GENERAL CONSIDERATIONS COMPONENTS AND CLASSIFICATION OF FPD CHRISTEENA







: That is luted or otherwise securely retained to natural")



























































 - Tooth supported FPD : - Conventional or")



 ü Core-plastic core material -amalgam")




















: 259 -64. �Comparison of Metal-Ceramic and All-Ceramic Three-Unit")








 with one")








")












 Collected a data on the safety & efficiency of")
 Suggested that composite materials used for luting adhesive FPDS demonstrated a")

) �Described a technique for a")
 �Compared three methods of etching metals for resin")
 �studied the effect of oxidation of alloys on the")






- Slides: 136
GENERAL CONSIDERATIONS, COMPONENTS AND CLASSIFICATION OF FPD CHRISTEENA JOSEPH 2 nd YEAR PG DEPT OF PROSTHODONTICS
CONTENTS �INTRODUCTION �GENERAL TERMINOLOGY �GENERAL CONSIDERATIONS �INDICATIONS AND CONTRAINDICATIONS OF FPD �COMPONENTS OF FPD �RETAINERS ü Classification ü Materials used
�PONTIC ü Classification ü Ideal requirements �CONNECTORS ü Types of connectors �CLASSIFICATION OF FPD ü Fixed – fixed FPD ü Fixed removable FPD ü Cantilever FPD ü Spring cantilever FPD �OTHER SYSTEMS OF CLASSIFICATION �ADVANTAGES AND DISADVANTAGES
�REVIEW OF LITERATURE �CONCLUSION �SUMMARY �REFFERENCE
INTRODUCTION
�The need for replacing missing teeth is important for the patient when the edentulous space is in the anterior segment of the mouth but it is equally important in the posterior region. � when a tooth is lost the structural integrity of the dental arch is disrupted & there is a subsequent realignment of teeth and new state of equilibrium is achieved.
�Missing teeth can be replaced by one of the three prosthesis types –RPD , tooth supported FPD & an implant supported FPD.
GENERAL TERMINOLOGY �Fixed partial denture(bridge): That is luted or otherwise securely retained to natural teeth, tooth roots and / or dental implant abutments that furnishes the primary support for the prosthesis. GPT – 8) �Crown An artificial replacement that restores missing tooth structure by surrounding part or all of the remaining structure with a material such as cast metal , porcelain or a combination of material such a metal and porcelain.
�Retainer The part of a fixed dental prosthesis that unites the abutments to the remainder of the restoration. (GPT-8) �Major and minor retainers The retainer in fixed movable bridge that is rigidly united to the terminal pontic is known as major retainer. A retainer that is united to the pontic by a semi rigid joint is called as a minor retainer.
�unit. Each part of the bridge, retainer or pontic may be reffered as a unit. Therefore a bridge replacing one premolar and using two retainers are termed as three unit bridge. �Pontic An artificial tooth on a fixed dental prosthesis that replaces a missing natural tooth , restores in function, and usually fills the space previously occupied by the clinical crown.
�Connector The portion of a fixed prosthesis that unites the retainer and pontic �Pier or intermediate abutments Any abutment other than the terminal abutment of an FPD is termed as pier. �Conventional bridges These bridges employ conventional retained design and do not depend upon adhesive technique for their retention.
�Resin bonded bridges These depend upon adhesive technique for there retention and are cemented using resin cements. �Hybridges These bridges consist of one or more conventional bridge retainers combined with resin bonded retainer
�Inlay-A fixed intracoronal restoration; a dental restoration made outside of a tooth to correspond to the form of the prepared cavity, which is then luted into the tooth �Onlay-A restoration that restores one or more cusps and adjoining occlusal surfaces or the entire occlusal surface and is retainedby mechanical or adhesive mean
GENERAL CONSIDERATIONS �THE PATIENT ü When explaining to the patient about the differences between a fixed and removable prosthesis , the advantage of a denture and its economic advantages should not be minimized. ü The main advantage of an FPD is that it is fixed and does not need to be removed from the mouth as the denture. ü involves teeth adjacent to the space. Inlays and crowns-4 th edition, colin. R. Cowell
ü The main disadvantage is that the time and cost and the problems associated with repair after damage. �THE EDENTULOUS SPACE ü The bridges are ideally used for restoring small gaps within a complete arch having strong and well supported teeth on either end of the space. ü Other considerations in edentulous space. Vertical height being diminished by an overeruption of an unopposed tooth. Inlays and crowns-4 th edition, colin. R. Cowell
ü Spaces may be also diminished by drifting , rotating or tilting of the tooth. �Occlusion ü The abutment support and the amount of retention required will vary not only with the length of the span, but also with the force exerted by the opposing teeth. ü Bruxism, pipe smoking and other habits needs to be taken care. Inlays and crowns-4 th edition, colin. R. Cowell
ü Occlusal adjustments may be carried out to remove premature contacts and diminish unwanted lateral stress on the teeth. �SUPPORT AND PERIODONTAL HEALTH. ü The abutment teeth should be able to provide adequate support for the FPD , with all the extra leverage and torque which it will impose. ü This support is related to the amount of root area secured in the healthy bone. Inlays and crowns-4 th edition, colin. R. Cowell
�HEALTH OF MUCOSA ü Correct design will allow the function of mastication , toothbrush and interdental cleansers to act on the maximum area of mucosa and prevents food packing. ü This area of mucosal coverage should be kept to minimum and should be accessible for cleansing with dental floss. Inlays and crowns-4 th edition, colin. R. Cowell
