Genus BRUCELLA Universities Press India Private Limited Universities
 Private Limited Universities Press")
Genus BRUCELLA © Universities Press (India) Private Limited Universities Press

Case 1 • 6 -yr male child, New Delhi, was admitted with complaints of fever & dry cough for 5 days, headache and vomiting for 1 day. • He also had two episodes of epistaxis. His oral acceptance was reduced. • Fever was high grade, remittent in nature and a not associated with chills. • There was no history of joint pain or swelling, pain abdomen, diarrhea or skin rashes. The child was not receiving any antibiotics. • There was history of travelling to a hill station in northern India two months prior to the onset of illness. There was history of consumption of dairy products made from unpasteurized cow milk. • No other family member had similar illness. © Universities Press (India) Private Limited Universities Press

• On examination child was conscious, well oriented, afebrile with cool extremities, pulse rate was 144/min, low volume, blood pressure was 96/50 mm. Hg, respiratory rate was 26/min • There was no pallor, icterus, lymphadenopathy or skin rashes. • He had hepatomegaly of 3. 0 cm below costal margin in midclavicular line and splenomegaly of 1. 5 cm. There was no abdominal distension or tenderness, no free fluid and bowel sounds were normal. • Respiratory and cardiovascular systems were normal clinically. • There were no neurological deficit or meningeal signs and fundus examination was also normal. © Universities Press (India) Private Limited Universities Press

• At admission hemoglobin was 11. 2 g/dl, TLC was 3600/cu mm with neutrophils 56%, band forms 9%, platelets 1. 30 × 105/cu mm, SGPT (ALT) 254 IU and SGOT (AST) 196 IU • Patient was started on ceftriaxone and intravenous fluid resuscitation following which peripheral perfusion and BP improved. • Blood culture was sterile after 72 hours of incubation © Universities Press (India) Private Limited Universities Press

• On day 4 of admission, child developed generalized abdominal pain with severe nausea and vomiting. • There was generalized abdominal distension with diffuse tenderness. • CT scan abdomen showed hepato-spleenomegaly with a single, non enhancing, hypo dense lesion in the spleen © Universities Press (India) Private Limited Universities Press

• On day 5 of admission, child was drowsy, sleeping excessively but easily arousable and had headache. • Child was also noticed to have developed tender, discreet lymphnodes in submental, submandibular and posterior triangle on both sides of the neck • CT scan of thorax showed bilaterial pleural effusion with basal atelectasis of lower lobe • Agglutination test for Brucella was done on day 10 of admission and was reported positive for B. abortus (1: 160). © Universities Press (India) Private Limited Universities Press

• Child was treated with oral cotrimoxazole for 6 weeks and intravenous gentamicin for 2 weeks. • He became aferbrile within 48 hours and abdominal symptoms and lymphadeno-pathy disappeared within 72 hours of starting therapy and was discharged after 2 weeks of stay in the hospital to complete the treatment at home. • Follow up CT scan abdomen done after completion of therapy showed resolution of splenic hypodensity. • The child remained afebrile without any evidence of arthritis or arthralgia and hepatosplenomegaly during six months follow-up. © Universities Press (India) Private Limited Universities Press

Case 2 • A 24 -year-old male was admitted with history of fever for 3 months. • There was history of insidious onset, progressive weakness of both lower limbs proximal more than distal in the form of not being able to stand from squatting, climbing up, and getting down stairs for the last 2 months. • Simultaneously, he noticed proximal weakness in both upper limbs in the form of inability to lift heavy objects as he used to previously. • Patient also gave history of difficulty in walking for the same duration © Universities Press (India) Private Limited Universities Press

• History of increased frequency of micturition accompanied with urgency and precipitancy was present for the last month. • In addition patient had developed impairment in hearing for the last month. • Patient belonged to a rural area and was associated with livestock rearing. He used to consume raw milk of goat. (This history was disclosed retrospectively. ) • On examination patient was febrile. Rest of the general physical examination was normal. © Universities Press (India) Private Limited Universities Press

• On nervous system examination, patient was conscious Examination of cranial nerves revealed bilateral sensory neural deafness. • Gait was spastic. • Rest of the neurological examination was normal. Review of other systemic examinations was normal. On investigations hemoglobin was 11. 6 gm% and total leukocyte count was 7200/cmm. • Peripheral smear revealed a microcytic hypochromic picture. © Universities Press (India) Private Limited Universities Press

