Gettin Digi Wit it Digoxin Overdose Core Rounds











 • CVS – (Palpitations, Syncope,")





























")






, he doper than Dre •")
- Slides: 58
Gettin’ Digi Wit it Digoxin Overdose Core Rounds March 6, 2003 A. F. Chad, MD, CCFP Randall Berlin, MD
The Fresh Prince • After years of getting jiggy, Will Smith develops CHF and is Rx Digoxin • He presents to the FHH feeling “not jiggy” • What should you do?
Wild West • Digoxin is a cardiac glycoside from Foxglove plant – Other cardiac glycosides from oleander, foxglove, and lily-of-the-valley • Used in ancient Roman as cardiac med • Physicians first studied 18 th C • Digoxin toxicity 1 st described in 1785
Gettin’ Jiggy • Inotropic effects via inhibition Na/K ATPase pump -> incr myocardial Ca -> more forceful contraction • Increases automaticity in atrial and ventricular tissue • Slows conduction through AV node (via parasympathomimetic tone)
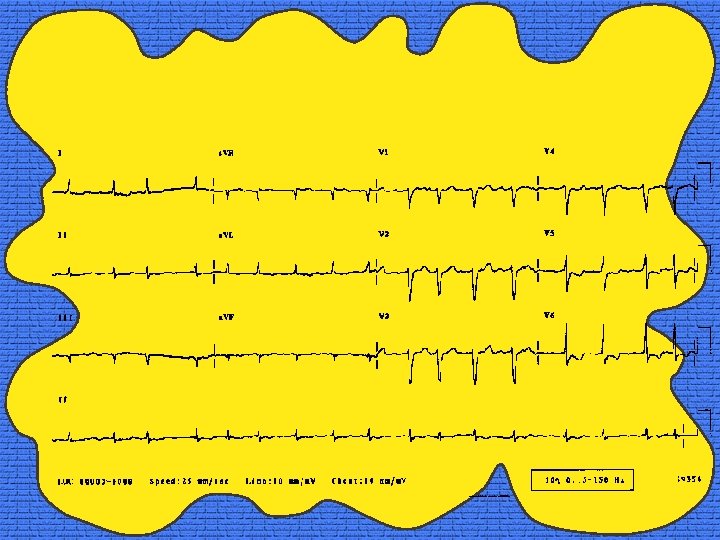
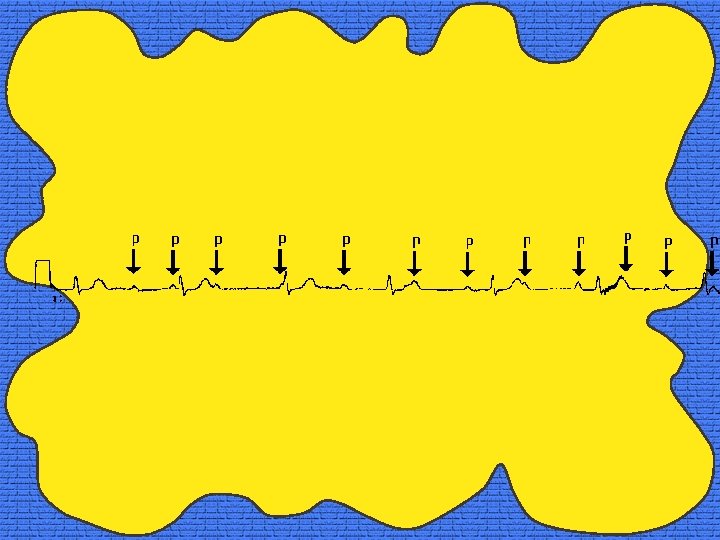
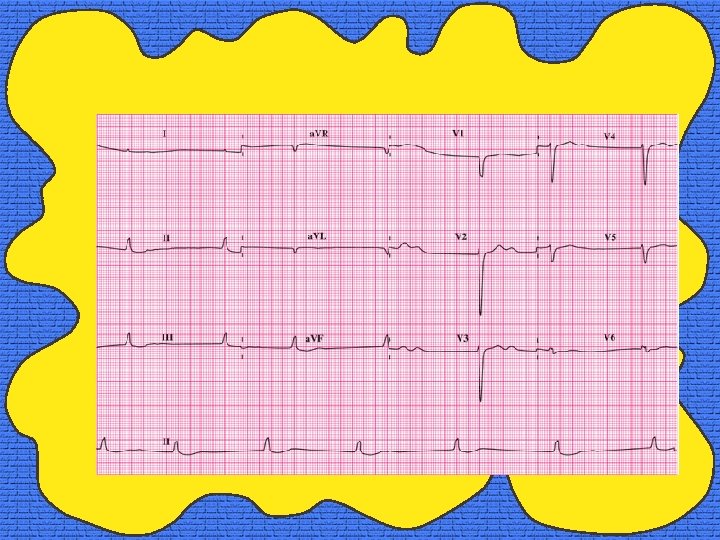
Gettin’ Jiggy : ECG Effects • • Downward scooping of ST segment Inverted T waves Reduced T wave amplitude Short QT interval U waves Prolonged PR interval Does NOT affect QRS duration
Gettin’ Jiggy • Onset 5 -30 mins IV, peak 1 -4 hrs • Onset 30 -120 mins po, peak 2 -6 hrs • “N” levels = 0. 6 -2. 6 nmol/L, most reliable 6 hrs post ingestion • Narrow therapeutic window • Large Vd (5. 6 L/Kg) • Crosses BBB, placenta • Hepatic degredation (15%), excreted in urine (85%) • T 1/2= 30 -40 hrs (4 -6 d in RF)
So Fresh • USA: – 0. 4% hospital admissions – 1. 1% of outpatients on digoxin – 10 -18% nursing home patients • Internationally: – 2. 1% of inpatients on digoxin – 0. 3% of admissions