�STRENGTH ü Limited by the strength of individual units. ü Points of potential weakness arejoints, the gold frames , and also occlusal or incisal surfaces. ü The requirements for strength of the individual units depends on the amount of the masticatory forces it has to resist over the area of span and retainers. Inlays and crowns-4 th edition, colin. R. Cowell
�APPEARANCE ü Anterior esthetics. �FUNCTION ü Apart from the static function of maintaining the continuity of the dental arch and restoring the appearance, a bridge should have a dynamic function as an effective part of mastication. ü Remove premature occlusal contact and avoid new occlusal problems by placing a fixed prosthesis. Inlays and crowns-4 th edition, colin. R. Cowell
�ABUTMENT CROWNS ü Crown size-a common cause of FPD failure is a choice of abutment with crown with inadequate height. ü The clinical crown should have enough height to allow sufficient retention for the prosthesis. ü Any tooth which has less than 4 mm interproximal from the marginal ridge to gingival attachment is unsuitable. Planning and making crowns and bridges-Bernard GN Smith
�Crown strength ü Caries , existing restorations or endodontic treatment may have weakened an abutment crown. the extent of the caries , primary or secondary must be known before the type of retainer is chosen. ü Radiographic examination is mandatory. Planning and making crowns and bridges-Bernard GN Smith
�Crown shape ü The shape of abutment teeth may cause certain problems, when a partial venner retainer is planned for an upper canine. ü The retention of this type of retainer depends on slots placed in the proximal surfaces. Planning and making crowns and bridges-Bernard GN Smith
CROWN ROOT RATIO 1: 1. 5 considered satisfactory. 1: 1 considered minimal. Long-term abutment prognosis removable prosthesis may be advantageous, when, the ability of the remaining supporting structures to accept excessive occlusal forces is questionable. Planning and making crowns and bridges-Bernard GN Smith
� root length and root form - roots with parallel sides and developmental depressions are better able to resist additional occlusal forces than are smooth-sided conical roots - multirooted teeth generally provide greater stability than single-rooted teeth - longer root has better retention than short root Planning and making crowns and bridges-Bernard GN Smith
Alveolar ridge form considerable loss of alveolar bone may not allow the use of pontics of normal size or their placement to best support the lips and cheeks to restore normal facial form. Age of the patient in mouth of adolescents fixed prosthesis is usually contraindicated due to incomplete eruption of the teeth and large pulp chambers. Inlays and crowns-4 th edition, colin. R. Cowell
�PULP ü The size of the pulp can be assessed by radiograph and knowledge about the pulp. ü A tilted or rotated tooth may have a relatively smaller pulp which is vulnerable because of the position of the tooth. ü If a positive response is elicitated by electrical pulp tester or bur on exposure of the pulp is present, the pulp can be assumed to be healthy enough to receive the prosthesis. Inlays and crowns-4 th edition, colin. R. Cowell
�ABUTMENT ROOTS ü For estimation of the amount of support needed, the combined root area of the abutment teeth should’nt be less than the teeth to be replaced. ü In 1926 DR. Ante stated ‘the combined pericemental area of the abutment teeth should be equal to or greater in pericemental area than the tooth or the teeth to be replaced. ü The life of the prosthesis have also been depended on the quality of the periodontal support as the quantity. Inlays and crowns-4 th edition, colin. R. Cowell
�The occlusal design of the retainers and the pontic to reduce the undue stress on the periodontal tissues is an important prerequisite. �The number, length and shape of the roots will indicate the amount of support available for the bridges. the preference for the abutment teeth are; upper 6, 7, 3, 4, 5, 1, 2, lower 6, 7, 3, 5, 4, 2, 1. 3 rd molar may be used as abutments, but exibit such variations in forms its difficult to place them in order of preference. Inlays and crowns-4 th edition, colin. R. Cowell
�The area of the tooth needed for support will depend on the length of the span to be supported and the amount of leverage to fall on the span. �The upper anteriors usually have a forward projection which creates a leverage arm and requires additional support. Inlays and crowns-4 th edition, colin. R. Cowell
�MULTIPLE ABUTMENTS �Occasionally teeth adjacent to a gap are potentially weak abutment teeth and their sole use as the mesial and distal abutments tooth is contraindicated. �usually found in patients with periodontal problems which would have been controlled before the prosthetic procudures are comensed, but may have reduced the bony attachments to the tooth. �In such cases additional retention is obtained by including additional abutments. Inlays and crowns-4 th edition, colin. R. Cowell
�BONE SURROUNDING ABUTMENT TEETH. �Radiographs of the abutment teeth should be evaluated preferably around the apices of the abutment tooth. �ENDODONTICALLY TREATED TEETH �There is no contraindication for a pulpless tooth as part of the prosthesis , if there is satisfactory root filling. �A periapical lesion or evidence of inadequate endodontic treatment should be reviewed because of further damage may be caused by the prosthesis. Inlays and crowns-4 th edition, colin. R. Cowell
INDICATIONS AND CONTRAINDICATIONS �INDICATIONS Ø In short edentulous patients Ø Abutment teeth and supporting tissues are healthy. Ø To harmonize dental occlusion in temporomandibular disorders Ø To stabilise and splint the dentition after advanced periodontal therapy Ø When the patient desires a fixed prosthesis Tylman’s Theory and practice of Fixed Prosthodontics. WFP. Molone etal
�The patient has the skill to maintain a good prosthestic and oral hygiene �When removable prosthesis is not indicated as in mentally and physically challenged patients. Tylman’s Theory and practice of Fixed Prosthodontics. WFP. Molone etal
