Genetic Disorders Dr Mohamed Hesham Sayed Professor of













 inheritance •")


 o Polyploidy: Multiple of the haploid (> Diploid)")




 Translocation : the transfer of a chromosome or a segment of")





















 Trisomy 21")

 (1) Non-disjunction : “ 95 % of cases” • It is")


 (2) Translocation : “ 4 % of cases” • The extra")







 (3) Mosaicism : “ 1 % of cases” • Some cells")






 Mental retardation • Moderate - severe range except in mosaic •")
 Characteristic physical features (in the absence of mental retardation, they should")
 • Clinodactly (incurved little finger)")
















 Common")

 Karyotyping = chromosomal study • To establish diagnosis • To determine genetic")




 At Birth. . Edema of dorsum of hand & feet")











 Achondroplasia, Osteogenesis imperfecta 2) Neurofibromatosis")




 2")









 4 -")












 A. R. – unaffected parents pass it on to offspring – males and")



 is a human")





 inheritance • It results from interaction between genetic predisposition and environmental factors")















- Slides: 176
Genetic Disorders Dr. Mohamed Hesham Sayed Professor of Pediatrics Rabigh Medical College
Objectives • Identify the different types of genetic disorders • Appreciate that malformations are a common and significant health burden. • Recognize the red flags that signify a potential underlying genetic syndrome that need a genetic referral. • Define malformations, their types and causes; recognize that they may be isolated or part of a larger spectrum and appreciate their medical implications.
Basic definitions • • • Chromosomes, DNA and genes Chromatides, and centromere Arms of a chromosome (p and q) Karyotype Autosomes and sex chromosomes Genotype and phenotype
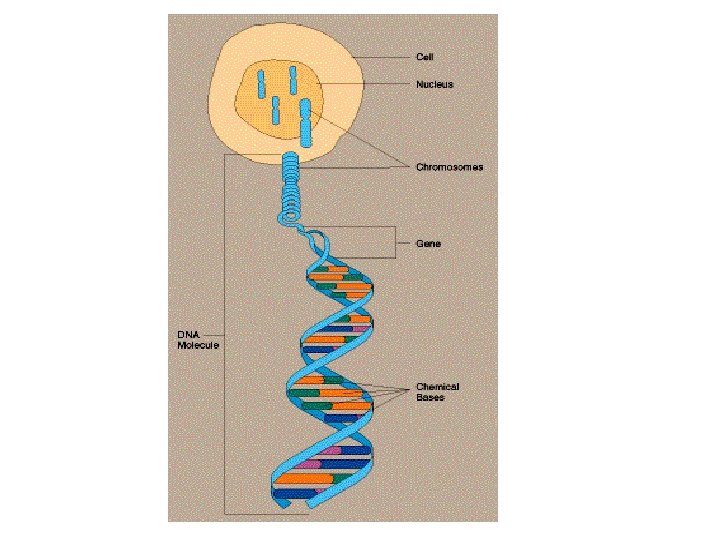
Human Chromosomes • The chromosome is that portion of the chromatin material of the nucleus which carries the genetic information. • Chromosomes are composed of deoxyribonucieic acid (DNA) on framework of protein.
• Segments of DNA molecules comprise the genes; the units of heredity. • During cell division, the chromosome can be seen to consist of 2 parallel strands; the chromatids, held together at one point, the centromere.
Chromosomes
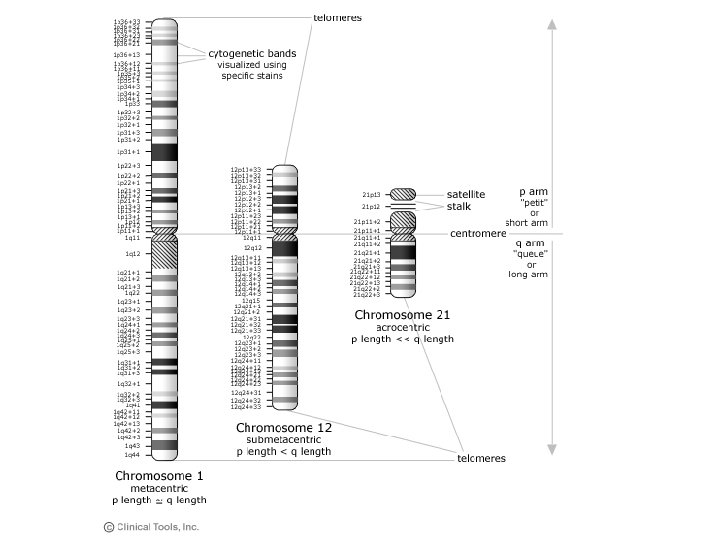
Short arm and long arm
Karyotype • It is the set of chromosomes of an individual. • It is the systematized arrangement of the chromosomes of a single cell. • Chromosomes are arranged in groups A to G according to their shape & size.
• In the human cell, there are 46 chromosomes or 23 pairs (diploid number); of these 23 pairs, 22 are similar in both sexes and are called the autosomes. The remaining pair is called sex chromosomes : XX in the female cells and XY in the male cells. • The genotype is the set of genes the individual carries. • The phenotype is the external appearance of an individual as determined by his genotype.
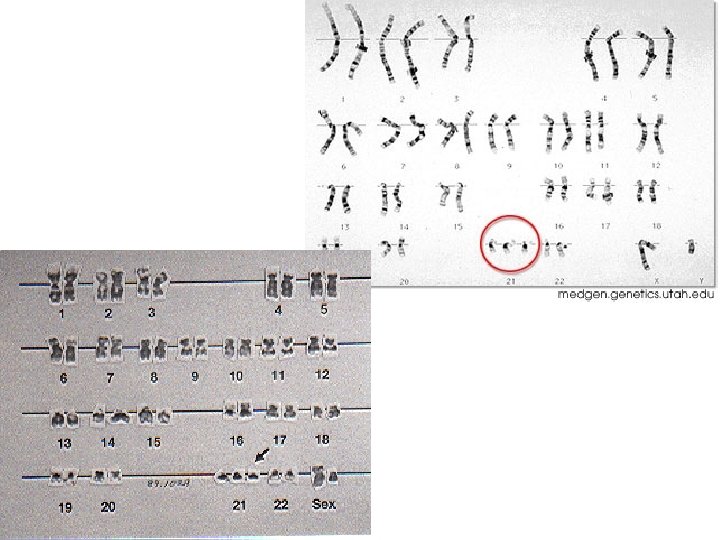
Karyotype of a normal male
Karyotype of a normal female
Karyotype of a normal male
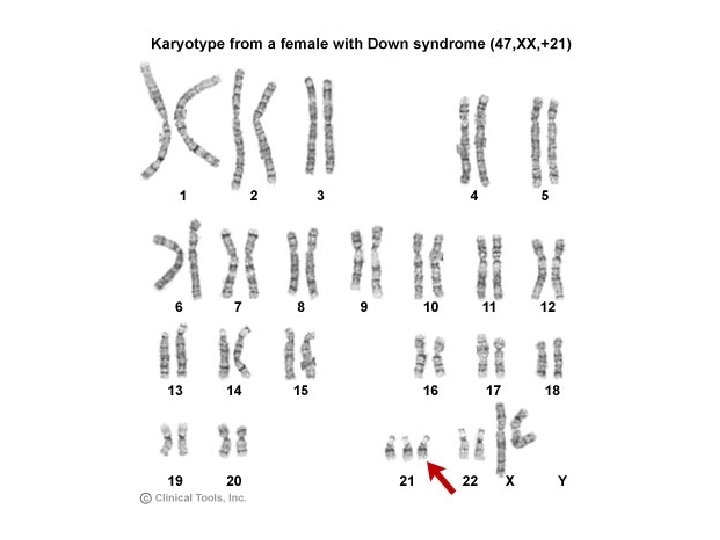
