GEORGIA TQIP STATE COLLABORATIVE DATA VALIDATION PROJECT Amy

GEORGIA TQIP STATE COLLABORATIVE DATA VALIDATION PROJECT Amy Svestka, BA, EMT, CSTR Program Manager, TQIP Data Quality American College of Surgeons, Committee on Trauma

GA Collaborative Data Validation…

Site Selection • Random selection • Excluded centers who had already undergone a data validation visit within the last 3 -years.

What is a Data Validation Site Visit? • Patient List • All Deaths with a length of stay of 15 days or fewer. • Patients with an ISS greater than 24, no major complications, and a length of stay of at least 1, but not more than 30 days • Patients with a length of stay between 15 and 30 days with no major complications or death • Patients 64 years of age or more, no co-morbidities, and a length of stay of 15 or fewer days • Patients on the mechanical ventilator for more than 7 days who had a length of stay of 30 or fewer days and no pneumonia • Patients who survived with a GCS motor score of 1, no major complications, and a length of stay between 3 and 30 days. • TQIP Data Abstraction • Comparison Review • The comparison review is for educational purposes. • Recommendations

Agenda…

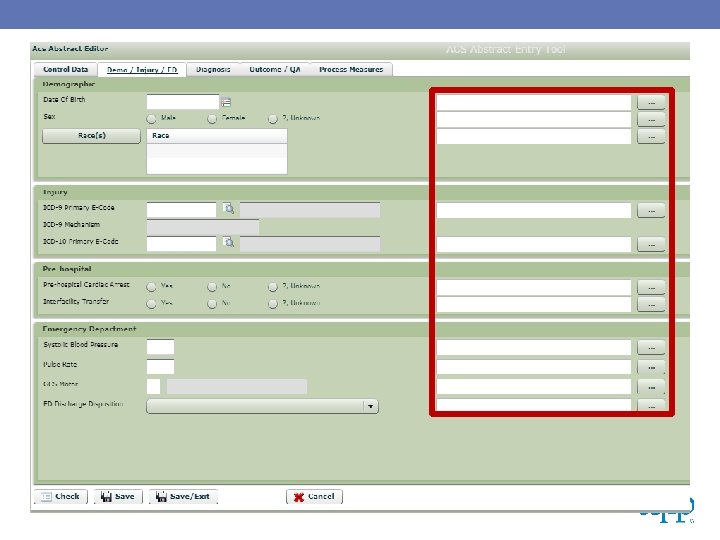
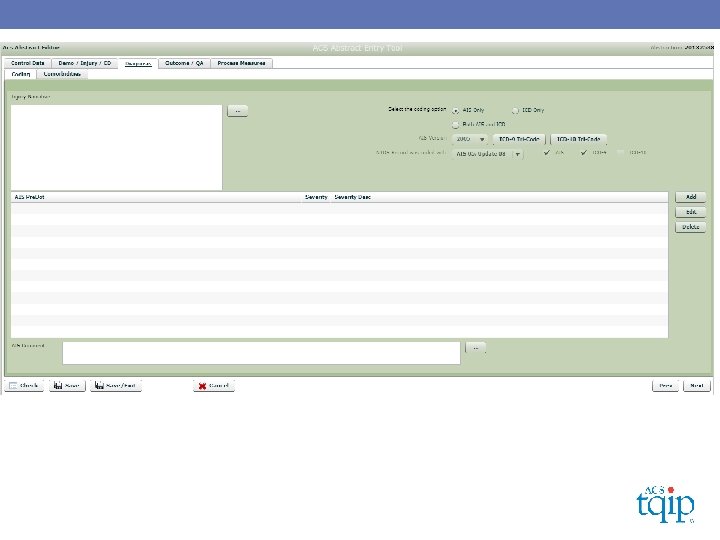
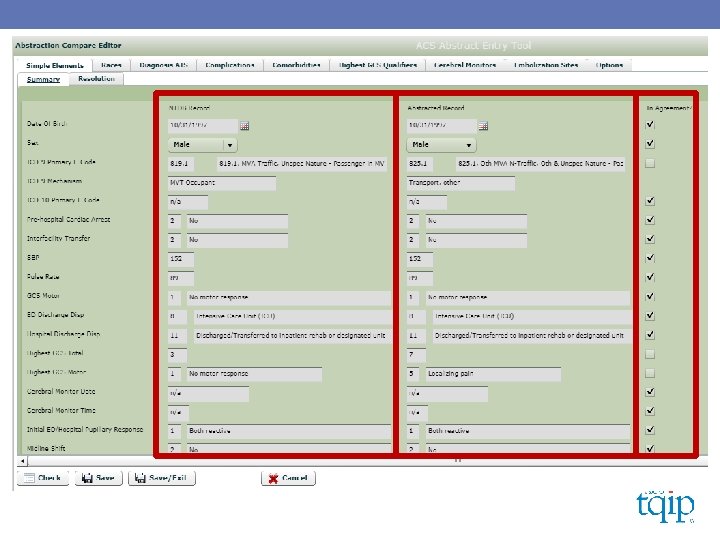
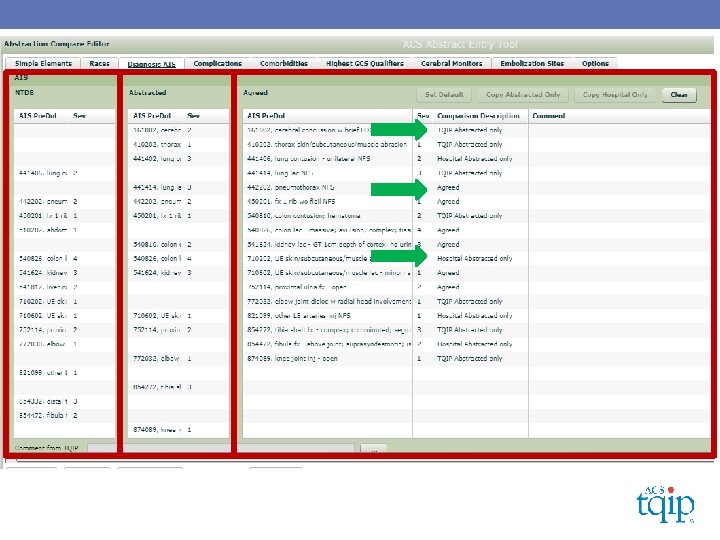
TQIP Data Validation Tool…

