Geriatric syndromes D Greyling Geriatric syndromes 1 Frailty





: 1. Acute onset and fluctuating course")






 3. Psychiatric")
















- Slides: 31
Geriatric syndromes D. Greyling
Geriatric syndromes • • • 1. Frailty 2. Delirium 3. Falls 4. Sleep disorders 5. Dizziness 6. Syncope 7. Pressure sores 8. Incontinence 9. Elder mistreatment 10. Dementia 11. Parkinson's
Frailty • A clinical syndrome of increased vulnerability and decreased ability to maintain homeostasis that is age related and centrally characterized by decline in functional reserves across multiple physiological systems
Frailty • Suspect if : • 1. Unintentional weight loss of more than 4, 5 kg in the past year • 2. Feeling exhausted • 3. Weakness ( Poor grip strength ) • 4. Slow walking speed • 5. Low physical activity
Frailty • Associated with a high risk of falls, dependency disability, institutionalization, hospitalization, risk of iatrogenesis and side effects of medical interventions and death. • Frailty is part of a single or multiple clinical syndromes
Delirium • • • CAM( Confusion Assessment Method): 1. Acute onset and fluctuating course 2. Inattention 3. Disorganized thinking 4. Altered level of consciousness: From lethargic, stupor to coma.
Clinical • • • History: Precipitating factors Ask and determine: 1. Level of consciousness 2. Orientation 3. Memory 4. Attention 5. Perceptual problems : delusions 6. Pschycomotor behavior 7. Sleep –wake cycle
Precipitating factors • D – Drugs • I – Infections • M- Metabolic ( electolytes, glucose, acid base) • T- Toxins • O – Oxygen deficiency • P – Psychiatric ( Bereavement, Emotional stress)
Falls • 35 - 40 % of persons over 65 fall in a given year and increases with age. • • • Risk factors for falls: 1. Muscle weakness 2. Gait Deficit 3. Balance deficit 4. Use of assistive device 5. Visual deficit 6. Impaired Daily Activity of living 7. Cognitive impairment 8. Age more than 80
Assessment • • • 1. History 2. Medications 3. Vision 4. Gait and Balance : Standing on one leg for 5 sec Bending 5. Lower limb joints 6. Neurological 7. Cardiovascular: Orthostatic hypotension Pulse rate and rhythm
Sleep disorders • 50 % of elderly persons complain of sleep difficulty • • 1. Sleep disordered breathing Hypopneas or apneas during sleep • 2. Restless legs syndrome : Cluster of repeated leg jerks every 20 – 40 seconds during sleep • • 3. Circadian rhythm sleep disorders: Sleep wake cycle - sleepy early in the evening and waking up early • 4. Insomnia : low quantity and or quality of sleep • • 5. Rapid eye movement sleep behavior disorders : A dissociated state during which complex motoric behaviors occur
Dizziness • A broad term to describe various abnormal sensations arising from perceptions of the bodies relationship to space and of unsteadiness. • Older than 65 years 10 % in crease for every 5 years
Causes 1. Vestibular causes 2. Central nervous system causes( TIA / Stroke) 3. Psychiatric disorders( Depression/ Anxiety) 4. Cervical spine( Vertebral artery occlusion) 5. Systemic causes( DM, HT, CAD, Low Hb, Hypothyroidism, CCF) • 6. Orthostatic hypotension • 7. Post prandial hypotension • 8 Drugs • • •
Syncope • Rapid onset of transient loss of consciousness and spontaneous complete recovery • Caused by blunted baroreceptor sensitivity
Evaluation • Three questions: • 1. ? Loss of consciousness attributable to the syncope(Trauma, Epilepsy , Vascular, Conversion) • 2. ? Heart disease • 3. Are there important clinical features that suggest the etiology ?
Syncope examination • • Orthostatic hypotension Use of devices for mobilty Vision 5 item recall Gait Balance Neuromuscular: Quadriceps strenght Rigidity, Tremor, Bradikinesai
Pressure ulcers • Areas of local tissue trauma developing where soft tissue are compressed between bony prominences and any external surface for long periods of time. • Most common : Sacrum, Ischial tuberosities , throchanters and heels
Stage 1 • Skin intact with redness over a bony prominence
Stage 2 : Loss of the dermis with a shallow ulcer
Stage 3: Full tissue loss
Stage 4: Full thickness with exposed tendon/muscle/bone
Incontinence Any involuntary leakage of urine. “DRIIIPP” D – Delirium R- Restricted mobility I – Infection ( UTI) , Inflammation ( Atrophic vaginitis), Impaction of feaces • P- Pharmaceuticals • • •
Types of incontinence • Stress: Loss of urine with increase of intra – abdominal pressure • Urge : Inability to delay voiding after sensation of bladder fullness is perceived • Mixed: Combination of above • Overflow: Due to mechanical forces on an over distended bladder( Urinary retention/ Abnormal bladder and sphincter function)
Elderly mistreatment • The willful infliction of pain, injury or causing mental anguish to an elder person. • Very common – Physical abuse • Neglect • Financial or material abuse • Psychological and verbal abuse • Violation of a trusting relationship
Risk factors for elderly abuse • • Disability Cognitive impairment Abusers likely to abuse alcohol/drugs Abuser dependency Living arrangement External stress Social isolation History of violence of the abuser
Dementia
Dementia • Progressive cognitive and behavioral deficits accompanied by structural abnormalities of the brain. • DSM IV criteria: • 1. Memory impairment • 2. One of the following disturbances: • - Language disturbance • -Impaired ability to carry out motoric activities • - Failure to identify objects • - Disturbance in executive functioning • 3. Significant impairment in social and occupational functioning • 4. Do not occur during the course of delirium
Mild cognitive impairment • • Memory complaint Memory impairment for age and education Preserved general cognitive function Intact social and occupational function
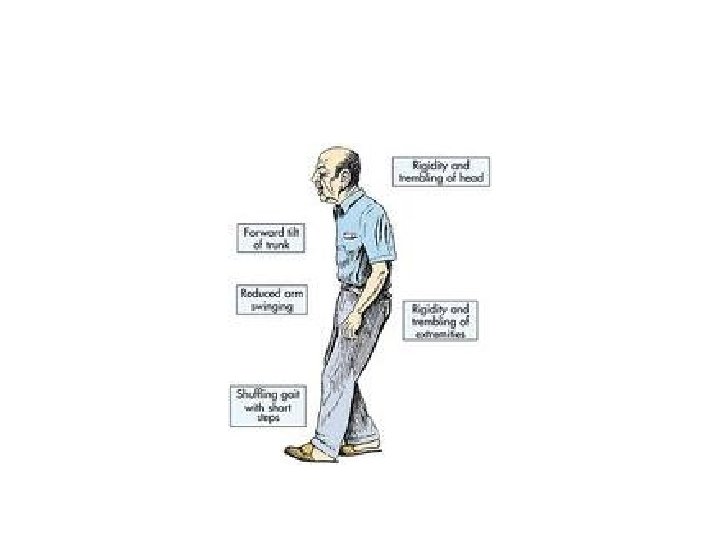
Parkinson’s Disease • Any combination of six independent motoric features: • 1. Rest tremor • 2. Bradykinesia • 3. Rigidity • 4. Loss of postural reflexes • 5. Flexed posture • 6. Freezing phenomenon( Feet glued to the ground)