• CSF analysis had proteins: 273 mg/d. L; glucose: 29 mg/d. L (concomitant blood glucose: 10 Blood sample was positive for RBT. • SAT was positive in 1 : 640 titers. • Subsequently brain MRI was done. white matter hyperintensities involving frontal lobes) with involvement of subcortical fibres at places were observed. © Universities Press (India) Private Limited Universities Press

• Patient was prescribed doxycycline 100 mg twice a day, rifampicin 600 mg once a day, and cotrimoxazole (160 mg trimethoprim and 800 mg sulfamethoxazole) twice a day. • Patient became afebrile on fourth day of treatment. • All three drugs were continued for three months. • At the end of three months patient remained afebrile, deafness recovered, and bladder dysfunction and spastic gait improved. He had resumed his routine work © Universities Press (India) Private Limited Universities Press

GRAM NEGATIVE COCCOBACILLI • • • BORDETELLA BRUCELLA YERSENIA PASTEURELLA FRANCESELLA • HAEMOPHILUS, MORAXELLA, GARDENERELLA • HACEK © Universities Press (India) Private Limited Universities Press

Many Names of Brucellosis Human Disease • Malta Fever • Undulant Fever • Mediterranean Fever © Universities Press (India) Private Limited Universities Press

Jeffery Allen Marston • Contracted Malta fever. • Described his own case in great detail. © Universities Press (India) Private Limited Universities Press
 • British Army physician and microbiologist • Discovered Micrococcus")
Sir David Bruce (1855 -1931) • British Army physician and microbiologist • Discovered Micrococcus melitensis (July 9, 1887) © Universities Press (India) Private Limited Universities Press
 • Danish physician and veterinarian • Discovered Bacterium abortus (1897)")
Bernhard Bang (1848 -1932) • Danish physician and veterinarian • Discovered Bacterium abortus (1897) could infect cattle, horses, sheep and goats. © Universities Press (India) Private Limited Universities Press

BRUCELLA • • • B. melitensis – humans – goat’s milk B. abortus – abortion in cattle B. suis – pigs B. canis – canine abortion B. ovis – abortion in sheep © Universities Press (India) Private Limited Universities Press

Morphological Profile Brucella spp. are small, Gram-negative, non-motile, non-spore-forming, coccobacilli. Intracellular microbes causing chronic disease. © Universities Press (India) Private Limited Universities Press

CULTURE • Aerobes • B. abortus and B. ovis capnophilic 5– 10% CO 2 • Optimum temperature – 37°C • Ph, 6. 6– 7. 4 • Nutrient agar – slow growth, colony – small, moist, translucent and glistening © Universities Press (India) Private Limited Universities Press

Cultural characters • Aerobe. Best medium is Trypticase Soya Agar with selective agents (Polymyxin, Cyclohexamide). Small, moist, translucent and glistening colonies after 3 or more days of incubation. © Universities Press (India) Private Limited Universities Press

CULTURE • Serum dextrose agar – 0. 5– 1 mm, low convex, circular, smooth, transparent colonies • Selective medium – serum dextrose agar, with antibiotics – bacitracin, cycloheximide, nalidixic acid, nystatin, polymyxin B, vancomycin © Universities Press (India) Private Limited Universities Press

CLASSIFICATION • 6 species – based – CO 2 requirement, H 2 S production, urease, growth – 1 in 50, 000 basic fuchsin and thionine agglutination/monospecific sera – B. melitensis; 3 biotypes • B. abortus – 7 biotypes • B. suis – 5 biotypes © Universities Press (India) Private Limited Universities Press

Biochemical reactions Catalase and Oxidase positive. Nitrates are reduced. Rapidly positive for urease. Negative for IMVi. C reactions. Susceptibility n n n Killed at 600 C in 10 minutes Pasteurization of milk. Survival is long in refrigerated milk, ice creams and cheese. © Universities Press (India) Private Limited Universities Press

Transmission to Humans • Conjunctiva or broken skin on contact with infected tissues in farmers, dairy workers, veterinarians – Blood, urine, vaginal discharges, aborted fetuses, placentas • Ingestion – Raw milk & unpasteurized dairy products (Cheese) – Rarely through undercooked meat © Universities Press (India) Private Limited Universities Press