CONTRAINDICATION �GENERAL FACTORS : • Age of patient : the young or the very old Length of clinical crown : � younger patient � main cause of the high failure rate (< 21 years) • • Caries rate : Tylman’s Theory and practice of Fixed Prosthodontics. WFP. Molone etal
�GINGIVAL AND PERIODONTAL CONSIDERATIONS : �Gingival hyperplasia : proliferation of the gingival tissues around the bridge �Severe marginal gingivitis : � Any prosthesis is liable to increase plaque formation aggravate any gingivitis � the finishing margins at least 1. 5 -2 mm clear �Advanced periodontal disease : � prognosis of the remaining teeth is obviously poor Tylman’s Theory and practice of Fixed Prosthodontics. WFP. Molone etal
Local factors contraindicating a bridge Prognosis of Abutment Teeth Malformed dentin Extent and position of caries Deep sub-gingival caries Periapical infection Effective root surface Periodontal condition Longer span - Ante’s law Possibility of further loss in same arch Unfavourable tilting rotation of the teeth Tylman’s Theory and practice of Fixed Prosthodontics. WFP. Molone etal
COMPONENTS OF FPD � Parts of FPD involves ; Retainer Pontic connectors Fundamentals of fixed prosthodontics-Herbert. T. Shillingburg
RETAINER This is used for stabilization or retention of the prosthesis �CLASSIFICATION The retainers can be classified on the following criteria; Amount of tooth coverage 1. Complete coverage or full coverage crowns ü Covers all the surfaces of the abutment tooth and maximum retension ü Most commonly used retainer and is the retainer of choice if the abutment teeth are extensively damaged Fundamentals of fixed prosthodontics-Herbert. T. Shillingburg
�Partial veneer retainers or partial coverage retainers �These retainers does not involve all the surfaces of the abutment �Compared to full veneer retainers they require less amount of tooth preparation have superior esthetic but less retentive �Depending on the surface and coverage they are termed as ¾ th crown, 4/5 th crown, 7/8 th crown, one half crown , pinlays and pinledges. Fundamentals of fixed prosthodontics-Herbert. T. Shillingburg
�Conservative retainers ü These retainers require minimum preparation and are advised in the anterior teeth. ü They cannot accept heavy occlusal load �Mechanism of retention 1. Extracoronal retainers Obtain retention from the external surface of the coronal part of the abutment teeth, eg. full vener and partial veneer crowns. Fundamentals of fixed prosthodontics-Herbert. T. Shillingburg
2. Intracoronal retainers Obtain retention from within the coronal tooth structure eg, inlays and onlays �Materials used 1. All metal retainers ü Can be either partial or full coverage. ü Good strength and commonly used in posterior abutment. Fundamentals of fixed prosthodontics-Herbert. T. Shillingburg
ü They require minimal tooth preparation 2. Metal ceramic retainers ü Indicated in both anterior and posterior tooth ü Ceramic can be either a facing or full coverage. ü They require more tooth preparation compared to the all metal 3. all ceramic retainers ü Most esthetic ü but the strength in long span FPD is questionable. Fundamentals of fixed prosthodontics-Herbert. T. Shillingburg
4. Acrylic retainers Used for temporary fixed partial dentures They are not used in defenitive FPD because of their poor strength , color stability, inadequate wear resistance and poor tissue response. Fundamentals of fixed prosthodontics-Herbert. T. Shillingburg
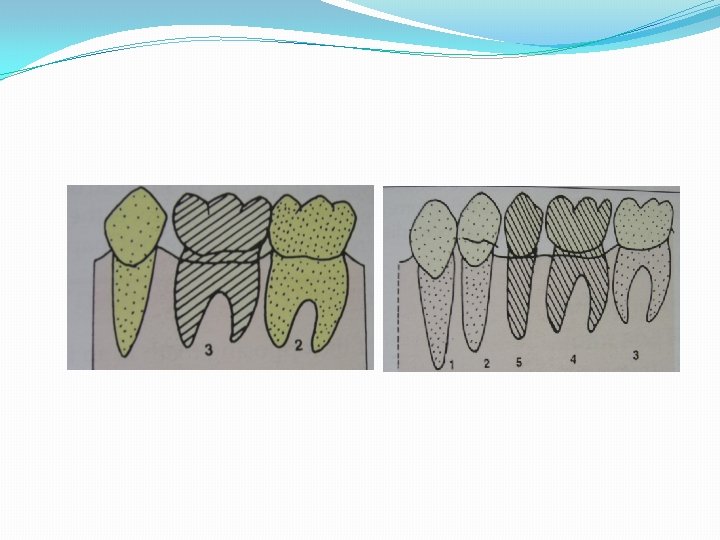
�CRITERIA FOR SELECTION OF RETAINERS Factors governing the selection of retainers are; 1. Abutment angulation 2. Condition of the abutment 3. Aesthetics 4. Preservation of tooth structure 5. Retention 6. Cost Fundamentals of fixed prosthodontics-Herbert. T. Shillingburg
ANGULATION OF THE ABUTMENT TEETH
PONTICS �IDEAL REQUIREMENTS OF PONTICS 1. Restore function of the replaced tooth. 2. Provide esthetics and comfort 3. Should be biologically acceptable 4. Permit effective oral hygiene 5. Preserve the underlying residual ridge and mucosa 6. Have adequate strength to withstand occlusal force Pontics Fundamentals of fixed prosthodontics-Herbert. T. Shillingburg
�Classification of pontics �Mucosal contact Ø With mucosal contact ü Saddle pontic ü Ridge lap pontic ü Modified ridge lap pontic ü Ovate pontic Ø Without mucosal contact ü Bullet pontic ü Hygienic or sanitary pontic Fundamentals of fixed prosthodontics-Herbert. T. Shillingburg
�Type of materials used Ø Metal and porcelain veneered pontic Ø Metal and resin veneered pontic Ø All metal pontic Ø All ceramic pontic �Method of fabrication Ø Custom made pontic Ø Prefabricated custom modified pontic. Fundamentals of fixed prosthodontics-Herbert. T. Shillingburg
CONNECTORS �TYPES OF CONNECTORS 1. rigid connectors �Cast connectors �Soldered connectors �Loop connectors 2. Non rigid connector �Tenon mortise connector �Split pontic connector �Cross pin and wing connector Fundamentals of fixed prosthodontics-Herbert. T. Shillingburg
�RIGID CONNECTORS ü Indicated when entire masticatory load is to be transfered on to the abutment ü They can be directly cast as a part of a multiunit fixed partial denture or different units joined together by soldering. ü The tissue contour should be maintained during the fabrication of the wax pattern ü The size shape and position of the rigid connectors all influence the sucess of the prosthesis Fundamentals of fixed prosthodontics-Herbert. T. Shillingburg
�Non rigid connector ü Limited movement between the retainer and the pontic and have less flexibility �Indications ü When parallel path of insertion cannot be achieved ü Pier abutment ü Periodontally compromised abutments to reduce the stress Fundamentals of fixed prosthodontics-Herbert. T. Shillingburg