Yes, Y’all: ? Not that common? • Williamson, KM, et al. Digoxin Toxicity: An Evaluation in Current Clinical Practice. Arch Intern Med. 1998; 158: 2444 -2449 • 5 hospitals, dig levels taken in 3434, 2009 >2. 6 nmol/L, only 83 (4. 1%) clinical tox, 16% had levels < 6 hrs
Men in Black • Morbidity = 4. 6 -10% • 50% if digoxin level > 7. 7 nmol/L
Not So Fresh Prince • Will Smith: “ My breathin’ is ill G, I gots me some palpitations, my guts be groovin’ like DJ Jazzy Jeff, and I be seein’ yellowgreen, like them aliens in Men in Black. ” • Does this sound like he’s digi wit’ it?
Nod Ya Head • Constitutional symptoms – (weakness, fatigue) • CVS – (Palpitations, Syncope, Dyspnea) • CNS – (Confusion and somnolence, Dizziness w/o vertigo, Agitation, delirium, hallucinations, h/a, Paresthesias, neuropathic pain, Seizures (extremely rare)
Nod Ya Head • Ocular – (Disturbances color vision with tendency to yellow-green , Blurring, diplopia, Halos, scotomas, Photophobia) • GI – (N&V&D, anorexia, Abdo pain (uncommon))
Nod Ya Head • Acute – Mainly Cardiac ad GI • Chronic – Can have any of the Symptoms
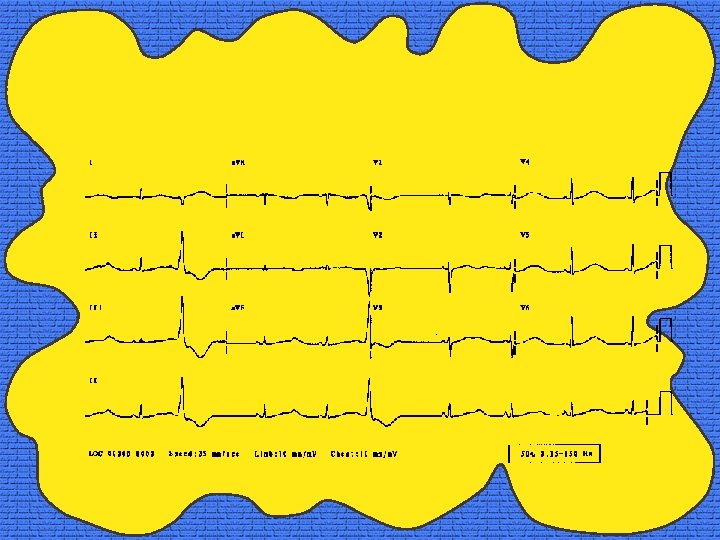
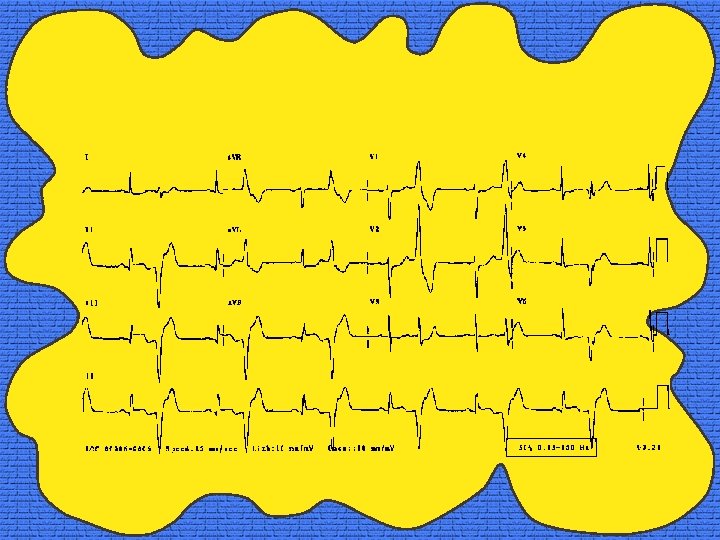
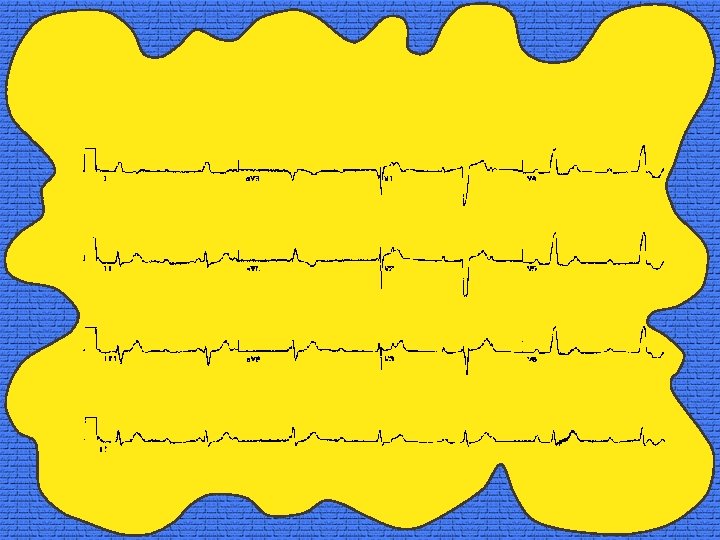
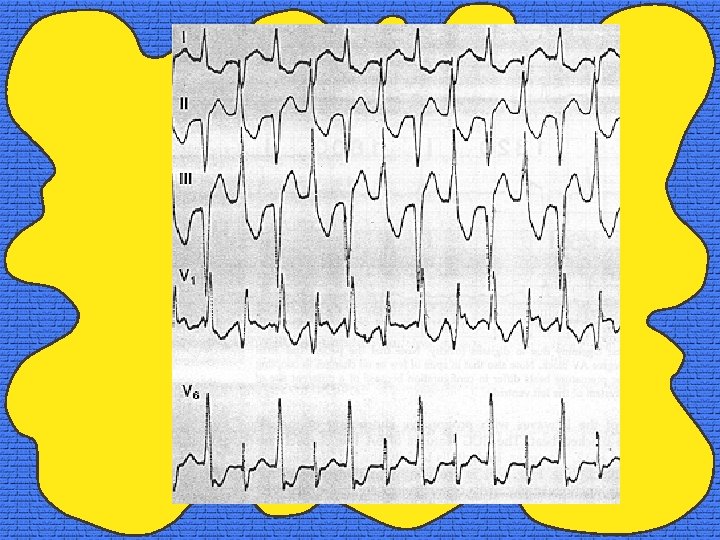
Big Willie Style • ANY arrhythmia • Classically: paroxysmal atrial tachycardia + 2: 1 block, accelerated jnc, bidirectional VT, Td. P • Typically: combo of increased ectopy or automaticity with block • Acute or healthy heart more typical to have bradyarrhythmias and blocks • Chronic or diseased hearts: enhanced automaticity + impaired conduction
