GESTATIONAL TROPHOBLASTIC DISEASE Done by Alaa khreisat q

GESTATIONAL TROPHOBLASTIC DISEASE Done by: Ala'a khreisat

q. Trophoblast are cells forming the outer layer of a blastocyst, which provide nutrients to the embryo and develop into a large part of the placenta. qproliferates and differentiates into 2 cell layers: qcytotrophoblast & syncytiotrophoblast (which implant into uterus , come into contact with maternal blood and form chorionic villi and secrete h. CG ) üHCG : a hormone produced by the placenta after implantation It helps in secreting progesterone and sustain pregnancy h. CG-positive indicates an implanted blastocyst and mammalian embryogenesis
 INCLUDE : 1. HYDATIDIFORM MOLES (BOTH COMPLETE AND")
• GESTATIONAL TROPHOBLASTIC DISEASES (GTD) INCLUDE : 1. HYDATIDIFORM MOLES (BOTH COMPLETE AND PARTIAL) 2. INVASIVE MOLES 3. CHORIOCARCINOMA
 with GTD have a benign course. v.")
v. The majority of patients (80 -90%) with GTD have a benign course. v. This diverse group of diseases has a sensitive tumor marker, human chorionic gonadotropin (h. CG), that allows accurate follow-up and assessment of the diseases.

HYDATIDIFORM MOLE • BENIGN TROPHOBLASTIC DISEASE • CLASSIFIED AS COMPLETE OR PARTIAL MOLES üMOLAR PREGNANCY IS AN ABNORMAL FORM OF PREGNANCY IN WHICH A NON-VIABLE FERTILIZED EGG IMPLANTS IN THE UTERUS AND WILL FAIL TO COME TO TERM • Most molar pregnancies are sporadic, but a familial syndrome of recurrent hydatidiform mole has been described and is reported to be strongly associated with a mutation in the NLRP 7 gene.

Risk factors for hyatidiform mole ØPrevious molar pregnancy The risk of the development of a second molar pregnancy is 1 -3%, or as much as 40 times greater than the risk of developing the first molar pregnancy. ØHigh or low maternal age(<20 or >40) result from defective fertilizationa process that is more common in both younger and older individuals. ØAsian origin ØDiet may play a causative role. The incidence of molar pregnancy has been noted to be higher in geographic areas where people consume less β-carotene (a retinoid) and folic acid.

COMPLETE MOLE The majority of hydatidiform moles are “complete” moles Serum h. CG is excessively high with complete moles Pathogenesis Enucleate ovum +normal sperm which replicates it self Rarely : Enucleate ovum +2 sperms • FETAL KARYOTYPES • 46 XX: MORE COMMON (∼ 90% OF CASES) • 46 XY: LESS COMMON (∼ 10% OF CASES) • 46 YY KARYOTYPE HAS NEVER BEEN OBSERVED BECAUSE IT IS NONVIABLE.
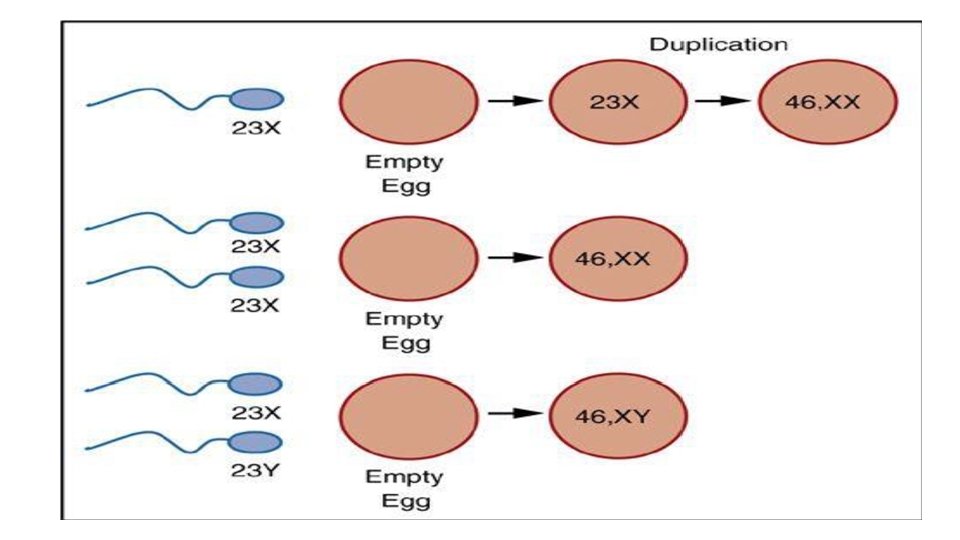