ü a shoe/key is incoporated to the mesial half and the keyway in the distal half. The assembly engages when the FPD is seated in position ü Cross pin and wing connector are similar to the split pontic connector and are used for tilted abutments. ü The wing is attached to the distal retainer which is cemented first and pontic to the mesial retainer. Fundamentals of fixed prosthodontics-Herbert. T. Shillingburg
TYPES OF FPD �BASIC DESIGN , COMBINATIONS AND VARIATIONS ü There are four basic designs of bridges, the difference being the type of support provided at each end of the pontic; ü THE FOUR DESIGNS ü Fixed –fixed FPD design ü Fixed –moveble FPD design ü Cantilever design ü Spring cantilever design
CLASSIFICATION OF FPD � ACCORDING TO THE LOCATION �Class 1 -posterior edentulous space. Planning and making crowns and bridges – Bernard GN Smith
� Class II-Anterior edentulous space Planning and making crowns and bridges – Bernard GN Smith
� Class III-Antero-posterior edentulous space. Planning and making crowns and bridges – Bernard GN Smith
�DIVISION �A division gives information about the adjuscent teeth which can renter support. �Division I-Cantilever FPD ü The abutment present only on one side of the edentulous space can be taken for suport. Planning and making crowns and bridges – Bernard GN Smith
�Division II-Conventional FPD ü Abutments capable of taking up occlusal loads are present on both the sides. Planning and making crowns and bridges – Bernard GN Smith
� Division III-pier abutment ü A single tooth is surrouded by and edentous space on either side. Can be treated with a single prosthesis. Planning and making crowns and bridges – Bernard GN Smith
�SUBDIVISION – status of the tooth to be used as an abutment. �Subdivision I-ideal abutment ü Healthy teeth that provide good support. Planning and making crowns and bridges – Bernard GN Smith
�Subdivision II-Tilted abutment ü Either the design of the prosthesis should be modified or the tilt of the abutment should be corrected. Planning and making crowns and bridges – Bernard GN Smith
� Subdivision III-periodontally weak abutment ü This abutment cannot withstand occlusal load compared to a healthy abutment. Planning and making crowns and bridges – Bernard GN Smith
�Subdivision IV-Extensively damaged abutment. ü The abutment has good bone support but needs an extensive restoration. ü Eg, inlays , onlays. Planning and making crowns and bridges – Bernard GN Smith
�Subdivision V-Implant abutment. Planning and making crowns and bridges – Bernard GN Smith
�Each subdivision can be further grouped in two ü Group A- Denotes that one side of the edentulous space is taken from a single abutment. ü Group B-Support for one side of the edentulous space is taken from more than one abutment. Planning and making crowns and bridges – Bernard GN Smith
OTHER SYSTEMS OF CLASSIFICATION 1. Depending upon location - Anterior posterior 2. Depending on number of teeth - 2 Unit bridges - 3 Unit bridges 3. Depending upon the tooth reduction - Conventional preparation bridge - Minimal preparation bridge - Hybridge Textbook of prosthodontics –V. RANGARAJAN
4. Recent classification (depending on support) - Tooth supported FPD : - Conventional or rigid FPD - Cantilever FPD �Resin-Bonded Tooth Supported FPD’s: Rochette Bridge Maryland Bridge Cast Mesh FPD Virginia bridges Textbook of prosthodontics –V. RANGARAJAN
Implant supported FPD : - Screw retained FPD - Cement retained FPD 5. Depending on material used: All metal crowns Metal ceramic crowns All acrylic crowns Ceramic veneers Acrylic veneers 6. Depending upon construction : - Cast metal FPD - CAD CAM assisted FPD - Direct fibre reinforced RBFPD Textbook of prosthodontics –V. RANGARAJAN
7. Depending upon the connector : - Fixed – fixed bridges – Anterior, posterior - Fixed – fixed movable bridges – anterior, posterior - Springs cantilever bridges - Compound bridges 8. Length of span Long span bridges Short span bridges Textbook of prosthodontics –V. RANGARAJAN
� 9. Type of abutment üNormal / ideal abutment üCantilever abutment üPier abutment üMesially tilted abutment -mesial half crown -telescopic crown Textbook of prosthodontics –V. RANGARAJAN
�Endodontically treated abutment(depending on the amount of tooth remaining) ü Core-plastic core material -amalgam -composite -glass ionomer cements -pin retained amalgam ü Post core restoration -custom-made post -prefabricated post Textbook of prosthodontics –V. RANGARAJAN
�Periodontally weak teeth ü Resin bonded bridges ü Fiber reinforced bridges ü Splints -implant abutments 10. Bridges which require minimal preparation Micro retention Macro retention Textbook of prosthodontics –V. RANGARAJAN
FIXED –FIXED DESIGN ü The fixed – fixed FPD has a rigid connector at both the ends of the pontic. ü The abutment teeth are rigidly splinted together and parallel to each other. ü The retainer should have maximum retention to reduce the forces applied to the prosthesis or it may dislodge one retainer from its abutment leaving the other end suspented. ü To minimize this risk the entire occluding surfaces of all the abutment teeth to be covered by the retainers. Inlays crown and bridges-George. F. kantorowicz
FIXED MOVABLE DESIGN �Incorporats a stress redistribuiting device , which allows limited movement at one end of the joints between pontic and the retainer �The fixed end of the bridge has a rigid connector that isusually distal to the pontic-major retainer �The minor retainer having a moveable joint, doesnot require much retention compared to major retainer �The moveable joint provide –support against vertical occlusal forces, allow limited movement for lateral forces. Inlays crown and bridges-George. F. kantorowicz
�This prevents the movement of one retainer transmitting torsional force directly to another and breaking the cement seal. �The cantilever effect of the non rigid retainer gives additional stress on the major retainer and strong abutment is required. �Contraindicated in long spans.