Big Willie Style • Hemodynamic instability -> arrhythmia or CHF • PVCs most common arrhythmia • Sinus brad & bradyarrhythmias very common: Slow a. fib with little variation in ventricular rate (regularization of the R-R interval) • Heart block • Rapid a. fib or flutter is rare • VT • Cardiac arrest from asystole or VF usually fatal
Big Willie Style • GI symptoms common, abdo exam nonspecific. • Neurological findings related to changes in sensorium or mental status – Lateralizing findings usually indicate another disease process. • Visual changes occur, pupils are spared, objective findings few • Drug-induced fever does not occur
Not So Fresh Prince • Will Smith: “Dr Dre, my beat physician put me on lasix, spironolactone, ibuprofen, amiodarone, and propafenone. ” • “Is tryin’ to do me like Biggie? ”
Y’all Know • Drug interactions most common cause • directly increase plasma levels, alter renal excretion, induce electrolyte abnormalities. • • • Amiloride Amiodarone Calcium channel blockers Propafenone Quinidine Quinine Indomethacin Spironolactone Hydrochlorothiazide Other loop diuretics Triamterene Amphotericin B
Y’all Know • Hypokalemia, hypernatremia increase the toxic CVS effects of digoxin re: effects on NA+/K+ ATPase pump. – Digoxin toxicity does not cause hypokalemia, but hypokalemia can worsen digoxin toxicity. – Hyperkalemia is usual lyte abnormality ppt by digoxin toxicity, esp acute
Y’all Know • Hypomagnesemia – increases myocardial digoxin uptake and decreases cellular Na. K ATPase activity – makes correcting hypokalemia very difficult • Acidosis depresses Na+/K+ ATPase pump and may cause digoxin toxicity • Dehydration
Y’all Know • Ischemia suppresses Na+/K+ ATPase pump and independently alters automaticity • Hypothyroid re decreased renal excretion, smaller volume of distribution. • Bioavailability varies depending on formulation – Toxicity may occur by increasing bioavailability.
