General Approach of Haemostasis Lupus Anticoagulant Islamic University


 q Lupus anticoagulants (LA) are heterogeneous")

 should be")



 2. TTI (Tissue Thromboplastin")
 q The specificity of the APTT to LA")
 q The Tissue Thromboplastin Inhibition test utilizes a diluted")
 KCT is similar to APTT, the difference being that KCT")
 q The platelet neutralization procedure (PNP) is based on the")



 q d. RVVT : The test of choice")




FRAGMENT D-dimer is a fibrin degradation product (or FDP),")




- Slides: 28
General Approach of Haemostasis Lupus Anticoagulant Islamic University of Gaza
ANTIBODIES. q Anti-phospholipid antibodies are a heterogeneous family of autoantibodies that react with epitopes on proteins that are themselves complexed with negatively charged phospholipids. q The blood vessel problems can then lead to complications such as stroke, heart attack, and miscarriage. q The two most commonly measured kinds of Antibodies are: Lupus anticoagulant Anticardiolipin antibody
LUPUS ANTICOAGULANTS (LUPUS ANTIBODY, LA, OR LUPUS INHIBITORS) q Lupus anticoagulants (LA) are heterogeneous Ig. G or Ig. M autoantibodies which inhibit phospholipid-dependent assays of blood coagulation by binding to plasma phospholipid-binding proteins such as beta 2 glycoprotein I (β 2 -GPI) or prothrombin q Lupus Anticoagulant was found in patient with SLE. q Most patients with a lupus anticoagulant do not actually have lupus Erythematosus, and only a small proportion will proceed to develop this disease bleeding. q It is a prothrombotic agent, agent that is, presence of Lupus anticoagulant antibodies precipitates the formation of thrombi in vivo. q In vivo, it is thought to interact with platelet membrane phospholipids, increasing adhesion and aggregation of platelets; thus its in vivo prothrombotic characteristics.
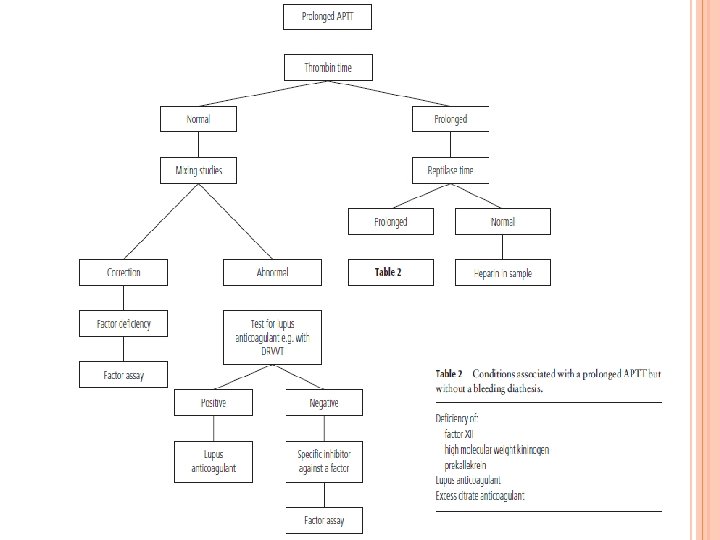
q q q The term "anticoagulant" accurately describes its function in vitro, but in vivo, it is now known that it functions as a coagulant Lupus anticoagulants impair the in vitro phospholipid dependent activation of factor X, factor IX, and Prothrombin. Presence of these antibodies causes an increase in a. PTT. The initial workup of a prolonged PTT is a mixing test. If the mixing test indicates an inhibitor, diagnosis of a lupus anticoagulant is then confirmed with phospholipid-sensitive functional clotting testing, such as the dilute Russell's viper venom time, time or the Kaolin clotting time The presence of an LA is usually not associated with a bleeding problem unless accompanied by o Thrombocytopenia, o Factor II deficiency, o Platelet dysfunction o Or drug administration (e. g. , aspirin).