CANTILEVER DESIGN �A cantilever design provides support only at one end. �The pontic may be attached to a single retainer or two or more retainers splinted together, but has no connection at the other end. �The abutment tooth for a cantilever prosthesis may be either mesial or distal to the span but for small designs it distal. Inlays crown and bridges-George. F. kantorowicz
SPRING CANTILEVER DESIGN �Spring cantilever FPDs restricted to the replacement of upper incisors. �Only one pontic can be supported by a spring cantilever prosthesis. This is attached to the end of a long mesial arm running high into the palate and down to the rigid connector on the palatal side of a single retainer or pair of splinted retainers. �The forces applied to the pontic are absorbed spring nature of the arm and the displacement of the soft tissue of the palate. Inlays crown and bridges-George. F. kantorowicz
�The abutments are usually the two premolars splinted together or a single premolar or molar tooth. Inlays crown and bridges-George. F. kantorowicz
COMBINATION DESIGNS �the fixed-fixed and cantilever designs �fixed-fixed and fixed-movable designs. Inlays crown and bridges-George. F. kantorowicz
Advantages : �simplifies the construction of the prosthesis : �complex bridge to be broken down into several �the unfavourable angulation of the abutment �same line of insertion and withdrawal - simplify preparations and conserve tooth structures- lighter preparations �Precision retainers - permit the separation of two or more components �repair Inlays crown and bridges-George. F. kantorowicz
ADVANTAGES AND DISADVANTAGES �Advantages Disadvantages �Fixed-fixed • Splinting effect • Parallel preparation • Larger bridge • Over reduction • Construction • Widely separated teeth • Extensive preparation �Fixed-movable • Divergent abutment • Limited span • Independent retention • Complicated construction • More conservative • Temporary bridge • Minor movements • Cementation Inlays crown and bridges-George. F. kantorowicz
�Cantilever • only one abutment is needed Easy parallel preparation design in case two or more adjuscent abutments. • for longer span more abutment teeth to be used. • Construction must be rigid Construction in lab is relative straightforward procedure Inlays crown and bridges-George. F. kantorowicz
HYBRID DESIGN �Fixed – fixed with one conventional and one minimal-retainer. · Fixed – movable with a minimalretainer carrying the movable connector �Fixed-movable with the conventional retainer carrying the movable connector. �restored abutment- an inlay or conventional retainer other abutment tooth is unrestored Inlays crown and bridges-George. F. kantorowicz
REMOVABLE FPD �permanent cementation of large bridges the maintenance and further endodontic or periodontal treatment of abutment teeth is difficult �can be removed by the patient. �cleaning around the abutment teeth. �acrylic facings Inlays crown and bridges-George. F. kantorowicz
ALL METAL FPD � Esthetics not prime- the best choice � with conventional bridges – the least tooth reduction The margins are easier to adapt to the preparations These dentures are fabricated using only metal Characteristics. They are indicated for replacing maxillary and mandibular posterior teeth. Inlays crown and bridges-George. F. kantorowicz
METAL CERAMIC FPD �When the strength of metal is required together with a tooth-coloured retainer or pontic, metal – ceramic is the best material � Here, metal is used to fabricate the core of the prosthesis. The external surface is fabricated using ceramic. �The metal is bonded to ceramic chemically, mechanically and ionically. Inlays crown and bridges-George. F. kantorowicz
� Metal ceramic fixed partial dentures can be of two types. In the first type, the metal is surrounded by porcelain on all the surfaces. � In the second type the lingual and occlusal surface is formed by metal and the labial and gingival surface is alone formed by porcelain. These restorations are also termed as porcelain facings or porcelain veneers. Inlays crown and bridges-George. F. kantorowicz
�Advantages Aesthetically pleasing. Stronger metal substructure. Characterization possible with use of internal and external stains. � Disadvantages. Significant tooth preparation necessary. To achieve better aesthetics, the facial margin of an anterior restoration is often placed subgingivally, this increases the potential for gingival destruction. Brittle fracture can occur due to failure at the metal ceramic junction. More expensive. Inlays crown and bridges-George. F. kantorowicz
ALL CERAMIC BRIDGES �limited to two-unit cantilever bridges or three-unit fixed bridges. � Compared to the metal ceramic prosthesis it take less time for the laboratory procedures. �All porcelain prosthesis if properly design and constructed will have sufficient strength to survive normal functional forces but will break if subjected to excessive load. Inlays crown and bridges-George. F. kantorowicz
�All ceramics are less fracture resistant, hence, they do not render as good retainers. However, aluminareinforced porcelains (inceram) have sufficient strength to be used as good retainers. Advantages. ü Superior aesthetics. ü Excellent translucency. ü Requires slightly more preparation of the facial surface. The appearance can be influenced and modified by selecting different colors of luting agent. Inlays crown and bridges-George. F. kantorowicz
Disadvantages. � Reduced strength due to lack of reinforcement with metal. � It is very difficult to obtain a well-finished margin because the ceramic edges tend to chip easily. � These crowns cannot be used on extensively damaged teeth because they cannot support these restorations. � Due to porcelain's brittle nature, large connectors have to be used, which usually leads to impingement of the inter-dental papilla. This increases the potential for periodontal disease. . � Wear of opposing natural teeth. Inlays crown and bridges-George. F. kantorowicz
�Int J Prosthodont. 2016 May-Jun; 29(3): 259 -64. �Comparison of Metal-Ceramic and All-Ceramic Three-Unit Posterior Fixed Dental Prostheses: A 3 -Year Randomized Clinical Trial. Nicolaisen MH, Bahrami G, Schropp L, Isidor F. PURPOSE: �The aim of this randomized clinical study was to compare the 3 year clinical outcome of metal-ceramic fixed dental prostheses (MC-FDPs) and zirconia all-ceramic fixed dental prostheses (AC -FDPs) replacing a posterior tooth. MATERIALS AND METHODS: �A sample of 34 patients with a missing posterior tooth were randomly chosen to receive either a MC-FDP (n = 17) or an ACFDP (n = 17). The FDPs were evaluated at baseline and yearly until 3 years after cementation. They were assessed using the California Dental Association assessment system. Periodontal parameters were measured at the abutment teeth, and the contralateral teeth served as control. The statistical unit was the FDP/patient.