Karyotype of a female Down syndrome
Genetic Disorders • Chromosomal abnormalities • Single gene disorders • Multifactorial (polygenic) inheritance • Unusual patterns e. g. mitochondrial inheritance • Due to teratogens
Chromosomal Abnormalities
Chromosomal Abnormalities • Chromosomal abnormalities are either • • numerical or structural. They are a very common cause of early spontaneous miscarriage. Usually, but not always, cause multiple congenital anomalies and learning difficulties.
Chromosomal Abnormalities • Numerical Aberrations (abnormalities) o Polyploidy: Multiple of the haploid (> Diploid) o Aneuploidy: Abnormal number • Structural abnormalities o Translocation o Deletion o Others
Numerical Aberration • Autosomal - Trisomies: 1 ch extra (e. g. trisomy 21 -13 -18) - Monosomies: 1 ch is missing • Sex chromosome - Klinefilter syndrome (47, XXY male) - Turner syndrome (45, XO female)
Numerical abnormalities Trisomy i. e. 47 chromosomes - Trisomy 21 (the extrachromosome is No 21) - Klinefelter syndrome ( 47, XXY male) Monosomy i. e. 45 chromosomes - Monosomy 21 - Turner syndrome (the missing chromosome is X in female : 45, X or 45 XO )
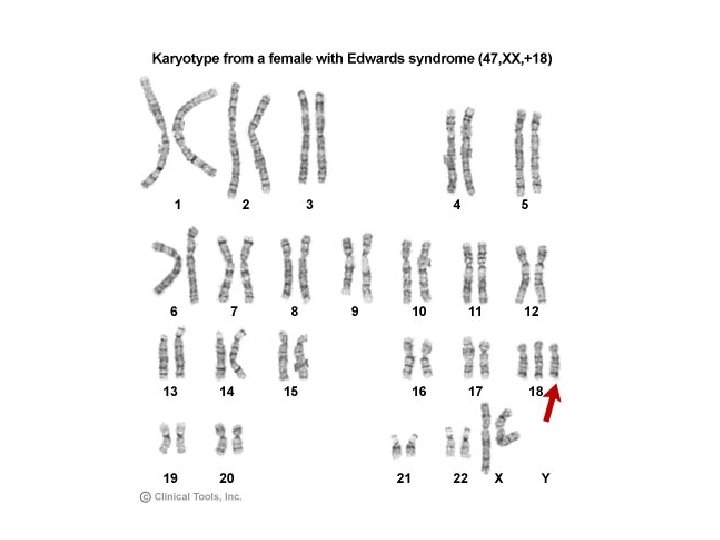
Trisomy 18, Edward Syndrome
Overlapping of the fingers in Edwards' syndrome
Structural abnormalities 1) Translocation : the transfer of a chromosome or a segment of it to a non-homologous chromosome. 2) Deletion : loss of a portion of a chromosome. 3) Ring chromosome 4) Duplication : extra piece of a chromosome. 5) Inversion : fragmentation of a chromosome followed by reconstitution with a section inverted. 6) Isochromosomes : division of chromosome at centromere transversely instead of longitudinally
Structural abnormalities
Structural abnormalities
Structural abnormalities
Structural Abnormalities Inversion Deletion Duplication
Structural Abnormalities Isochromosome Ring chromosome
Structural abnormalities Robertsonian Translocation Reciprocal Translocation
Reciprocal translocations • An exchange of material between two different chromosomes is called a reciprocal translocation. When this exchange involves no loss or gain of chromosomal material, the translocation is 'balanced' and has no phenotypic effect. • Balanced reciprocal translocations are relatively common, occurring in 1 in 500 of the general population.
Reciprocal translocations • Finding a balanced translocation in one parent indicates a recurrence risk for future pregnancies and antenatal diagnosis by chorionic villus sampling or amniocentesis should be offered as well as testing of relatives.
Reciprocal Translocation
Reciprocal Translocation Robertsonian Translocation
Robertsonian Translocation
When to suspect chromosomal abnormalities? • Abnormal features * coarse facies * Mongoloid eye * Low set ears * Micrognathia/cleft lip & palate * Simian crease * Clinodactyly • Mental retardation Do chromosomal analysis • Ambiguous genitalia Do chromosomal analysis • Delayed puberty: Klinefelter syndrome and Turner syndrome
Coarse Features
Cardiofaciocutaneous Syndrome Antimongoloid slant
Low set Ears