Y’all Know • Deteriorating renal function, dehydration, lytes, ischemia precipitate chronic toxicity. • Acute overdose or accidental exposure to plants containing cardiac glycosides may cause acute toxicity.
Y’all Know • Complex interaction between digoxin and various lyte & renal abnormalities • normal digoxin levels (0. 6 -2. 6 nmol/L) & renal insufficiency or severe hypokalemia may have more serious cardiotoxicity than patient with high digoxin levels and no renal or electrolyte disturbances
Not So Fresh Prince • Will Smith: “If y’all help me out, I’ll put yo on my next album … you can bust rhymes with me & Puffy. ” • After a Mic check, What tests should you do?
Tests for the Willenium • Digoxin level • Electrolytes, Mg, Ca, Renal Fnc tests • ECG • CXR • ? Echo • ? Cath
Tests for the Willenium • Acute toxicity, repeat the dig level q 2 -4 hours • Levels do not necessarily correlate with toxicity, esp acute ingestion. • Acutely digoxin levels do not equilibrate quickly re variable absorption and tissue distribution.
Tests for the Willenium • Toxicity related to intracellular levels, not serum • Digoxin level drawn <4 hrs of acute ingestion may be incredibly high with no apparent toxicity. • Rx guided by digoxin level and serum K+ and patient's clinical and ECG
Not So Fresh Prince #1 • Big Willie all of a sudden becomes less jiggy and hypotensive • Monitor shows a bradysrhythmia • Now What? • Should I pace him (to the beat of Wild West)?
Not So Fresh Prince #2 • Big Willie all of a sudden becomes less jiggy and hypotensive, • Monitor shows a tachydysrhythmia • Now What? • Should I cardiovert him (like a glock to the chest)?