� RESULTS: � The success rate was 76% and 71% for MC-FDPs and AC-FDPs, respectively. Three technical complications were observed in the MCFDP group and five in the AC-FDP group, all chipping fractures of the ceramic veneer. Furthermore, one biologic complication in the MCFDP group (an apical lesion) was observed. No framework fractures occurred. All patients had optimal oral hygiene and showed no bleeding on periodontal probing at any of the recalls. Only minor changes in the periodontal parameters were observed during the 3 years of observation. CONCLUSIONS: � Three-unit posterior MC-FDPs and AC-FDPs showed similar high survival rates and acceptable success rates after 3 years of function, and ceramic veneer chipping fracture was the most frequent complication for both types of restorations
ALL ACRYLIC FPD Characteristics. � Only indicated for long-term temporary or interim prostheses. � Can be used for making fixed periodontal splints. � Poor wear resistance. � Easy to fabricate and adjust. � Aesthetically pleasing. Inlays crown and bridges-George. F. kantorowicz
�Veneer is a layer of restoration placed over the labial surface of a tooth. They are primarily used as aesthetic adjuncts to discolored or fractured teeth. � Type of Veneers � Ceramic It is the most ideal veneering material when used with metal substructure or in all ceramic restorations. � Acrylic Tooth colored acrylic can be used with metallic restorations as a veneer. They are not considered as a permanent material due to poor wear resistance. Recent advances include use of indirect composite resins as veneer materials. Inlays crown and bridges-George. F. kantorowicz
COMBINATION OF MATERIALS �A metal – ceramic retainer and pontic with a movable connector to a gold inlay or other minor retainer. �An all – metal retainer (a full or partial crown) towards the posterior end of the bridge with anterior metal-ceramic units. Inlays crown and bridges-George. F. kantorowicz
FIBER REINFORCED COMPOSITE FIXED PROSTHESIS �an innovative alternative � a conservative approach �overcome drawbacks of conventional prostheses. �a fiber-reinforced composite (FRC) substructure veneered with a particulate composite material. �exhibits better physical properties and esthetics than direct placement composite restoratives
Indications : 1. The need for a restoration with excellent appearance. 2. The need to decrease wear of the opposing dentition. 3. The use of conservative intracoronal abutment tooth preparations. 4. The potential for bonding the prosthesis retainer to the abutment. 5. The desire for a metal–free, nonoporcelain prosthesis ( especially metal allergies).
Contraindications : 1. Inability to maintain good fluid control (e. g. , patients with chronic or acute gingival inflammation or when margins would be placed deeply into the sulcus) 2. Long span (i. e. , two or more pontics) 3. Patients with unglazed porcelain or removable partial denture frameworks that would oppose the restoration 4. Patient who abuse alcoholic substances. 5. Parafunctional habits
� Fiber-reinforced Composite Fixed Dental Prostheses with Various Pontics Perea, Leila / Matinlinna, Jukka P. / Tolvanen, Mimmi / Lassila, Lippo V. J. / Vallittu, Pekka K. J Adhes Dent 16 (2014), No. 2 (07. 04. 2014) Page 161 -168 �Purpose: To evaluate the load-bearing capacities of fiberreinforced composite (FRC) fixed dental prostheses (FDP) with pontics of various materials and thicknesses. Materials and Methods: Inlay preparations for retaining FDPs were made in a polymer phantom model. Seventytwo FDPs with frameworks made of continuous unidirectional glass fibers (ever. Stick C&B) were fabricated. Three different pontic materials were used: glass ceramics, polymer denture teeth, and composite resin. The FDPs were divided into 3 categories based on the occlusal thicknesses of the pontics (2. 5 mm, 3. 2 mm, and 4. 0 mm). The framework's vertical positioning varied respectively. Each pontic material category contained 3 groups (n = 8/group).
�In group 1, pontics were fabricated conventionally with composite resin (G-ӕnial, GC) with one additional transversal fiber reinforcement. In group 2, the pontics were polymer denture teeth (Heraeus- Kulzer). Group 3 had an IPS-Empress CAD pontic (Ivoclar Vivadent) milled using a Cerec CAD/CAM unit. Groups 1 and 2 served as controls. Each FDP was statically loaded from the pontic until initial fracture (IF) and final fracture (FF). Initialfracture data were collected from the load-deflection graph. Results: ANOVA indicated statistically significant differences between the materials and occlusal thicknesses (p < 0. 001). Quadratic analysis demonstrated the highest correlation between the thickness of the pontic and IF and FF values with ceramic pontics (IF: p < 0. 001; R 2 = 0. 880; FF: p < 0. 001; R 2 = 0. 953).
