General Summary of DM with Medications part II
 영양병원 내과 이준엽")





 Initial")









 (h) excretion Meglitinide repaglinide 1. 5")


 weight loss 2) improve lipid profile 3) no hypoglycemia")
 renal insufficiency (s-Cr > 1. 4 in women, >1. 5")

 DRUG retinoic PPARg RXR Regulates gene transcription AGGTCA X AGGTCA")

 hepatotoxicity (AST/ALT, BIL MONTHLY FOR THE FIRST 8 MONTHS,")

 inflammatory")


 <1. 4 Sulfonylurea Meglitinide Biguanide -GI TZD Insulin")









- Slides: 50
General Summary of DM, with Medications (part II, drug therapy) 영양병원 내과 이준엽
Drug Therapy 1. Oral hypoglycemic agent ① ② ③ ④ ⑤ ⑥ Sulfonylurea Meglitinide Biguanides -glucosidase inhibitor Thiazolidinedione Others – orlistat, sibutramine 2. Insulin
Action Mechanisms of Oral Hypoglycemic Agents
Relationship between Hb. A 1 c and sugar level Hb. A 1 c above normal level (%) 1 2 3 4 5 6 7 8 Mean blood glucose (mg/dl) ∼ 150 ∼ 180 ∼ 210 ∼ 245 ∼ 280 ∼ 310 ∼ 345 ∼ 380 Nathan DM, et al. , NEJM 310: 341, 1984 Hb. A 1 c BG 6. 5 = 135 7. 0 = 150 7. 5 = 165 8. 0 = 180 8. 5 = 195 9. 0 = 210 9. 5 = 225 10. 0 = 240 10. 5 = 255 11. 0 = 270 11. 5 = 285 12. 0 = 300 13. 0 = 330
Monitoring Parameters for Control of Complications Every visit Blood Pressure Foot Exam (55% achieve goal) ____________________________ 3 -6 months A 1 C - Every 3 months if treatment changes or not meeting goals - Every 6 months if stable ____________________________ Annual Dilated Eye Examination (63% achieve goal) Lipid Levels* Microalbumin ____________________________ *Every 2 years if levels fall in lower risk categories
Impact of Therapies on A 1 C Levels Therapy § § § A 1 C Reduction Diet and Exercise 0. 5 - 2. 0% Sulfonylureas and Glitinides 1. 0 - 2. 0% Metformin 1. 0 - 2. 0% -Glycosidase Inhibitors 0. 5 - 1. 0 % Thiazolidinedione 0. 5 - 1. 0% Insulin >5. 0% Nathan, D. Oct 2002. N Engl J Med, Vol. 347, No. 17
Flow Chart by Initial Sugar Level in Type 2 Diabetes(By Staged Diabetes Management) Initial Sugar Level FBS < 180 mg/dl Random < 250 mg/dl Diet & Exercise Oral Agent Initial Sugar Level FBS 180 -250 mg/dl Random 250 -350 mg/dl Combination Initial Sugar Level FBS > 250 mg/dl Random > 350 mg/dl Insulin
Major target organs and actions of OHAs in Type 2 DM. TZD = thiazolidinedione; FFA = free fatty acid; AGI =a-glucosidase inhibitor.
Therapeutic Agents for Type 2 Diabetes Mechanism of Action 1. Sensitize the body to insulin Agent 2. Control hepatic glucose production 3. Stimulate the pancreas to make more insulin 4. Slow the absorption of starches 5. Decreases hepatic glucose production and increases peripheral glucose uptake Thiazolidinediones, Biguanides, Thiazolidnediones Sulfonylureas Meglitinides Alpha-glucosidase inhibitors Insulin