COMPLETE MOLE IS THE RESULT OF PATERNAL DISOMY( A GENOTYPIC ANOMALY IN WHICH AN INDIVIDUAL RECEIVES TWO COPIES OF ONE CHROMOSOME FROM A SINGLE PARENT AND NO COPIES FROM THE OTHER)
 of choronic villi hydropic degeneration---->grape-like vesicls")
Patholgy üplacental abnormality severe hyperplasia of trophoblasts hydropic(swollen) of choronic villi hydropic degeneration---->grape-like vesicls filling uterus THE ACCUMULATION OF WATER IN CELLS IN RESPONSE TO INJURY. IMPAIRED NA+/K+-ATPASE PUMP FUNCTION (E. G. , DUE TO HYPOXIA) DECREASES ATP PRODUCTION, WHICH LEADS TO NA+ ACCUMULATION IN THE CELL. üAbsent fetus tissue üAbnormal proliferation of syncytotrophoblast---->High h. CG levels (>100, 000 ml. U/ml) Large theca cysts >6 cm Hyperthyrodism Hyperemesis gravidarum Early pre-eclampsia ü 15 -20% progress to malignancy

Symptoms • VAGINAL BLEEDING(irregular or heavy vaginal bleeding during the first or early second trimester of pregnancy. The bleeding is usually painless, although it can be associated with uterine contractions) • UTERUS SIZE GREATER THAN NORMAL FOR GESTATIONAL AGE • PASSAGE OF VESICLES THAT MAY RESEMBLE A BUNCH OF GRAPES THROUGH THE VAGINA • ENDOCRINE SYMPTOMS. . NERVOSNESS TREMORS DUE TO HYPERTHYROIDISIM(VERY HIGH AMOUNTS OF ΒHCG MAY LEAD TO HYPERTHYROIDISMBECAUSE Β-HCG STRUCTURALLY RESEMBLES TSH. ITS THYROTROPIC ACTIVITY) • PREECLAMPSIA (IRRITABILITY DIZZZINESS AND PHOTOPHOBIA) (BEFORE THE 20 TH WEEK OF GESTATION) ü PREECLAMPSIA TENDS TO HAPPEN 2 ND AND 3 RD TRIMESTER NOT IN 1 ST TRIMESTER. SO IF THE SIGNS OCCUR IN 1 ST TRIMESTER THINK ABOUT MOLAR PREGNANCY. • HYPEREMESIS GRAVIDARUM (A CONDITION OF SEVERE, PERSISTENT NAUSEA AND VOMITING DURING PREGNANCY THAT IS ASSOCIATED WITH > 5% LOSS OF PRE-PREGNANCY WEIGHT AND SEVERE DEHYDRATION. MORE COMMON AMONG YOUNG, PRIMIGRAVID WOMEN AND WOMEN WITH MULTIFETAL GESTATION OR MOLAR PREGNANCY. ) The typical clinical presentation of complete molar pregnancies has changed with the advent of high-resolution