Low set Ears
Micrognathia
Ambiguous Genitalia
Ambiguous Genitalia
Clinodactyly
Clinodactyly
Down Syndrome (Mongolism) Trisomy 21
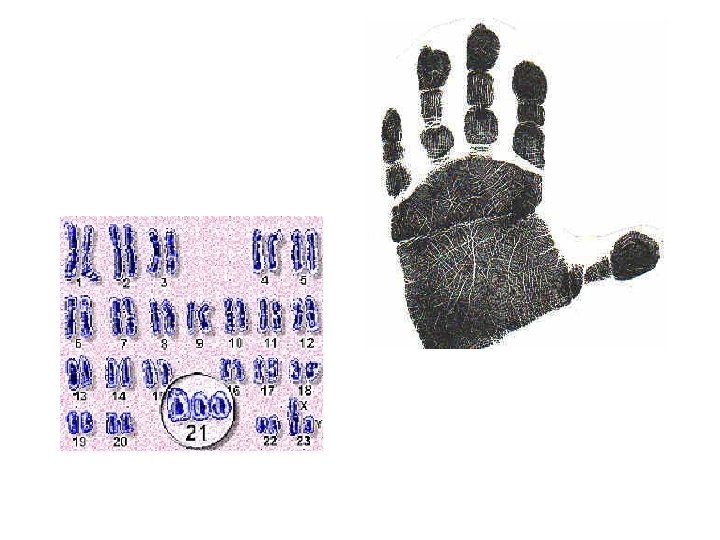
Down Syndrome Incidence : • The most common chromosomal aberration • Incidence 1/700 live birth & 10 % of M. R. Definition : It is trisomy 21 i. e. the cell contain an extra chromosome, number 21 i. e. the cell contains three 21 chromosomes instead of two.
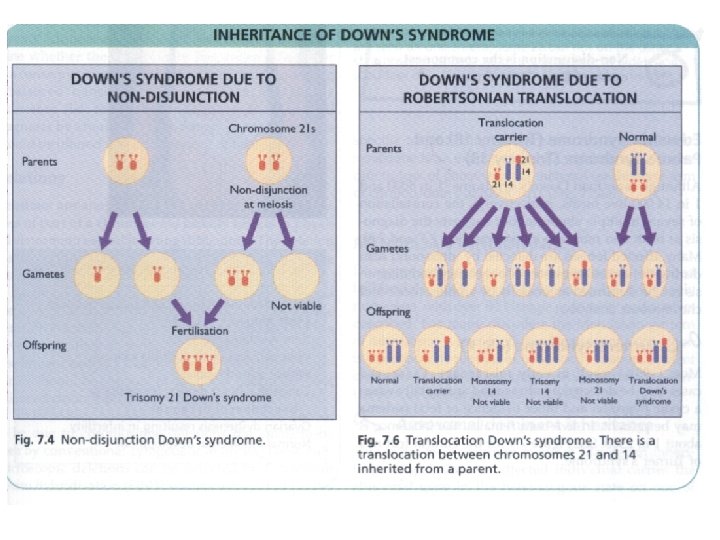
Genetic types (Cytogenetics) (1) Non-disjunction : “ 95 % of cases” • It is due to failure of disjunction of the 2 chromosomes of the pair No 21 during division, the extra 21 chromosome is separate and so total no. in cell is 47. • Incidence is higher with increasing maternal age & so it is age-dependent
Cytogenetics
Non-disjunction
Genetic types (Cytogenetics) (2) Translocation : “ 4 % of cases” • The extra 21 chromosome is translocated (attached) to another chromosome e. g. (15/21) so total no. of chromosomes is 46 but the genetic material is that of 47 chromosomes. • Incidence is usually in young mothers & risk of recurrence is high & mother is called translocation carrier
Translocation
Types of translocation
Down syndrome Translocation carrier
Down syndrome Translocation carrier • One parent contains a 14/21 translocation and has only 45 chromosomes, and is a phenotypically normal carrier. • 1/4 of the individual's gametes will have almost 2 copies of chromosome 21. • The resulting zygote has 46 chromosomes, but almost 3 copies of chromosome 21, and exhibits Down syndrome.
Translocation carrier Recurrence Risk ? ?
Translocation carrier Recurrence Risk ? ?
Figure 8. 4 Translocation Down's syndrome. There is a translocation between chromosomes 21 and 14 inherited from a parent
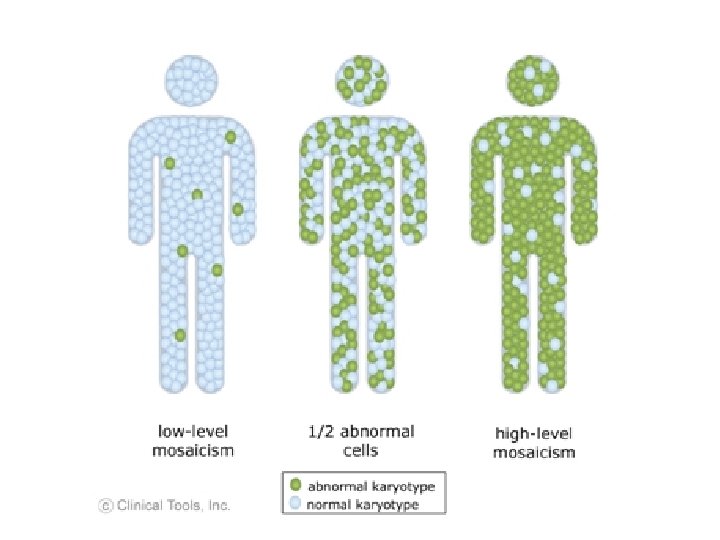
Genetic types (Cytogenetics) (3) Mosaicism : “ 1 % of cases” • Some cells are normal (46 chromosomes) & others are trisomic (47 chromosomes) • Clinical feature are less evident & M. R. is mild.
Down syndrome-Prenatal diagnosis • Triple test ( low estriol, low maternal serum alphafetoprotein and elevated HCG) is often associated with chromosomal syndromes; 15 -18 weeks • Quad screen (quad test): Triple test + inhibin A (↑ ) • Ultrasonography: nuchal thickening; 11 -14 weeks • Amniocentesis: chromosomal analysis; 15 -18 weeks • Chorionic villous sampling: chromosomal analysis; 10 -12 weeks
Normal nuchal thickening
Abnormal nuchal thickening
Chorionic villous sampling
Amniocentesis
Clinical Features Diagnosis depends on abnormal features IN THE PRESENCE OF mental retardation & delayed motor development (due to hypotonia)
Clinical Features 1) Mental retardation • Moderate - severe range except in mosaic • Manifested by delayed smiling, laughing & recognition of mother. 2) Delayed motor development (Hypotonia) • Delayed head support, sitting & standing
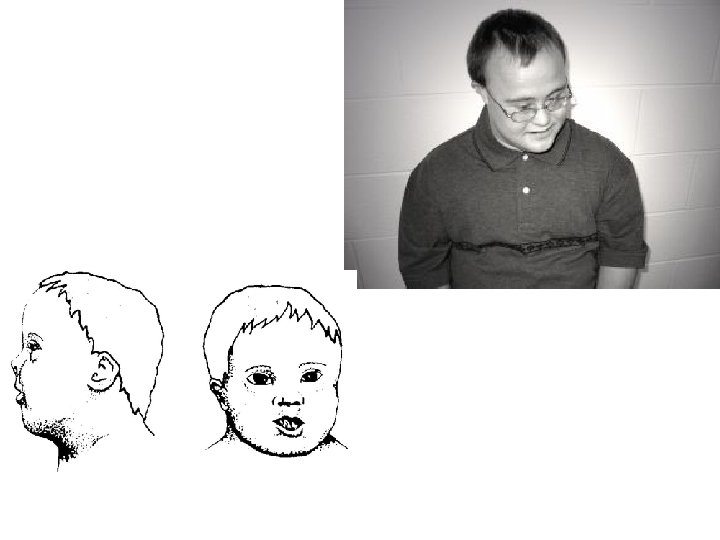
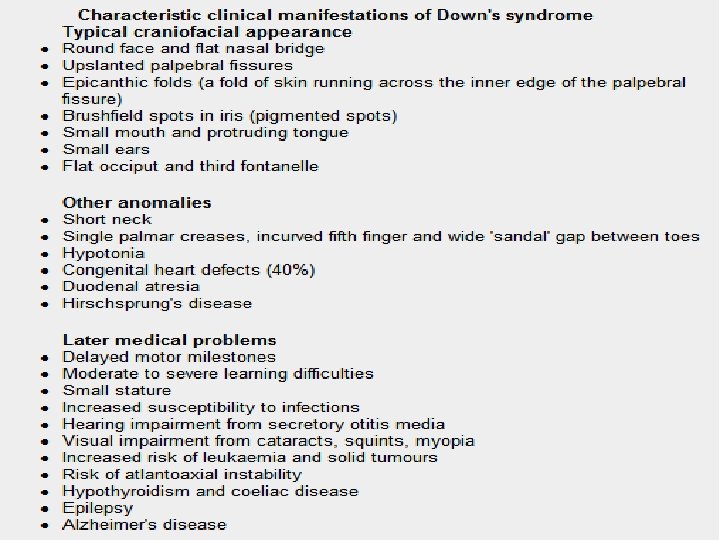