Not So Fresh Prince #3 • Big Willie all of a sudden becomes less jiggy and hypotensive, • Monitor shows peaked T’s, widened QRS. • K+ comes back @ 7 mmol/L • Should I give him Ca++?
Not So Fresh Prince #4 • Big Willie all of a sudden becomes less jiggy and hypotensive • Your Rx to date have done nothing (including your attempt at rappin’ Parents Just Don’t Understand) • Is there anything else you could use?
Just the two of Us • • • ABCD!!!! IV’s, Monitors Consider AC & Lavage if acute Anti-arrhythmics Lyte Abn Digibind
Black Suits Coming: CVS • ANY Arrhythmia!!! • Unstable = digibind • Brady = atropine, ? pacing (lowers Fib threshold)?
Black Suits Coming: CVS • Stable VT / Ventricular arrhythmias – digibind, dilantin, lido, Mg, avoid cardioversion – Lido, dilantin 1 st line antiarrhythmic, case / dog studies, decrease ventricular ectopy w/o slowing nodal activity • Unstable VT or VF – digibind + cardioversion, defibrillate vfib • Do not cardiovert SVTs
Black Suits Coming: CVS • Ca++ = BAD – increase: dig effects? , contractions? , tetany? • Cardioversion / defib relatively contraindicated re ventricular ectopy -> “safe if not toxic” – Ditchey RV, Curtis GP. Effects of apparently nontoxic doses of digoxin on ventricular ectopy after directcurrent electrical shocks in dogs. J Pharmacol Exp Ther 1981 Jul; 218(1): 212 -6. – Ditchey RV, Karliner JS. Safety of electrical cardioversion in patients without digitalis toxicity. Ann Intern Med. 1981 Dec; 95(6): 676 -9. – N=21
Black Suits Coming: Pacing? • Taboulet, P, et al. Acute Digitalis Intoxication - Is pacing Still Appropriate? Clin Tox, 31(2), 261 -273 (1993). • ? No? • N=92 • 41 Rx Lavage, AC, +/- atropine -> all survived • 51 Rx, as above, but pace vs FAB vs both • 23 paced, 12 FAB, 16 both • 9 / 39 paced -> 7 VF, 2 VA 2 to pacer use (7 prior to FAB), also infxn, pacer malfnc • 3 / 28 FAB -> 2 in VF / VA prior -> died, one died later of VF 100 hrs later
Will 2 K+ • Usual Rx • Insulin + glucose, B 2 ags, Kayexelate, Na. HCO 3 / correct acidosis, dialysis • Avoid Ca++ -> ppt ventricular dysrrhythmias • Caution with digibind if using other means to correct hyperkalemia prior to digibind Rx-> will result in markedly decreased K+!!!
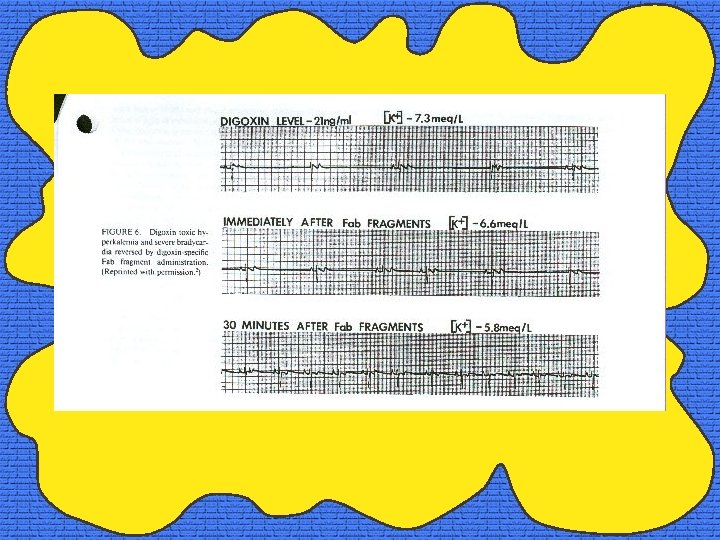