DATA VALIDATION FINDINGS

Results… • Average scores • 90 -100% overall average • 80 -89% overall average • Below 80% overall average • Submission Frequency Report • Education • Staffing

90 -100% Overall Average • • • • • Date of Birth Gender Race ICD-10 Primary External Cause Code Inter-Facility Transfer Pre-Hospital Cardiac Arrest Initial ED/Hospital SBP Initial ED/Hospital Pulse Initial ED/Hospital GCS Motor ED Discharge Disposition Hospital Discharge Disposition Cerebral Monitor Date Cerebral Monitor Time VTE Prophylaxis Type VTE Prophylaxis Date Transfusion Blood (4 Hours) Transfusion Blood (24 Hours) Transfusion Blood Measurement Transfusion Blood Conversion • • • • • Transfusion Plasma (4 Hours) Transfusion Plasma Measurement Transfusion Plasma Conversion Transfusion Platelets (4 Hours) Transfusion Platelets (24 Hours) Transfusion Platelets Measurement Transfusion Platelets Conversion Cryoprecipitate (4 Hours) Cryoprecipitate (24 Hours) Angiography Embolization Site Angiography Date Angiography Time Surgery for Hemorrhage Control Type Surgery for Hemorrhage Control Date Surgery for Hemorrhage Control Time Withdrawal of Care Date Withdrawal of Care Time

80 -89% Overall Average • Highest GCS Motor • GCS Assessment Qualifier of Highest GCS Total • Midline Shift • Cerebral Monitor • Transfusion Plasma (24 Hours) • Cryoprecipitate Conversion

Below 80% overall Average • Co-Morbid Conditions • AIS Injury Codes • Hospital Complications • Highest GCS Total • Initial ED/Hospital Pupillary Response • VTE Prophylaxis Time • Lowest ED/Hospital SBP

Co-Morbid Conditions • Provides a baseline heath status of the patient • Risk-adjusted benchmarking • Average Score 62. 96%

Co-Morbid Conditions Findings… • “Not Applicable” was reported when patient’s past medical history was unknown • “Not Known/Not Recorded” was reported when patient’s had no NTDS comorbidities • Definitions were not being followed • Co-Morbid Condition were reported when the criteria was not met • Co-Morbid Conditions were not reported when the criteria was met

AIS Injury Codes • TQIP Patient Inclusion Criteria • Risk-Adjusted Cohorts • Severe TBI • Isolated Hip Fracture • Non Risk-Adjusted Cohorts • Fracture • Mid-shaft Femur Fracture • Open Tibia Shaft Fracture • Blunt Splenic Injury Average Score 53. 44% • Important for modeling • Highest AIS by body region • Survival Risk Ratio

AIS 2005 Abbreviated injury Scale 2005 Update 2008

AIS Findings… • Missed injuries • External Injuries • Cerebral Concussion • Lung laceration • Pericardium hemopericardium • Torn “Vein of Labbe” • Injuries coded incorrectly • Large SDH reported (25). Documentation supported SDH NFS (9) • Minor concussion reported (3). Documentation supported DAI (12) • Single SDH NFS reported (9). Documentation supported small bilateral SDH (12) • Simple open radius fracture reported (6). Documentation supported comminuted open radius shaft fracture (9)