Clinical Features 3) Characteristic physical features (in the absence of mental retardation, they should NEVER be considered diagnostic) Head • Flat occiput • Upward slanting of palpebral fissure • Epicanthal folds • Flat nasal bridge • Malformed ears • Protruded tongue
Clinical Features Hands • Simian crease (transverse palmar crease) • Clinodactly (incurved little finger) • Short broad hand Feet • Big space between the first and second toes
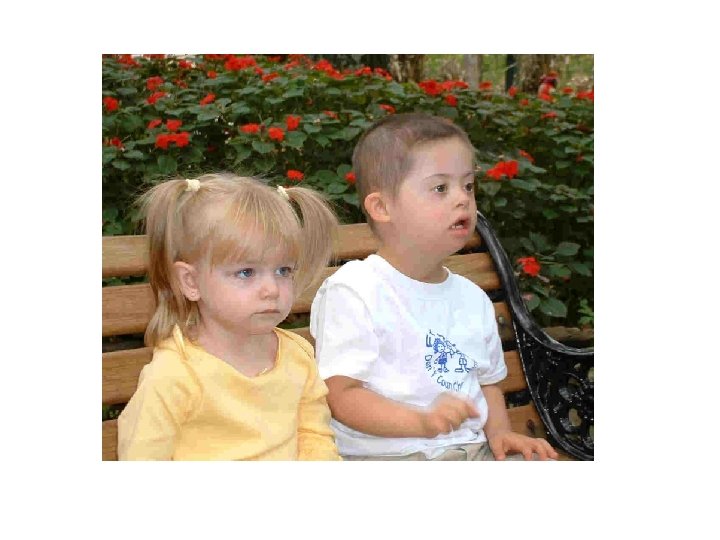
Down syndrome, child
Baby demonstrates the typical features of Down syndrome
Brushfield spots
Brushfield spots
Brachycephaly
Simian Crease, Trisomy 21
Simian Crease, Trisomy 21
Short broad hand
Gap between first and second toes
Gap between first and second toes
Down Syndrome
Down Syndrome
Clinical Features Associated congenital anomalies 1 - Congenital heart disease: (40% of cases) Common atrioventricular canal or VSD 2 - GIT anomalies: Duodenal atresia 3 - Renal anomalies Complications 1 - Recurrent chest infections: due to hypotonia and CHD 2 - Leukemia : 20 times commoner in trisomy 21.
Genetic counseling • Parents need information about o o short-and long-term implications of the diagnosis. how and why the condition has arisen, risk of recurrence antenatal diagnosis for future pregnancies. • > 85% of infants with trisomy 21 survive to 1 yr of age. • Severe CHD is a major cause of early mortality. • At least 50% of affected individuals live > 50 years.
Investigations 1) Karyotyping = chromosomal study • To establish diagnosis • To determine genetic type for genetic counselling & prognosis 2) Chest X - ray & echocardiography for suspected congenital heart disease. 3) Others : hearing and vision testing and checking thyroid profile due to increased risk of hypothyroidism
Management • Supportive care : 1 - Proper nutrition & medical care to diagnose and manage possible complications. 2 - Special social & educational care in specialized institutes like speech therapy aiming to make the child as independent as possible
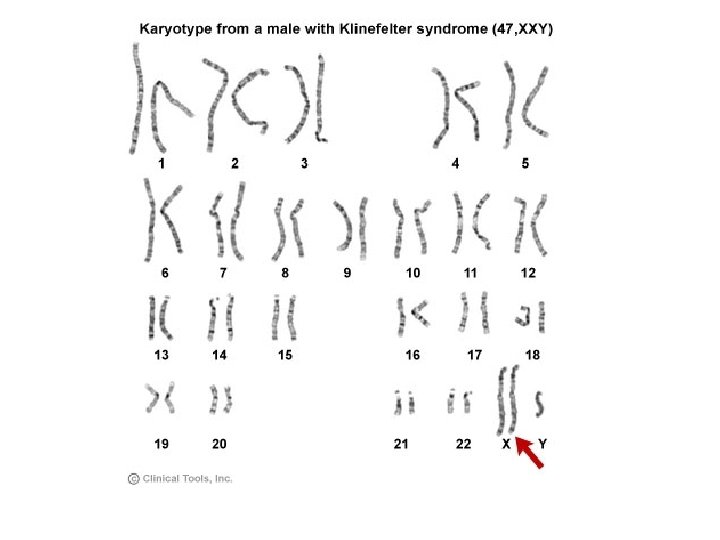
Klinefelter syndrome Cytogenetics 47, XXY, MALE Incidence: 1/1000 Features • Hypogonadism with small testes • Gynecomastia • Tall stature (tall legs) • Infertility (most common presentation) • A common but not a serious disease, which may benefit from testosterone therapy
Klinefelter syndrome
Turner syndrome Cytogenetics: 45, XO, FEMALE Incidence: 1/5000 Features • Lymphedema of hands and feet in newborn • Short stature • Webbing of neck • Wide carrying angle • Gonadal dysgenesis (1 ry amenorrhea) • Renal anomalies and cardiac anomalies
Turner syndrome (Gonadal Dysgenesis) At Birth. . Edema of dorsum of hand & feet . . Webbing of neck. Childhood period - Short stature - Head . . Low posterior hairline - Neck . . Webbing of the neck - Chest. . Broad chest & wide spaced nipples - Limbs. . Cubitus valgus
Turner syndrome Adolescence - Failure of development of 2 ry sex characters - 1 ry amenorrhea (streaked ovary) - Normal mentality, Some learning disability Associated anomalies & complications: 1 - Cardiac anomalies: Bicuspid aortic valve – AS - coarctation of aorta 2 - Renal anomalies: Horseshoe kidney 3 - Ear: Recurrent OM – SNH loss