Sulfonylureas Increase endogenous insulin secretion • Efficacy - decrease blood glucose ~ 60 mg/dl - reduce Hb. A 1 c 1. 0 - 2. 0 % - no specific effect on plasma lipids or blood pressure • Other Effects - hypoglycemia - weight gain
Sulfonylureas
Characteristics of sulfonylurea Generic name Approved Daily Duration of Dosage Range, mg Action, h Clearance First generation Chlorpropamide(Diabinase) 100 -500 Tolazamide 100 -1000 Tolbutamide 500 -3000 >48 12 -24 6 -12 Second generation Glipizide(Diagreen) 2. 5 – 40 Glyburide(Daonil) 1. 25 -20 Gliquidone(glurenorm) 30 -180 Gliclazide(Diamicron) 80 -240 Glimepiride(Amaryl) 1 -8 12 -18 12 -24 24 Renal Hepatic, renal Hepatic, renal
Indications of Sulfonylurea 1. Onset age > 40 years 2. Onset duration < 5 years 3. Normal weight or obese 4. Never received insulin or controlled < 40 U/day
Contraindications of Sulfonylurea 1. Type 1 DM or pancreatic DM 2. Pregnant or lactating women 3. Undergoing surgery 4. Severe infection 5. Severe stress or trauma 6. Severe adverse reaction to sulfonylurea : Indication of Insulin Therapy
Side Effects of Sulfonylurea 1. Hypoglycemia 2. Weight gain 3. Allergies to sulfonylureas 4. Alcohol intolerance 5. Hyponatremia
Meglitinides Non-sulfonylurea insulin releasing agent; taken before each meal Rapid onset of action with a duration of action of several hours • Efficacy - decrease peak postprandial glucose - decrease blood glucose 60 - 70 mg/dl - reduce Hb. A 1 c 1. 0 - 2. 0 % • Other Effects - hypoglycemia - weight gain - safe at higher levels of creatinine than sulfonylureas
Glinides Dose range Peak level Half-life Metabolite (mg/day) (h) excretion Meglitinide repaglinide 1. 5 -12 (Novo norm ) 0. 75 1 inactive bile D-phenylalanine derivative nateglinide 360 (Fastic ) 1. 0 1. 4 weakly active kidney
Biguanides Decrease hepatic glucose production and secondarily may increase insulin-mediated peripheral glucose uptake • Efficacy - decrease blood glucose ~ 60 mg/dl reduce Hb. A 1 c 1. 0 - 2. 0% cause small decrease in LDL-C and triglycerides no specific effect on blood pressure no weight gain • Other Effects - diarrhea and abdominal discomfort - lactic acidosis if inappropriately prescribed - contraindicated in patients with impaired renal function
Metformin activates AMPK in liver and muscle to improve glucose and lipid metabolism in type 2 diabetes.
Biguanides • Agent-specific advantage 1) weight loss 2) improve lipid profile 3) no hypoglycemia • Side effects 1) lactic acidosis (1/20, 000 Pt. yr) 2) nausea, diarrhea, anorexia
Biguanides • Contraindications 1) renal insufficiency (s-Cr > 1. 4 in women, >1. 5 in men) 2) any form of acidosis 3) congestive heart failure 4) severe liver disease