Transmission to Humans • Inhalation of infectious aerosols – Pens, stables, slaughter houses • Inoculation with vaccines – B. abortus strain 19, RB-51 – B. melitensis Rev-1 – Conjunctival splashes, injection • Person-to-person transmission is rare • Incubation varies – 5 days to three months © Universities Press (India) Private Limited Universities Press

Transmission to Humans • In laboratory – accidental ingestion, inhalation, injection and mucosal/skin © Universities Press (India) Private Limited Universities Press

Transmission in Animals • Ingestion / contact with infected tissues or body fluids • Mucous membranes, injections • Venereal • Swine, sheep, goats, dogs • Fomites © Universities Press (India) Private Limited Universities Press

PATHOGENESIS • B. melitensis – most pathogenic, B. suis, B. abortus and B. canis • BRUCELLOSIS – ZOONOSIS • Animal infection – GIT, skin, mucus membrane – lymph nodes – bacteremia – multiply in uterus and mammary glands – growth on CAM – abortion – spontaneous recovery – vaginal secretions, urine and milk © Universities Press (India) Private Limited Universities Press

PATHOGENESIS • Site – lymphatics – lymph nodes – lymphadenopathy – bloodstream – liver/spleen/bone marrow – joints, heart, kidneys, CNS and genital tract • Incubation period – 3 weeks © Universities Press (India) Private Limited Universities Press

ENTRY INTO THE BODY Macrophage activation Polymorph migration & Phagocytosis Intracelluar multiplication Lymphatics RES organs Blood Any organ © Universities Press (India) Private Limited Universities Press

Pathogenecity and Immunity Entry into the body Ingested by PMN and not killed Spread to local LN, multiply and spread to blood. Reaches to RES (Spleen, Liver, BM, LN). Resist phagocytosis (Inhibits the phagolysosome fusion). Spread (CNS, Heart, Joints, Respiratory, Skin, GU system) Host response leads to granuloma formation and necrosis. © Universities Press (India) Private Limited Universities Press

PATHOGENESIS • Acute brucellosis – intermittent fever 38– 41°C – evening, temperature – rapid fall – profuse sweating • Undulant fever – periodic nocturnal fever – weeks, months, years • Temperature accompanied by myalgia and arthralgia • Chronic brucellosis – 6 months, serological evidence only – hypersensitivity/joint pain • Latent brucellosis – serological evidence only © Universities Press (India) Private Limited Universities Press

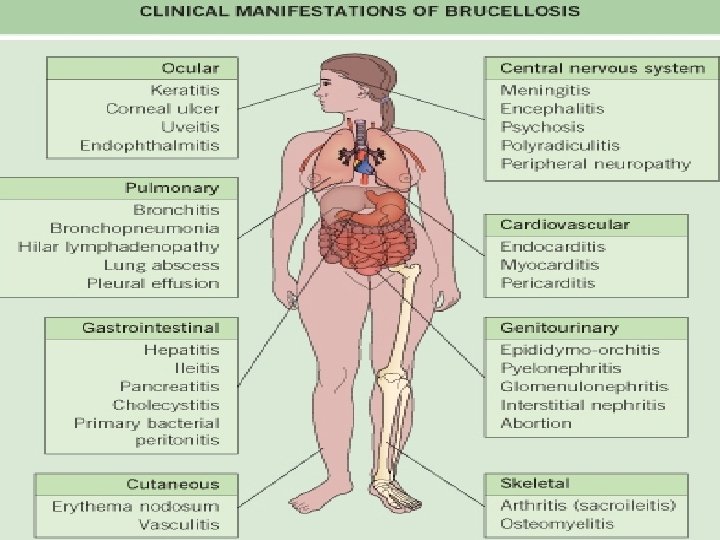
Human Disease • Can affect any organ or system • All patients have a cyclical fever – Headache, weakness, arthralgia, depression, weight loss, fatigue, liver dysfunction © Universities Press (India) Private Limited Universities Press

Human Disease • 20 -60% of cases – Osteoarticular complications • Arthritis, spondylitis, osteomyelitis • Hepatomegaly may occur • Gastrointestinal complications • 2 -20% of cases – Genitourinary involvement • Orchitis and epididymitis most common © Universities Press (India) Private Limited Universities Press