Turner syndrome - Treatment • Growth hormone therapy • Oestrogen replacement for development of secondary sexual characteristics at the time of puberty (but infertility persists).
Turner Syndrome
Turner Syndrome, webbed neck
Turner Syndrome, webbed neck
Turner Syndrome, Lymphedema
Single gene disorders
Single gene disorders • Every trait is represented by 2 genes, one from the father and the other from the mother. When the 2 genes for any given trait are similar, the person is homozygous for this trait. If the 2 genes are different, the person is heterozygous.
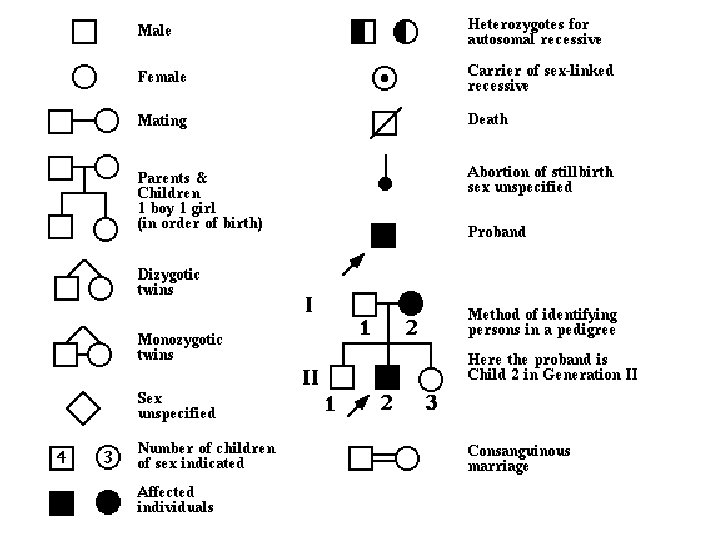
• A dominant gene expresses itself whether homozygous or heterozygous while recessive gene expresses itself only when homozygous. • Family pedigree means summarizing genetic data that is collected by observing the patterns of transmission of traits within the family
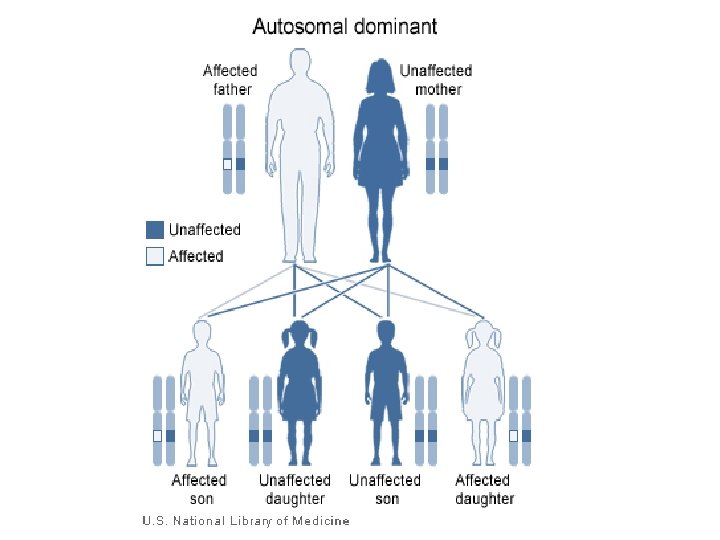
Autosomal dominant inheritance Characteristics : 1 - Every affected person has an affected parent. 2 - Unaffected persons are normal, do not transmit the trait, no carrier state 3 - The trait appears in every generation, no skipping 4 - The trait is transmitted by an affected person to 1/2 of his children at least. 5 - Transmission of trait is not influenced by sex or consanguinity; male to male transmission occurs
Autosomal dominant pedigree
Autosomal dominant inheritance Examples : mostly structural abnormalities 1) Achondroplasia, Osteogenesis imperfecta 2) Neurofibromatosis 3) Congenital spherocytosis, Von willebrand disease 4) Fascioscapulohumoral muscle dystrophy
Autosomal dominant inheritance Complicating factors include the following. Variation in expression Within a family, some affected individuals may manifest the disorder mildly and others more severely. Non-penetrance Refers to the lack of clinical signs and symptoms in an individual who must have inherited the abnormal gene.
Non-penetrance Example of non-penetrance. I 1 and III 2 have otosclerosis. II 2 has normal hearing but must have the gene. The gene is non-penetrant in II 2.
Autosomal dominant inheritance No family history of the disorder • A new mutation in one of the gametes. • The most common reason for absence of a family history in dominant disorders, e. g. >80% of individuals with achondroplasia have normal parents. Homozygosity In the rare situation where both parents are affected by the same autosomal dominant disorder, there is a 1 in 4 risk that a child will be homozygous for the mutant gene.
Autosomal dominant inheritance
Autosomal recessive inheritance Characteristics: 1 - Affected persons are only homozygous(2 abnormal genes) 2 - Unaffected persons can be normal or carriers (1 abnormal gene) 3 - The parents of the affected child may be consanguineous (strong relation to consanguineous marriage)
4 - Both parents of affected child have affected gene. 5 - On the average 1/4 of sibs (recurrence risk is 25%) of affected child are also affected. Males & females are equally affected. 6 -The trait appears mainly in sibs of patient not his parents or off springs.