• OVARIAN THECA LUTEIN CYSTS: BILATERAL, LARGE, CYSTIC, ADNEXAL MASSES THAT ARE TENDER TO THE TOUCH (A TYPE OF FUNCTIONAL OVARIAN CYST THAT IS THOUGHT TO ORIGINATE FROM EXCESSIVE AMOUNTS OF CIRCULATING GONADOTROPINS SUCH AS Β-HCG. TYPICALLY MULTIPLE AND SEEN BILATERALLY, WITH A HIGH ASSOCIATION WITH GESTATIONAL TROPHOBLASTIC DISEASE AND MULTIPLE GESTATIONS. USG SHOWS BILATERAL ENLARGED, MULTILOCULAR, CYSTIC MASSES OF THE OVARIES. USUALLY RESOLVE SPONTANEOUSLY ONCE THE SOURCE OF BETA-HCG IS REMOVED)
, WHICH SHOULD REVEAL")
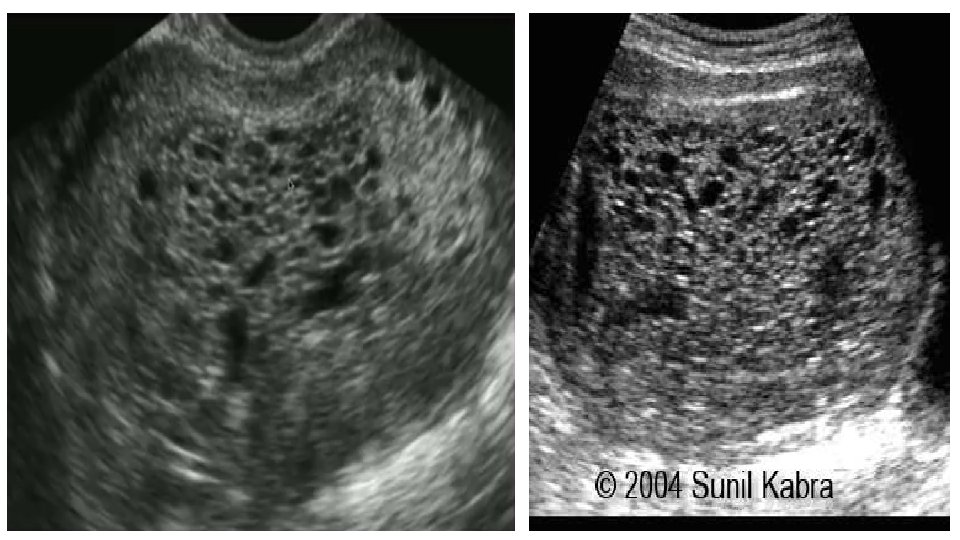
DIAGNOSTICS • LABORATORY TESTS: Β-HCG LEVEL MEASUREMENT (INITIAL TEST OF CHOICE), WHICH SHOULD REVEAL Β-HCG THAT IS MARKEDLY ELEVATED(HIGHER THAN EXPECTED FOR THE GESTATIONAL AGE) • TRANSVAGINAL ULTRASOUND • COMPLETE HYDATIDIFORM MOLE • THECA LUTEIN CYSTS • ‘ Snowstorm’ =SWISS CHEESE=BUNCH OF GRAPES appearance of mixed echogenecity, representing hydropic villi and intrauterine haemorrhage. • NO AMNIOTIC FLUID • LACK OF FETAL HEART TONES • NOTE: SOME MOLES MAY NOT PRODUCE HCG AT ALL!
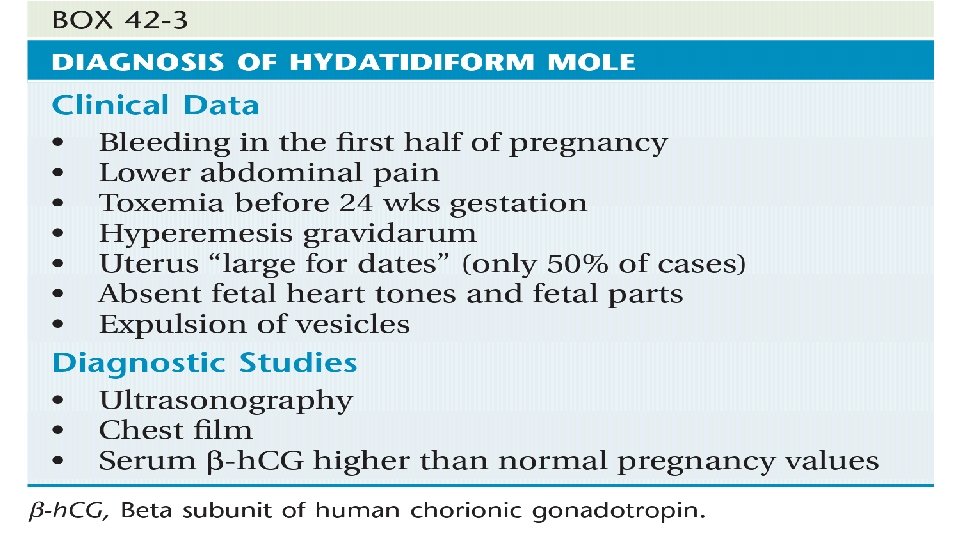