Human Disease • Neurological – Depression, mental fatigue • Cardiovascular – Endocarditis resulting in death • Chronic brucellosis is hard to define – Length, type and response to treatment variable – Localized infection • Blood donations of infected persons should not be accepted © Universities Press (India) Private Limited Universities Press

Human Disease • Congenitally infected infants – – – – Low birth weight Failure to thrive Jaundice Hepatomegaly Splenomegaly Respiratory difficulty General signs of sepsis (fever, vomiting) Asymptomatic © Universities Press (India) Private Limited Universities Press

Chronic brucellosis: It is hard to define - Length, type and response to treatment variable The localized form: -Bones and joints. -Lumbar spondylodiscitis, sacroiliitis is typical. -Orchitis also frequent. © Universities Press (India) Private Limited Universities Press

Sequelae are highly variable - Granulomatous hepatitis, - Arthritis, spondylitis, - Anaemia, leuukopenia, thrombocytopenia, - Meningitis, uveitis, optic neuritis, - Endocarditis. © Universities Press (India) Private Limited Granuloma of Liver Universities Press

Diagnosis in Humans • Isolation of organism – blood, bone marrow, CSF, urine, abscess, vaginal discharge • Serum agglutination test – Four-fold or greater rise in titer – Samples 2 weeks apart • Immunofluorescence Method – Organisms in clinical specimens • PCR © Universities Press (India) Private Limited Universities Press

LABORATORY DIAGNOSIS • Culture – blood culture – trypticase soy broth, 37°C – 5– 10% CO 2 – 5 ml blood/subculture solid media – 3– 5 days – should not be declared negative 6 – 8 weeks • Castaneda – biphasic method © Universities Press (India) Private Limited Universities Press
: Biphasic medium. Sample inoculated bottle has")
Blood cultures in trypticase soya broth (Castaneda’s method): Biphasic medium. Sample inoculated bottle has to be tilted to flow the broth over solid medium and keep it upright position at 370 C. The growth of brucellae is extremely slow. Bone marrow cultures are more sensitive than blood. © Universities Press (India) Private Limited Universities Press

Demonstration of Ig. M , Ig. G and Ig A • ELISA is the best method. Ig. M and Ig. G – differentiate acute and chronic Standard tube agglutination test: Anti -O-polysaccharide of LPS. Killed strains of B. abortus as antigen. Not useful for B. canis. Modified Tube agglutination test: 2 -mercaptoethanol is added to serum before testing which causes disruption of Ig. M and only Ig. G are detected. Prozone phenomenon: Presence of blocking or nonagglutinating antibodies. False positives with cholera, tularemia, yersinia or vaccination. © Universities Press (India) Private Limited Contd…. . Universities Press

Castaneda strip test: Strip with colored brucella antigen. On addition of patients serum, if antibodies are present, prevents the flow of serum. Brucellin Skin test: Delayed hypersensitivity. +ve indicates prior sensitisation Molecular techniques: PCR Radiology: Alterations in infected vertebrae; Pedro Pons sign and marked osteophytosis are suspecious of brucellic spondylitis.

Diagnosis in Animals Culture of urine and Milk. Rapid latex agglutination test, Rose Bengal card test. (Rose Bengal + B. abortus + Sodium azide) © Universities Press (India) Private Limited Contd…. Universities Press

Milk Ring Test: Frequently used test. A drop of colored brucella antigen (B. abortus/B. melitensis with hematoxylin) is added to milk in a test tube, incubated in a water bath at 700 C for 40 -50 minutes. Positive: Blue ring at the top leaving the milk unstained. Negative: No ring. Milk remains uniformly blue. © Universities Press (India) Private Limited Universities Press

DETECTION – MILK • Whey agglutination test – Antibody milk detection infected animals in dairies – pooled milk samples – culture and antibody detection © Universities Press (India) Private Limited Universities Press

PROPHYLAXIS • Checking brucellosis – diary animals • Pasteurisation of milk • Vaccines – Brucella abortus strain 19 vaccine – cattle, no suitable vaccine for human use • Treatment – Streptomycin + Tetracycline or Rifampicin + Doxycycline © Universities Press (India) Private Limited Universities Press
- Slides: 49