Thiazolidinediones Potentiate insulin action on muscle and adipose tissue , decrease peripheral insulin resistance • Efficacy - decrease FPG ~ 25 - 40 mg/dl - reduce Hb. A 1 c ~ 0. 5 - 1% (full hypoglycemic potency, until 12 Wks of Tx. ) - combined with sulfonylureas reduce Hb. A 1 c ~ 0. 8 - 1. 0 % - combined with insulin reduce Hb. A 1 C by 0. 8 - 1. 4% - Beneficial effect on lipids - Possible cardiovascular effects • Other Effects - contraindicated with abnormal liver function - weight gain, edema
Mechanism of Action(PPAR- ) DRUG retinoic PPARg RXR Regulates gene transcription AGGTCA X AGGTCA PPRE (DR-1) Gene encoding GLUT-4, lipoprotein lipase, PEPCK etc.
Mechanism of action of Thiazolidinediones.
Thiazolidinediones • Side Effects 1) hepatotoxicity (AST/ALT, BIL MONTHLY FOR THE FIRST 8 MONTHS, EVER 2 MONTHS FOR THE FIRST YR) 2) minor weight gain(1 -2 kg) 3) peripheral edema • Contraindications 1) liver disease 2) congestive heart failure (class III or IV)
Alpha-Glucosidase Inhibitors Competitive inhibitor of alpha glucosidase enzymes in small intestines; taken before meals • Efficacy - decrease fasting plasma glucose 20 -30 mg/dl decrease peak postprandial glucose 40 -50 mg/dl no specific effect on lipids or blood pressure reduce Hb. A 1 c 0. 5 -1. 0% • Other Effects - abdominal discomfort and flatulence - contraindicated with inflammatory bowel disease or cirrhosis
Alpha-Glucosidase Inhibitors • Side effects diarrhea, flatulence, abdominal distension, hepatotoxicity • Contraindication 1) inflammatory bowel disease 2) gastroparesis 3) s-Cr > 2. 0 mg/dl
Anticipated Response to Treatment
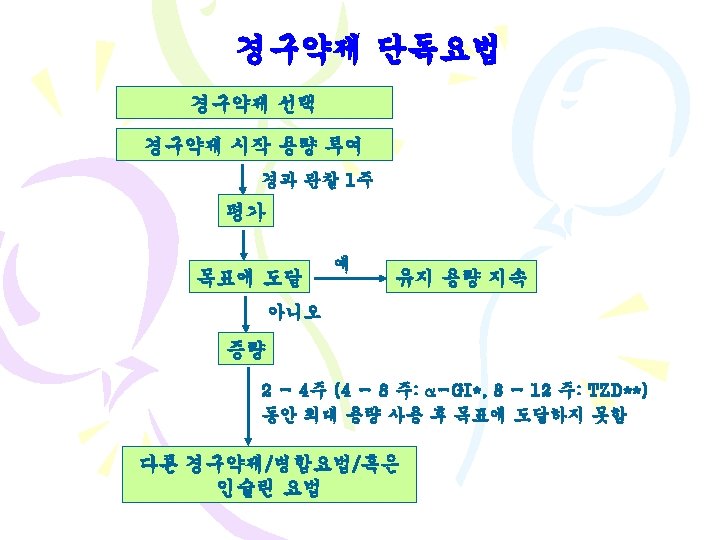
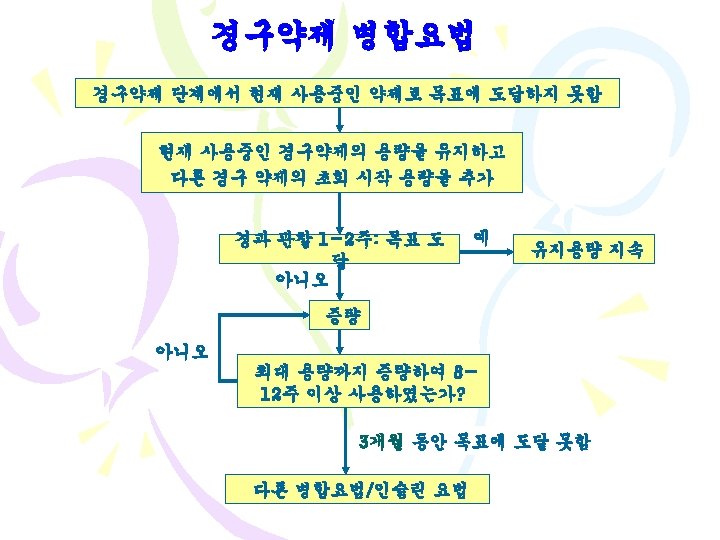
Oral hypoglycemic agents
동반질환에 따른 약물의 선택 신기능(mg/d. L) <1. 4 Sulfonylurea Meglitinide Biguanide -GI TZD Insulin 1. 4~2. 0 간기능 >2. 0
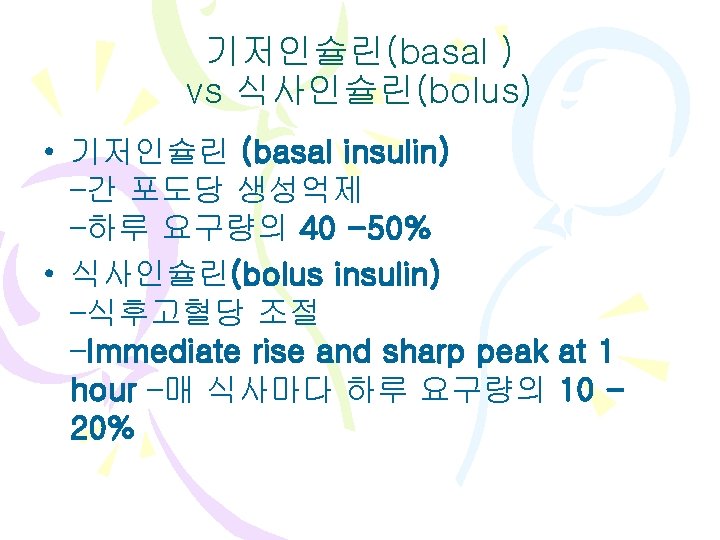
Insulin Decreases hepatic glucose production and increases uptake and use of glucose by muscle and adipose tissue • Efficacy - can lower plasma glucose to any level - reduces Hb. A 1 c > 5. 0% - limited by hypoglycemia • Other Effects - hypoglycemia - weight gain
Onset of action, peak, and duration of action of exogenous insulin preparations. (Neutral protamine Hagedorn = NPH)
The Incretin Effect Demonstrates the Response to Oral vs IV Glucose • Insulin Secretions : Oral > IV glucose
Schematic drawing of the role of DPP-IV in the inactivation of incretins (GLP-1, GIP, PACAP) (see text). DPP-IV-truncated GLP-1 and GIP act as weak receptor antagonists
The Incretin Effect Is Reduced in Pts. With T 2 DM
GLP-1 Key Regulating Peptide in Glucose Metabolism
Profile of ideal insulin replacement pattern.
당뇨조절의 실제 Breakfast Lunch Dinner Diabetes Normal Surfonylurea Meformin 노보넘 AGI 4: 00 8: 00 12: 00 16: 00 20: 00 24: 00