Autosomal recessive inheritance
Autosomal recessive inheritance
Pedigree to show autosomal recessive inheritance.
Autosomal recessive inheritance
Autosomal recessive Inheritance • Usually there is no previous family history • The most likely place to find a second affected child is a sibling of the first
Autosomal recessive inheritance • Inbreeding increases the chance of observing an autosomal recessive condition • e. g. Cystic fibrosis, sickle cell disease, Tay Sachs disease.
Autosomal recessive inheritance Examples : mostly defective enzymatic activity - Galactosemia, phenylketonuria - Thalassemia and sickle cell anemia - Albinism - Werdnig - Hoffman's disease
Sex-linked recessive inheritance Characteristics : 1 - The trait is expressed by all males who carry the gene, but females are affected only if they are homozygous (only if father is affected & mother is carrier). 2 - The trait is never transmitted from a father to his son, no male transmission
3 - Unaffected males give unaffected offspring (unless marries a carrier female) 4 - An affected male passes the gene through all his daughters (carriers) to half their sons who become diseased and half their daughters who become carriers.
X-linked recessive inheritance
X-linked recessive inheritance
X-linked recessive inheritance • Over 400 disorders • Males are affected • Females can be carriers but are usually healthy • Each son of a female carrier has a 1 in 2 (50%) risk of being affected • Each daughter of a female carrier has a 1 in 2 (50%) risk of being a carrier • Daughters of affected males will all be carriers • Sons of affected males will not be affected, since a man passes a Y chromosome to his son.
X-linked recessive inheritance
X-linked recessive inheritance.
Sex-linked dominant inheritance Characteristics : 1 - Affected male transmits the trait to all his daughters but none of his sons. 2 - Heterozygous female transmit the trait to 1/2 children of either sex while homozygous female transmit the trait to all children of either sex (in the same way as autosomal dominant). Examples : 1 - Vitamin D resistant rickets 2 - Pseudohypoparathyroidism
• The key for determining if a dominant trait is X-linked or autosomal is to look at the offspring of the mating of an affected male and a normal female. • If the affected male has an affected son, then the disease is not X-linked. • All of his daughters must also be affected if the disease is X-linked. • In Pedigree 5, both of these conditions are met.
X-linked dominant inheritance • The trait is never passed from father to son. • All daughters of an affected male and a normal female are affected. All sons of an affected male and a normal female are normal. • Matings of affected females and normal males produce 1/2 the sons affected and 1/2 the daughters affected. • Males are usually more severely affected than females. The trait may be lethal in males. • In the general population, females are more likely to be affected than males, even if the disease is not lethal in males.
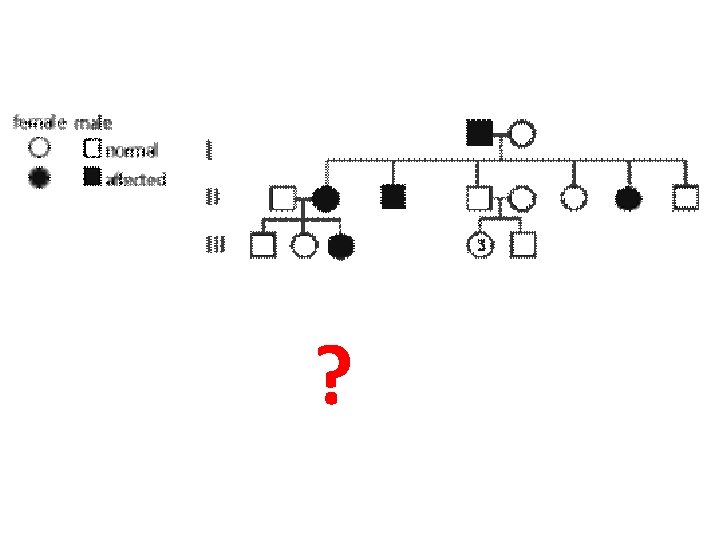
