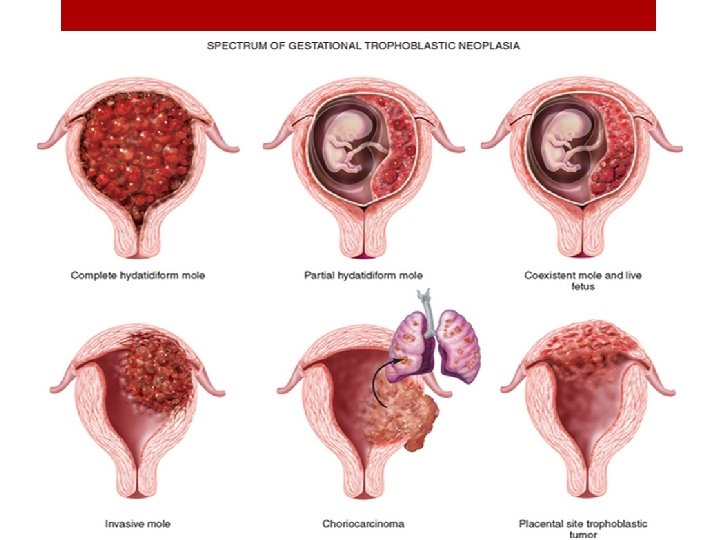
Gestational Trophoblastic Disease GTD Partial molar pregnancy BY
 Partial molar pregnancy BY: Mohammad Al-Momani")
Gestational Trophoblastic Disease (GTD) Partial molar pregnancy BY: Mohammad Al-Momani

1 -Origin 2 - Histologic features 3 -Clinical features 4 -malignant potential 5 -Diagnosis 6 -management 7 -follow up 8 -future fertilization

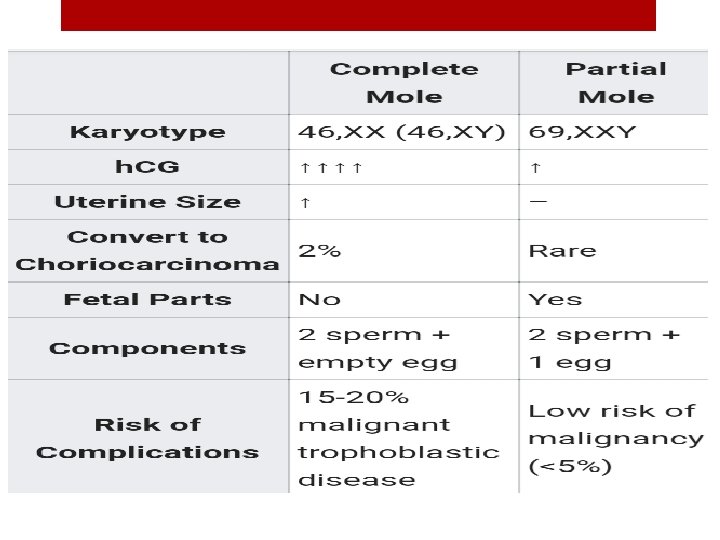
1 -Origin: is a normal ovum that is fertilized by two sperm. The resulting karyotype is 69, XXX, 69, XXY, or 69, XYY. A fetus, umbilical cord and amniotic fluid is seen which results ultimately in fetal demise(not viable)
 other villa")
2 - Histologic features : v Varying-sized villi, only some focal hydropic(edema) other villa are essentially normal “appearing grossly as grapelike structures” v Focal trophoblastic (cytotrophoblast) proliferation v. Presence of fetal tissue and vessels

. 3 -Clinical features : 1. Abnormal uterine bleeding is the most common presenting symptom in the first trimester of a pregnancy, similar to complete moles. 2. Excessive vaginal bleeding, hyperemesis, preeclampsia, hyperthyroidism, and ovarian cysts are rare. 3. As the cytotrophoblast does NOT produce h. CG , h. CG levels in partial mole will be NORMAL (or slightly elevated) 4. Many spontaneous abortions around the late first to early second trimester may represent undiagnosed partial moles. 4 - Malignant potential : • Less than 5% of partial moles progress to malignant disease.

5 -Diagnosis: 1. The exam is typically unremarkable (the only thing you can see is small uterus for dates So typically those women think they are pregnant then fetal demise occur ) 2. Quantitative h. CG: normal for pregnancy 3. Pelvic US may reveal fetus with abnormalities , or simply a gestational sac 4. Genetic analysis 5. Low aminotic fluid 6. Enlarged placenta with "swiss cheese " appearance FROM hydropic chorionic villi

Difference from the complete molar pregnance
 -Dilation and curettage of the uterus")
6 -Management of molar pregnancies (complete and partial) -Dilation and curettage of the uterus under GA and U/S guidance: is the primary tool for evacuating a molar pregnancy even when the uterus has enlarged beyond the size expected for a pregnancy of 20 weeks. Pre-op tests : CBC , PTT , TFT(no need in partial), Cross match should be available • Danger include : haemorrhage , sepsis , air embolism , incomplete evacuation and perforation of the uterus • Second aspiration or curettage may be needed two weeks later to ensure complete evacuation of the uterus. • Complete mole have 20% risk of becoming invasive and 2% risk of developing into choriocarcinoma. v Therefore, complete evacuation of the uterus is the mainstay of therapy -intravenous oxytocin should be given to enhance uterine contractionand minimize blood loss. -Hysterectomy is a treatment option for patients who do not desire future fertility. -contraception should be used until h. CG normalizes WHY? • (to make sure that any rise in the hcg is from an ivasive disease not from pregnancy)
 : • Prophylactic chemotherapy is not indicated in patients with molar")
-Chemotherapy( METHOTREXATE ) : • Prophylactic chemotherapy is not indicated in patients with molar pregnancy because 90% of these individuals have spontaneous remissions. • Indicated if : • Β-HCG values do not decrease. • Histological features of malignant GTD are present. • If metastasis are present on CXR ü Most patients with molar pregnancies are cured with evacuation and do not require any therapy. ü Some require transfusion, however, because of excessive blood loss. ü Abnormal clotting parameters should be treated with fresh frozen plasma and platelet transfusions, as indicated. ü Rarely, a patient can experience acute respiratory distress from trophoblastic embolization or fluid overload. Such patients may require respiratory support via a ventilator and careful cardiopulmonary monitoring

7 -Follow-up of a complete or partial molar pregnancy Follow-up of a molar pregnancy should include: 1 - Obtain quantitative h. CG titer 48 hrs P/O 2 - Serial h. CG weekly until levels are normal for 3 consrcutive weeks 3 - After h. CG levels normalized , serial h. CG monthly for 6 months, and then yearly. After evacuation, the expected average time to complete elimination of h. CG is 12 to 16 weeks • Pregnancy can be attempted after 6 to 12 months from the diagnosis, if there is no evidence of GTT requiring further treatment.

8 -Future fertility 1. Normal pregnancy is the most likely result of future gestations. 2. Risk of a second molar pregnancy is 1%. in the case of two sequential molar pregnancies, the risk of a third molar pregnancy is 33%. Subsequent molar pregnancies may be complete or partial, regardless of the type of initial molar pregnancy
- Slides: 13