CLINICAL INVESTIGATIONS Patients who have the presumptive or definitive diagnosis of hydatidiform mole should have a complete blood count done to exclude anemia, which might require a transfusion. They require an assessment of platelet count, prothrombin time, partial thromboplastin time, and fibrinogen level, because an occasional patient may experience disseminated intravascular coagulation. Liver and renal function tests should be performed. Blood should be typed and cross-matched in the event that excessive bleeding is encountered at the time of evacuation of the mole. A chest film should be obtained, as should an electrocardiogram if tachycardia is present or if the patient is older than 40 years of age

TREATMENT üEvacuation. . . The standard therapy for hydatidiform mole is suction evacuation followed by DILATION AND SUCTION CURETTAGE(D&C) of the uterine cavity, regardless of the duration of pregnancy. This should be performed in the operating. Pre-op tests : CBC , PTT , TFT. Cross match should be available. üoxytocin is given simultaneously to help stimulate uterine contractions and reduce blood loss. This technique is associated with a low incidence of uterine perforation and trophoblastic embolization. üMonitoring Levels of the β-Subunit of Human Chorionic Gonadotropin Following the evacuation of a hydatidiform mole, the patient must be monitored with weekly serum assays of β-h. CG until three consecutive levels have been normal. Monthly β-h. CG levels should then be followed until three consecutive levels have been normal. Following the evacuation, the β-h. CG levels should steadily decline to undetectable levels, usually within 12 to 16 weeks. üChemotherapy(METHOTREXATE) Prophylactic chemotherapy is not indicated in patients with molar pregnancy, because 90% of these individuals have spontaneous remissions. INDICATED BY ANY OF THE FOLLOWING: • Β-HCG VALUES DO NOT DECREASE. • HISTOLOGICAL FEATURES OF MALIGNANT GTD ARE PRESENT. • IF METASTASES ARE PRESENT ON CHEST X-RAY.

ØMost patients have an uncomplicated course in the immediate postoperative period. Ø Some require transfusion, however, because of excessive blood loss. ØAbnormal clotting parameters should be treated with fresh frozen plasma and platelet transfusions, as indicated. Ø Rarely, a patient can experience acute respiratory distress from trophoblastic embolization or fluid overload. Such patients may require respiratory support via a ventilator and careful cardiopulmonary monitoring.

ü COMPLETE MOLES HAVE A 20% RISK OF BECOMING INVASIVE AND A 2% RISK OF DEVELOPING INTO CHORIOCARCINOMA. THEREFORE, COMPLETE EVACUATION OF THE UTERINE CAVITY IS THE MAINSTAY OF TREATMENT. PROGNOSIS • MOST PATIENTS ACHIEVE NORMAL REPRODUCTIVE FUNCTION AFTER RECOVERY.
- Slides: 19