 x 1. 8 cm) • Distention of proximal stomach • Nonspecific lymph nodes (largest 7 mm) adjacent to lesser curve of stomach • No significant pulmonary findings • ? nonspecific liver hypodensities • ? nodularity of omentum

Clinical course • • No further hematemesis nor melena Unable to tolerate even clear liquid diet TPN initiated Tumor board discussion ▫ MRI liver to evaluate for metastases (negative) ▫ Diagnostic laparoscopy to evaluate for peritoneal disease (pending) ▫ Pending laparoscopy findings, further plans?

Management of malignant gastric outlet obstruction

Clinical questions • What are methods for palliation of malignant gastric outlet obstruction? ▫ Open gastrojejunostomy ▫ Laparoscopic gastrojejunostomy ▫ Endoscopic stenting • What is the role for gastrojejunostomy versus stent for palliation of malignant gastric outlet obstruction?

Gastrojejunostomy • Historical/traditional treatment for malignant gastric outlet obstruction • 72% of patients with good functional outcome and relief of symptoms • 13 -55% morbidity

Open versus laparoscopic GJ • 3/1998 to 1/2000: 78 GJ procedures (45 OGJ, 33 LGJ) • 68 patients had advanced gastric cancer undergoing palliative GJ (38 OGJ, 30 LGJ) • 10 case matched controls (age, gender, ASA class, prior abdominal surgery) • Assessed operating time, time to PO intake, use of pain medication, morbidity, mortality, WBC, ESR, IL-6, TNF alpha • Laparoscopic GJ group had lower inflammatory markers, morbidity, earlier recovery of bowel function Choi YB. Surg Endosc. 2002. 16(11): 1620 -6.

Open versus laparoscopic GJ • 24 patients with inoperable neoplasm of distal stomach, duodenum, or biliary tract ▫ Malignant metastatic or locally advanced unresectable • Randomized prospectively to undergo LGJ or OGJ, followed for 2 months • Age, gender, ASA class, primary tumor location, and mean duration of surgery not significantly different • LGJ significantly less blood loss and shorter time to PO intake compared with OGJ • Post-op stay shorter with LGJ (not statistically significant, 11 vs. 12 days) Navarra G et al. Surg Endosc 2006 20(12): 1831 -4.

Stents

Stents for malignant GOO • 1 st case report for self-expanding metallic stent for gastric outlet obstruction published in 1992 • Common complications include recurrence of GOO symptoms due to stent obstruction (food, tumor in-/overgrowth), stent migration, perforation, biliary obstruction • Nitinol: nickel-titanium shape-memory alloy, soft, flexible, smoother wire ends • Uncovered versus covered Boskoski I et al. Adv Ther 2010 27(10): 691 -703. Dormann A et al. Endoscopy. 2004; 36: 543 -550. Mauro MA et al. Radiology 2000; 215: 659 -69.

Stents for malignant GOO • Systematic review in 2004 on >600 cases shows reported technical success rate 97%, with clinical success 87% • Overall reported technical success rate 93 -97%, clinical success rate 84 -93% • Stents with >20 mm diameter should permit passage of solid food Dormann A et al. Endoscopy. 2004; 36: 543 -550. Van Hooft JE et al. Gastrointest Endosc. 2009 69(6): 1059 -66.
: includes 2")
Stenting versus gastrojejunostomy • Systematic review (10 studies between 1/1990 to 5/2008): includes 2 RCTs • 514 total patient outcomes (244 stents, 218 OGJ) • 30 day follow up • Endoscopic stenting more likely to result in earlier PO intake (7 days), shorter hospital stay (12 days) • Comparable periprocedural complication rate (15 -16%) ▫ OGJ more major complications (AKI, MI, PNA) ▫ ES usually technical complications requiring repeat intervention Ly J et al. Surg Endosc 2010 24(2): 290 -7.

Stenting versus gastrojejunostomy • Systematic review, 44 publications between 1/1996 and 12/2005 • Includes same 2 RCTs (18 patients, 27 patients) • No difference in early and late major complications (though high variability) • More rapid food intake and relief of obstructive symptoms after stent • Recurrent obstructive symptoms more common after stent (food obstruction, tumor in-/overgrowth) • Stent may have more favorable short-term results; GJ may be a better option in patients with longer survival Jeurnink SM et al. BMC Gastroenterol. 2007; 7: 18.