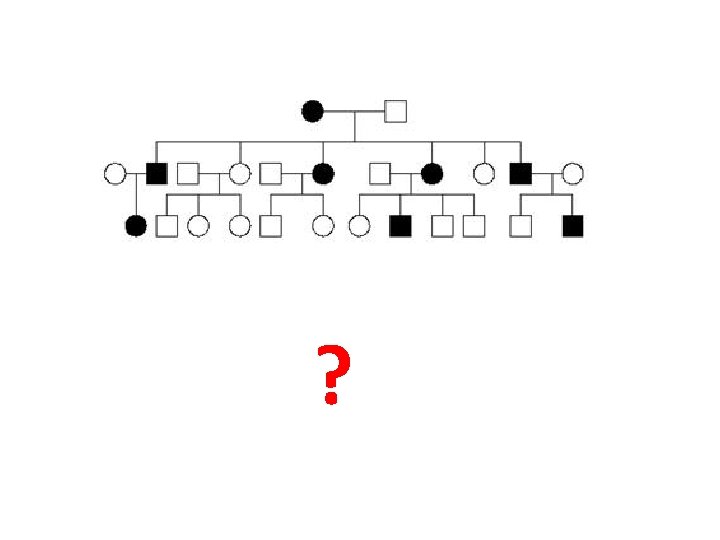
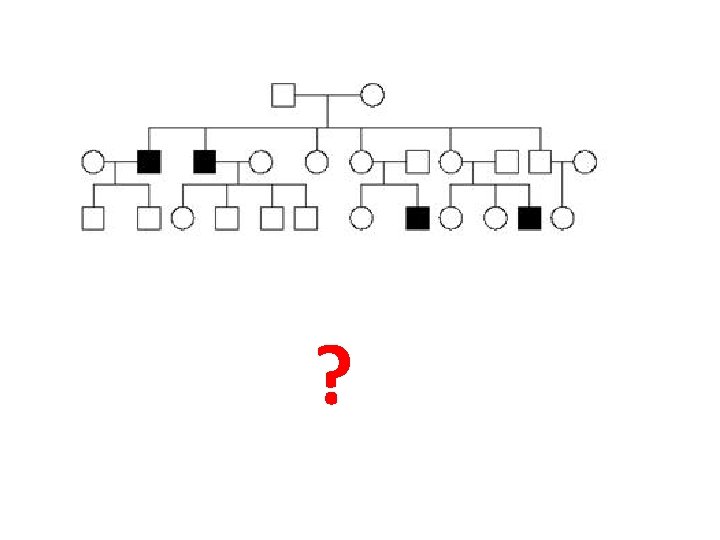
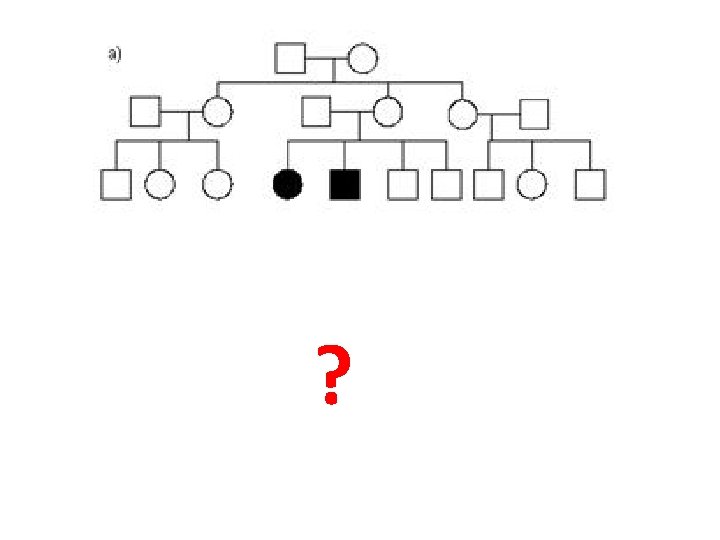
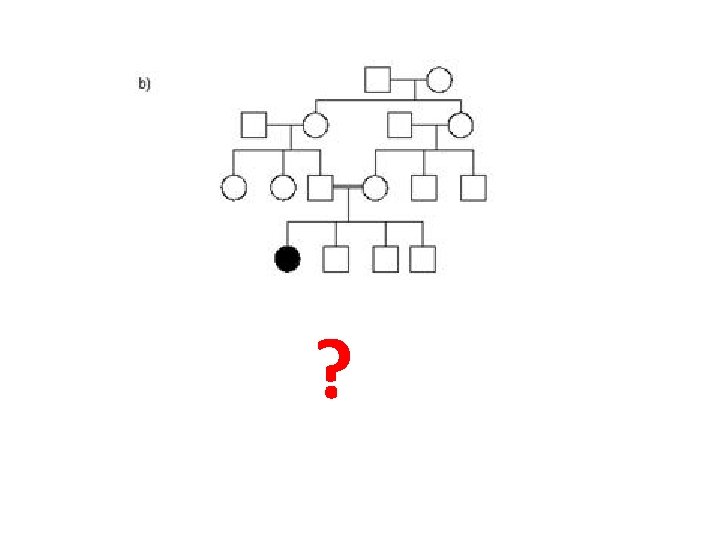
Exercises ?
A. Autosomal Dominant B. Autosomal Recessive C. Sex linked recessive D. Sex linked Dominant E. None of the Above
a. Mode of inheritance? Autosomal Dominant b. Why? All generations, no skipping, males and females
3. a. Mode of inheritance? X- linked Recessive b. Why? Only males affected, unaffected parents (moms) pass it on…
a) A. R. – unaffected parents pass it on to offspring – males and females affected b) A. R. – consanguineous marriage – female affected – unaffected parents
Fragile X syndrome • The prevalence of severe learning difficulties in males due to fragile X syndrome is about 1 in 4000. • This condition was initially diagnosed on the basis of the appearance of a gap (fragile site) in the distal part of the long arm of the X chromosome. • Diagnosis is now achieved by molecular analysis of the CGG (Cytosine-Guanine) trinucleotide repeat expansion in the relevant gene (FMR 1)
Fragile X syndrome
Fragile X syndrome
Trinucleotide repeat expansion mutation FMR 1 (fragile X mental retardation 1) is a human gene that codes for a protein called fragile X mental retardation protein, or FMRP
Trinucleotide repeat expansion mutation
Fragile X syndrome • These unusual findings are explained by the nature of the mutation, which occurs in 'pre-mutation' and 'full mutation' forms. • Norma copy of gene < 50 copies of CGG trinucleotide. • Genes with premutation contain 55 -199 copies. • Genes with full mutation contain > 200 copies of CGG. • This big number affects gene function, leading to learning disabilities.
A child with fragile X syndrome. At this age, the main physical feature is often the prominent ears.
Fragile X syndrome
Fragile X syndrome Clinical findings in males in fragile X syndrome • Moderate-severe learning difficulty (IQ 20 -80, mean 50) • Macrocephaly • Macro-orchidism - postpubertal • Characteristic facies - long face, large everted ears, prominent mandible and broad forehead, most evident in affected adults. • Other features - mitral valve prolapse, joint laxity, scoliosis, autism, hyperactivity • Fragile X syndrome is the second most common genetic cause of severe learning difficulties after Down's syndrome.
Multifactorial (polygenic) inheritance • It results from interaction between genetic predisposition and environmental factors • Such disorders are much common than single gene disorders with much lower recurrence risk • Examples are cleft lip, congenital heart disease, spina bifida, pyloric stenosis; and in later life diabetes, hypertension and asthma
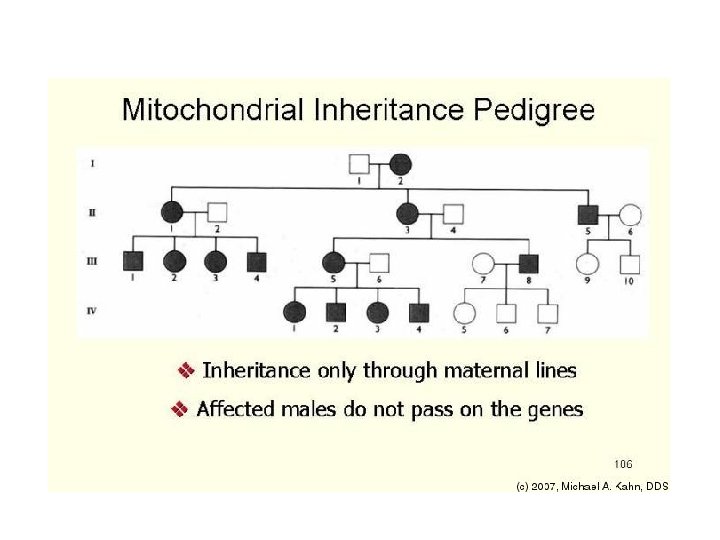
Mitochondrial inheritance • Mitochondria are cytoplasmic organelles that function as major energy producers for the cell and contain their own DNA (mt DNA). • Sperm do not contain mitochondria, so a father with a disorder due to a mitochondrial DNA mutation will not have affected children. • Mitochondrial DNA mutations show only maternal transmission.