Block Party: When Digibind • Arrhythmias associated with hemodynamic instability • Altered LOC attributed to digoxin toxicity • Hyperkalemia K+ > 5 m. Eq/L • Digoxin level > 10 nmol/L in adults at steady state (ie, 6 -8 h postingestion) • Ingestion > 10 mg in adults (40 X 0. 25 mg tablets) or > 0. 3 mg/kg in children • Hypotension not responsive to fluids
Block Party: Digibind • • Digoxin-FAB fragments From Ig. G of Sheep Excreted renally Each vial contains 40 mg Each Vial binds 0. 5 mg digoxin $4121 Cn for 10 vials accute, 5 chronic
Block Party: Digibind • Chronic toxicity: number of vials = digoxin level (ng/m. L) X weight (kg)/100 • Acute overdose: number of vials = total amount ingested (mg) X 0. 8 / 0. 5 • Give IV over 30 mins • Effect by then, peak in 4 hrs • Check levels in 4 -6 hrs – Levels post digibind will be markedly elevated and are uninterpretable unless you are able to get free digoxin levels
Block Party: Digibind • Saluk, S et al. Treatment of severe digitalis intoxication with digoxin-specific antibody fragments: A clinical review. Crit Care Med June 1988; 16, 6: 629 -635. • 20 papers, N=255, mainly case reports • FAB is GREAT and safe!
Block Party: Digibind • Hickey, et al. Digoxin-Specific FAB, Expanded Data on Safety. JACC Vol 17, No. 3, March 1, 1991: 590 -8. • N=717, form filled out if FAB used, F/U form post Rx • 357 responded, 172 partially, 89 none • No response usually incorrect Dx or inadequate dosing • No deaths attributed to FAB, 6 allergic responses
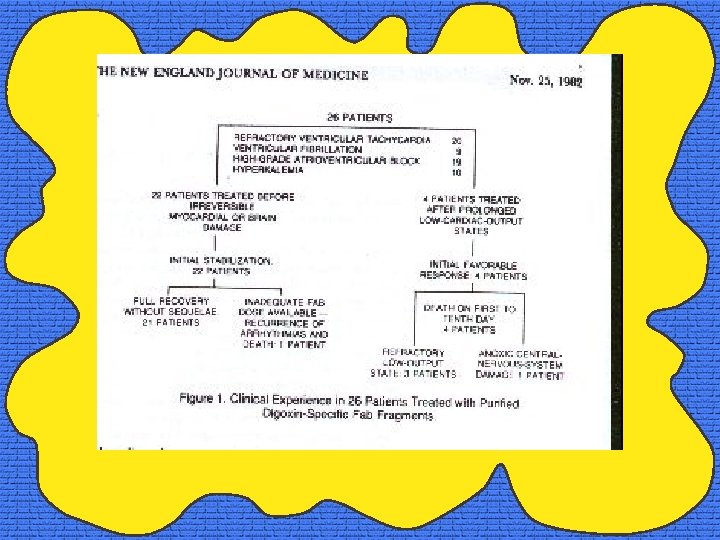
Block Party: Digibind • Smith, TW, et al. Treatment of lifethreatening digitalis intoxication with digoxin-specific Fab antibody fragments: experience in 26 cases. NEJM. 1982, 307: 1357 -1361.
Block Party: Digibind • Antman EM, et al. Treatment of 150 cases of life-threatening digitalis intoxication with digoxin-specific Fab antibody fragments: final report of a multicentre trial. Circulation 1990; 81: 1744 -1752.
Block Party: Digibind • N=150 • 75 long term, 15 accidental, 59 suicidal, 1 fetal • 148 responses documented, 80% resolved, 10% improved, 10% no response • Median time to response = 19 mins, 75% response <60 mins • 14 adverse effects (hypo. K, CHF) • Poor / non-response-> CAD, wrong Dx, inadequate dose, pts moribund
Miami • • ABCD’s Monitors, IV’s Lytes, dig level, ECG If toxic: – Supportive Rx – Rx hyperkalemia – Rx Digibind FAB if unstable
Residents DO just Understand! • Thanks to Dr Ber(lin), he doper than Dre • You, for keepin’ it real • My hommies back in tha projects in East Saskatoon • Biggie & Tupac • Peace Out