Stenting versus gastrojejunostomy • SUSTENT: multicenter randomized trial • 21 centers in the Netherlands, 1/2006 -5/2008 • 18 patients randomized to GJ, 21 patients to Enteral Wallflex stent • Compared GOO scoring system, early and late major complications, minor complications, persistent obstructive symptoms (>4 weeks), HRQo. L, and costs Jeurnink SM et al. Gastrointest Endosc 2010. 71(3): 490 -9.

GOO Scoring System • • • 0 = no oral intake 1 = liquids only 2 = soft solids 3 = almost complete diet 4 = full diet Adler DG, Baron TH. Am J Gastroenterol. 2002; 97: 72 -78.
: 490 -9.")
Jeurnink SM et al. Gastrointest Endosc 2010. 71(3): 490 -9.
: 490 -9.")
Jeurnink SM et al. Gastrointest Endosc 2010. 71(3): 490 -9.

SUSTENT • Stent placement: more rapid PO intake, shorter hospital stay, lower costs • GJ with longer follow-up (>2 months): better food intake, fewer major complications, and fewer recurrent obstructive symptoms and reinterventions • Recommend GJ as primary treatment if expected survival > 2 months • Recommend stent if expected survival < 2 months Jeurnink SM et al. Gastrointest Endosc 2010. 71(3): 490 -9.

Take home points • Several options for palliation of malignant gastric outlet obstruction • Treatment decisions often complicated by poor nutritional status, advanced underlying disease • Consider expected patient survival in management decisions

References • Boskoski I et al. Self-expandable metallic stents for malignant gastric outlet obstruction. Adv Ther 2010 27(10): 691 -703. • Brimhall B and Adler DG. Enteral stents for malignant gastric outlet obstruction. Gastrointest Endosc Clin N Am. 2011 21(3): 389 -403. • Canena JM et al. Oral intake throughout the patients’ lives after palliative metallic stent placement for malignant gastroduodenal obstruction: a retrospective multicentre study. Eur J Gastroenterol Hepatol. 2012 24(7): 747 -55. • Choi YB. Laparoscopic gastrojejunostomy for palliation of gastric outlet obstruction in unresectable gastric cancer. Surg Endosc. 2002 16(11): 16206. • Dormann A et al. Self-expanding metal stents for gastroduodenal malignancies: systematic review of their clinical effectiveness. Endoscopy. 2004; 36: 543 -550. • Jeurnink SM et al. Stent versus gastrojejunostomy for the palliation of gastric outlet obstruction: a systematic review. BMC Gastroenterol. 2007; 7: 18.
 • Jeurnink SM et al. Surgical gastrojejunostomy or endoscopic stent placement for")
References (con’t) • Jeurnink SM et al. Surgical gastrojejunostomy or endoscopic stent placement for the palliation of malignant gastric outlet obstruction (SUSTENT study): a multicenter randomized trial. Gastrointest Endosc 2010. 71(3): 490 -9. • Ly J et al. A systematic review of methods to palliate malignant gastric outlet obstruction. Surg Endosc 2010 24(2): 290 -7. • Mauro MA et al. Advances in gastrointestinal intervention: the treatment of gastroduodenal and colorectal obstructions with metallic stents. Radiology 2000; 215: 659 -69. • Mehta S et al. Prospective randomized trial of laparoscopic gastrojejunostomy versus duodenal stenting for malignant gastric outlet obstruction. Surg Endosc. 2006 20(2): 239 -42. • Mendelsohn RB et al. Carcinomatosis is not a contraindication to enteral stenting in selected patients with malignant gastric outlet obstruction. Gastrointest Endosc. 2011 73(6): 1135 -40. • Miller BH et al. An assessment of radiologically inserted transoral and transgastric gastroduodenal stents to treat malignant gastric outlet obstruction. Cardiovasc Intervent Radiol. 2013 Mar 2 (epub ahead of print).
. • Navarra G et al. Palliative antecolic isoperistaltic gastrojejunostomy: a randomized controlled")
References (con’t). • Navarra G et al. Palliative antecolic isoperistaltic gastrojejunostomy: a randomized controlled trial comparing open and laparoscopic approaches. Surg Endosc 2006 20(12): 1831 -4. • Roy A et al. Stenting versus gastrojejunostomy for management of malignant gastric outlet obstruction: comparison of clinical outcomes and costs. Surg Endosc 2012 26(11): 3114 -9. • Van Hooft JE, et al. Efficacy and safety of the new Wall. Flex enteral stent in palliative treatment of malignant gastric outlet obstruction (DUOFLEX study): a prospective multicenter study. Gastrointest Endosc. 2009 69(6): 1059 -66.

Questions?
- Slides: 37