Mitochondrial inheritance
Common teratogens • Maternal illness, DM, HTN, Epilepsy • Maternal infections, TORCH • Drugs and toxins – Thalidomide, anticogulants, anticonvulsants, psychiatric drugs • Alcohol and smoking. – Fetal alcohol syndrome • Ionizing radiation
Dysmorphology The term 'dysmorphology' literally means 'the study of abnormal form' and refers to the assessment of birth defects and unusual physical features that have their origin during embryogenesis.
Pathogenic mechanisms Malformation A primary structural defect occurring during the development of a tissue or organ, e. g. spina bifida and cleft lip and palate. Deformation Implies an abnormal intrauterine mechanical force that distorts a normally formed structure, e. g. clubfoot, congenital hip dislocation
Pathogenic mechanisms Disruption Involves destruction of a fetal part which initially formed normally; e. g. amniotic membrane rupture may lead to amniotic bands which may cause limb reduction defects. Dysplasia Refers to abnormal cellular organization or function of specific tissue types, e. g. skeletal dysplasias and dysplastic kidney disease.
Disruption
Pathogenic mechanisms Sequence Refers to a pattern of multiple abnormalities occurring after one initiating defect. Potter's syndrome (fetal compression and pulmonary hypoplasia) is an example of a sequence in which all abnormalities may be traced to one original malformation, renal agenesis. Association A group of malformations that occur together more often than expected by chance, but in different combinations from case to case, e. g. VACTERL association (Vertebral anomalies, Anal atresia, Cardiac defects, Tracheo. Esophageal fistula, Renal anomalies, Limb defects).
Pathogenic mechanisms Syndrome When a particular set of multiple anomalies occurs repeatedly in a consistent pattern, this is called a 'syndrome'.
Early diagnosis of single gene disorders • Prenatal diagnosis for thalassemia and Duchenne myopathy • Presymptomatic diagnosis for some autosomal disorders with onset in later life • Carrier detection for x-linked disorders as hemophilia and Duchenne myopathy by testing factor VIII and creatine kinase in suspected females. DNA markers are more accurate.
Genetic counselling • It is providing information about hereditary disorders i. e. its meaning, risk, and prevention or treatment if any • Components: 1) Correct diagnosis by history, examination and investigations including DNA testing 2) Risk estimation 3) Communication with family 4) Discussion of options for prevention and treatment if any
Genetic counseling, indications 1. Advanced maternal age 2. Consanguinity 3. Child with congenital anomalies or dysmorphic 4. Maternal history of stillborn with congenital anomaly
Gene therapy • It is the artificial introduction of genes into disease tissue in order to cure the diseases • Steps Integration of the introduced gene into the chromosomal DNA of recipient cells by transferring the gene into suitable cells and then inserting the transfected cells into the patient • One example is cystic fibrosis
Gene therapy
Thank You