RESIN BONDED FPD �As the name implies, these are fixed partial dentures, which are cemented onto the abutments using special resins. � Basically these dentures consist of one or more pontics supported by thin metal retainers placed only on the lingual and/ or proximal surface of the abutments. Retention in these prostheses relies on the adhesive bonding between etched enamel and the metal casting (retainer).
� Indications. ü Retainers for fixed partial dentures for abutments with sufficient enamel to etch for retention. ü Splinting of periodontally compromised teeth. . Stabilizing dentitions after orthodontics ü Medically compromised, indigent and adolescent patients who cannot co-operate with long sessions of therapy. ü Prolonged placement of interim prosthesis to augment surgical procedures.
�Contraindications. ü Patients with an acknowledged sensitivity to base metal alloys . When the facial esthetics of abutments require improvement. ü Insufficient occlusal clearance to provide 2 to 3 mm vertical frictional retention in the axial walls. E. g. abraded teeth. ü Deep vertical overbite. ü Inadequate enamel surfaces to bond. E. g. extensive caries, existing restorations. ü Incisors with extremely thin facio-lingual dimensions. Contemporary fixed prosthodontics -rosenstiel
üAdvantages. Non-invasive to dentin with lingual and proximal tooth preparation including occlusal rests. Decreased pulpal irritation. ü Conservative with undeniable patient appeal/comfort. . Decreased tissue irritation due to the placement of supragingival margins. ü Does not require cast alterations or removable die preparation. Reduced cost with less chair time. Contemporary fixed prosthodontics -rosenstiel
Disadvantages. �Demanding technique and tooth preparation. � Even minor laboratory errors cannot be corrected easily. Plaque accumulation may occur because design is outside the dimensions of the natural tooth. � Bulky contours may be intolerable in some patients. . Patient expectations of esthetics are high. � Not ideal for replacing more than one tooth. Contemporary fixed prosthodontics -rosenstiel
MINIMAL PREPARATION FPD �A simpler design involves attaching pontics through a metal plate to the unprepared (minimally prepared)lingual surface of the adjusent tooth. �The attachment is made by a composite resin material retained by acid etch technique to the enamel �Can be used in teeth with sufficient enamel. �The rochette bridge retained by a cast metal plate with undercut perforation through which the composite flows. Contemporary fixed prosthodontics -rosenstiel
�Maryland bridges have no perforations , but are cast in base metal alloy which is etched electrolytically in a strong acid mixture in a special bath. �Produces a retentive surface similar to an acid etched enamel. the etched surface should not be contaminated before cementation. �Fixed –fixed or catilever prosthesis are used in acid etch technique. Contemporary fixed prosthodontics -rosenstiel
�Indications ü Used in young patients. ü Where a tooth is lost unexpectedly through trauma or when the teeth is lost through periodontal disease and costly replacements are not justified until the prognosis of the periodontal treatment is not clear. �Disadvantages �Sacrifices full occlusal protection of the abutment teeth. Contemporary fixed prosthodontics -rosenstiel
MICROMECHANICAL RETENSION Ø MINIMAL PREPARATION BRIDGES �DIRECT �INDIRECT ü Micromechanical retention (eg, rochette fpd) ü Medium mechanical retention eg, virginia mesh design ü Micromechanical retention eg. Maryland ü Chemical adhesive eg. panavia. Resin bonded marryland bridges-journl of dental sc and rehab, alok kumar et al
Macro-mechanically retentive bridges : �perforations through the cast-metal plate �holes are cut in the wax �Rochette bridge �Funnel shaped perforations to enhance the resin retention-attributed to rochette in 1973. �He combined mechanical retention with a silane coupling agent to produce adhesion. Resin bonded marryland bridges-journl of dental sc and rehab, alok kumar et al
Medium-mechanical retentive systems : �all involve retentive features cast as part of the metal framework. �the cement-film thickness �thick retainer �Virginia design FPD �Cast mesh bridge Resin bonded marryland bridges-journl of dental sc and rehab, alok kumar et al
�Cast mesh fixed partial denture �A net likemesh placed over the lingual surface of the abutment teethon the working cast. �Then covered and incoporated in to the retainer waxpattern. �Undersuface of the retainer becoming a mesh like surface when casted. �Eliminates etching, permit s use of noble metal alloy. �Virginia bridges �Moon and hudgins et al produced particle roughned retainer by incoporating salt crystal into retainer pattern produces roughness on the inner surface. �Lost salt techniques
Micro-mechanical retention : § casting the metal retainer § etching : electrolytic etching in acid chemical etching with a hydrofluoric acid gel § smaller etch pits and unnecessary non-retentive features § thinner metal retainers and cement film. § Maryland bridge § Livaditis and thompson used a 35% solution of nitric acid with a current of 250 Ma/cm² for 5 minutes, followed by immersion in an 18% hcl solution in an ultrasonic cleanser for 10 min, to etch the retainer surface. Resin bonded marryland bridges-journl of dental sc and rehab, alok kumar et al
Chemically retentive resins : § adhere chemically to recently sandblasted metal surfaces § retained by conventional acid-etching
ACID ETCHED RESIN BONDED FIXED PROSTHESIS Advantages of the acid-etch resin bonded fixed prosthesis: 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. Reduction of tooth structure Kind to young or large pulps Maximum esthetics Pontic and embrasure forms easy to keep clean Minimum chair time less expensive than a conventional rebonding possible No permanent damage to the enamel Individual characterization No irreversible procedures are involved
Disadvantages of the acid-etch resin bonded fixed prosthesis 1. Uncertain longevity 2. The added thickness of the retainers. 3. The composite in the countersunk areas may abrade 4. The unfilled resin, a polymer, absorbs water molecules, and fluids 5. No space correction : . 6. No alignment correction : 7. DIfficult temporization :
Indications : 1. missing tooth, adjacent to intact teeth. 2. esthetics is of primary concern. 3. transitional fixed prosthesis 4. Anterior periodontal splinting procedures 5. Lingual ramps on maxillary canines to create canine disclusion. Contraindications : 1. Inadequate horizontal overlap 2. Short teeth with inadequate lingual enamel 3. Previous restorations or large areas of caries
4. Heavy anterior occlusion in excursive movement 5. Deep vertical overlap 6. nickel sensitivity 7. Significant pontic width discrepancy 8. Long edentulous span.