Importance of Hospital Complications… • TQIP Benchmark Report • Highlights areas of opportunity, as well as areas of excellence • Excessive missingness could lead to exclusion from risk-adjusted complications models • Under reporting will lead to inappropriate labeling of high performance • Over reporting will lead to inappropriate labeling of low performance • Average Score 70%

Hospital Complications Findings… • Missing Hospital Complications • Not Applicable was reported when there was documentation of reportable complications in the patient’s medical record • Cardiac arrest with CPR • Unplanned return to the OR • Definitions were not being followed • Hospital Complications were reported when the criteria was not met • Hospital Complications were not reported when the criteria was met

Importance of Highest GCS – Total… • Used in the Severe TBI Cohort • Average Score 65%

Highest GCS – Total Findings… • Collection Criterion • Missed injuries • Concussion • The definition was not followed • Highest documented score within 24 hours

Importance of Initial ED/Hospital Pupillary Response • Future - Severe TBI Cohort • Average Score 65%

Initial ED/Hospital Pupillary Response Findings • Collection Criterion • Missed injuries • Concussion • The definition was not followed • Physiological response of the pupil size within 30 minutes or less of ED/hospital arrival

Importance of VTE Prophylaxis Time • TQIP Benchmark Report VTE Prophylaxis cohort • Average Score 75%

VTE Prophylaxis Time Findings • The time reported was the time ordered, not the time administered

Importance of Lowest ED/Hospital SBP • TQIP Benchmark Report “Shock” cohort • Initial ED/Hospital SBP between 0 and 90 mm. Hg • Average Score 75%

Lowest ED/Hospital SBP Findings • Definition was not being followed • Lowest sustained (>5 min) systolic blood pressure measured within the first hour of ED/hospital arrival • Incorrect values were reported

SUBMISSION FREQUENCY REPORT FINDINGS

Submission Frequency Report… • Provides frequency tables for each NTDB data variable • Provides an opportunity for centers to see what their data looks like when it is received by the NTDB • Catches mapping problems • Data Validation

Submission Frequency Report Findings • “Not Applicable” was reported in data fields where ALL patients apply. • Weight • Initial ED/Hospital SBP • Inconsistencies between related data variables • Surgery for Hemorrhage Control Type vs. Surgery for Hemorrhage Control Date/Time • Clinical sense of associated Co-Morbid Conditions • 120 patients reported with “COPD” vs. 16 patients reported with “Steroid Use”

Causes of data discrepancies • Human error • Documentation issues • Mapping problems • Abstractor not following or understanding a data field definitions

STAFFING

Staffing… 97 NTDS variables vs. 310 average variables 75% understaffed Resources for Optimal Care of the Injured Patient aka. The Orange Book, Chapter 15 • One full-time equivalent employee dedicated to the registry must be available to process the data capturing the NTDS data set for each 500– 750 admitted patients annually (CD 15– 9). • This staffing need increases if additional data elements are collected. • Hospitals must also take into account the additional tasks, above the abstraction and entry of patient data, that are assigned to the registrar. Processes such as report generation, data analysis, research assistance, and meeting various submission requirements will decrease the time dedicated to the meticulous collection of patient data. • Electronic downloads into the trauma registry also create additional tasks, as does ongoing data validation prior to data acceptance. • Additional staff will be required to perform these tasks to ensure the integrity and quality of registry data that are used for prevention, PIPS, and other essential aspects of the trauma program.

EDUCATION

Education… • The trauma registrar is a vital member trauma team. of the Resources for Optimal Care of the Injured Patient aka. The Orange Book, Chapter 15 • Ideally, the trauma registrar works directly with the trauma team and reports to the trauma program manager. • Trauma registrars should receive initial training when they start the job. • They must attend or have previously attended two courses within 12 months of being hired: (1) the American Trauma Society’s Trauma Registrar Course or equivalent provided by a state trauma program and (2) the Association of the Advancement of Automotive Medicine’s Injury Scaling Course (CD 15– 7).

Education… • A certifying examination is available through the sponsorship of the American Trauma Society’s Registrar Certification Board, leading to the designation of certified specialist in trauma registries (CSTR) or equivalent. • Registrars should complete a minimum of 8 hours of registry- specific continuing education per year. • The trauma registrar must demonstrate proficiency with the NTDS. • Centers are encouraged to support trauma registrar training by providing educational offerings within the facility. For example, a lecture regarding organ injuries is appropriate training for registrars, because they are expected to code organ injuries, as well as the procedures performed to treat the injuries.

TQIP Education… • Monthly Educational Experiences • One center has not participated • Monthly Webinars • One center has not participated • TQIP Online Course • 50% completed the 2017 course

? ? ? QUESTIONS ? ? ?

- Slides: 44