IMPLANT SUPPORTED FPD MOST ADVANCED & DEMANDING ADVANTAGES �Retreivability �Independence from natural teeth �Bone stability DISADVANTAGES �Risk of screw loosening/ fracture �Need for 2 surgeries �Length of treatment time
�INDICATION �Unfavourable attitude toward RPD �Long span FPD questionable �Unfavourable no & location natural abutment �Single tooth restoration �Broad & flat ridge-dense bone �Dry mouth l l CONTRAINDICATIONS Inadequate bone – site Poor quality of bone Medical
l l Lack of experience Smoking Terminal illness Radiation
REVIEW OF LITERATURE �Ariel (2001) Collected a data on the safety & efficiency of anterior ceramic FPD & suggested that it not only replaces anterior missing teeth but also provides patient with safe & effective restoration oral heath social comfort. �Daniel (2002) Studied tooth structure removal associated with various preparation designs for anterior teeth & concluded that resin bonded prosthesis required approximately are half are quarter the amount of tooth reduction of conventional complete coverage.
�Pascal Magne (2002) Suggested that composite materials used for luting adhesive FPDS demonstrated a resilient component that favored stress transfer within the tooth or restoration complex. �Williams V. D, Dremon D. G et al (1982) �studied the effect of retainer design on retention of filled resins to acid - etched FPD’s. �They determined which retainer design had the best retention capacity to enamel. ØRochette used 6 holes with sharp spatula in wax pattern 0. 8 mm in diameter.
Ø Howe and Denehy used 1 -1. 5 mm, 0. 5 mm in diameter. Ø Kuhlke and Drenon used 0. 33 - 0. 5 mm thickness holes drilled Ø Newman bonded orthodontic brackets using fine mesh screen. �They found that all retainer design had enough retention for anterior forces of occlusion. Most retainer failure occurred at retainer - composite resin interface.
� G. J. Livaditis and V. P. Thompson (1982)) �Described a technique for a retentive mechanism that etches the inner side of the cast fixed partial denture frameworks. They etched metal ceramometal restoration with 0 -5 N nitric acid was then bonded to the enamel surface utilizing the technique for acid etching enamel. �They suggested that improved resin bonded retainers provide innovative conservative and viable alternatives to traditional fixed prosthodontics
�Re G. J. et al (1988) �Compared three methods of etching metals for resin bonded bridges. Ni- Cr alloys were air abraded with 50μm alumina MET- ETCH Gel, Electrolytic etching with 10% sulfuric acid for 10 mins at 300 m. A and Silicoating were evaluated as surface treatments. �It was observed that silicoating with electrolytic etching gave superior results. MET- Etch Gel produced lowest shear strength
�TANAKA T. ET AL (1986) �studied the effect of oxidation of alloys on the bond strength of resin cements. Here two types of alloys Ni- Cr and Co – Cr alloys were used. Two samples were air brushed with 50μm alumina powder whereas others oxidized with an oxidizing agent. �A solution of 0. 3% sulfuric acid and 1% potassium per manganate forms an oxide layer thus increasing the adherence of resin cements. �It was shown that Ni- Cr alloys developed superior bond strength after sandblasting and oxidation but an equivalent strength was obtained with Co –Cr alloys by merely sandblasting and ultrasonic washing.
SUMMARY
REFERENCE �Herbert T. Shillingburg; S. Hobo; et al Fundamentals of fixed Prosthodontics. 3 rd Edition. �Joseph E. Ewing , Fixed Partial Prosthesis. 2 nd edition. � Planning and making crowns and bridges – 3 rd edition 1998 -Bernard GN Smith
�A. Damien Walmsley et al. Restorative Dentistry. �Stephen F Rosenstiel; Martin F Land; J Fugimoto. Contemporary Fixed Prosthodontics. 3 rd Edition. �W F P Malone; David L Koth; et al Tylman’s Theory and practice of Fixed Prosthodontics. 8 th Edition. �Inlays, crowns and bridges -Colin. R. Cowell � Fixed prosthodontics – Keith e. Thayer
� Fixed bridge prosthesis – 2 nd edition 1980 D. H. Roberts �Analysis of Fixed Prosthetic. Appliances in Patients living in the Metkovi} Region, Croatia-Acta Stomatol Croat, Vol. 38, br. 2, 2004. Dragutin Komar etal �Aust Dent J. 1989 Jun; 34(3): 209 -18. Resin bonded prostheses: clinical guidelines. �Int J Prosthodont. 2016 May-Jun; 29(3)Comparison of Metal-Ceramic and All-Ceramic Three-Unit Posterior Fixed Dental Prostheses: A 3 -Year Randomized Clinical Trial. Nicolaisen MH, Bahrami G, Schropp L, Isidor F.
�Resin bonded marryland bridges, alok kumar etal, journl of dental science and rehabilitation, april- une 2012, pg 63 -65
THANKYOU