q The ISTH recommends that the laboratory diagnosis of lupus anticoagulants (LA) should be carried out on double-centrifuged plasma following a four-step procedure adhering to these principles: Prolongation of a phospholipid-dependent coagulation test. Extrinsic (d. PT), Intrinsic (a. PTT, dilute a. PTT, KCT, colloidal silica clotting time), Final common pathway (d. RVVT, Taipan venom time, Textarin and Ecarin time) q Evidence of inhibitory activity on mixing tests. q Evidence of phospholipid dependence. Correction of the prolonged coagulation time after addition of excess phospholipid or platelets q Lack of specificity for any one coagulation factor Lack of specifi c inhibition of one coagulation factor (such as FVIII: C, FIX: C, or FXI). q
ANTI-CARDIOLIPIN ANTIBODIES. q Ther is many classes of anticardiolipin antibody, abbreviated as Ig. G, Ig. M, and Ig. A. q The anticardiolipin antibody is measured in an ELISA test. q The Ig. G type of anticardiolipin antibody is the type most often associated with complications. q Some lupus patients with very high Ig. M anticardiolipin antibody have a problem called hemolytic anemia, in which their immune system attacks their red blood cells.
ANTI-PHOSPHOLIPID ANTIBODY SYNDROME q APS is present if at least one of the clinical criteria and one of the laboratory criteria that follow are met: 1. Clinical criteria: vascular thrombosis or pregnancy morbidity 2. Laboratory criteria: Lupus anticoagulant present in plasma on two or more occasions at least 12 weeks apart. B. Anticardiolipin antibody, Ig. G or Ig. M positive in medium or high titer on two or more occasions at least 12 weeks apart C. Anti-β 2 GPl antibody, Ig. G or Ig. M present on two or more occasions at least 12 weeks apart. A. q The positive laboratory criteria and the clinical criteria should occur within 5 years of each other.
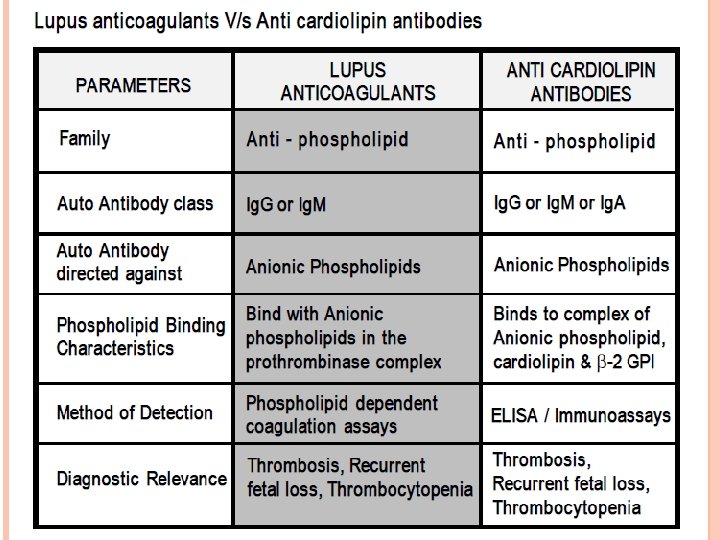
LABORATORY INVESTIGATIONS Immunological Individuals Assays with Lupus anticoagulants may also show the presence of other anti phospholipid antibodies. The most frequent finding is the presence of Anti- cardiolipin antibodies. The commonly employed method is the ELISA technique where the solid phase is coated with cardiolipin and β-2 GPI (as a cofactor). The ELISA method detects Ig. M, Ig. G and Ig. A class of anti-cardiolipin antibodies. An important point to note is that Lupus anticoagulants and anticardiolipin antibodies differ in their phospholipid-binding characteristic hence detection of anti cardiolipin antibodies is not specific for the presence of Lupus anticoagulants though they may be present in the same patient.
Clot based assays 1. APTT ( Activated Partial Thromboplastin Time) 2. TTI (Tissue Thromboplastin Inhibition test) 3. KCT (Kaolin Clotting Time) 4. PNP (Platelet Neutralization procedure) 5. Hexagonal Phase Phospholipids (Staclot-LA)
APTT ( ACTIVATED PARTIAL THROMBOPLASTIN TIME) q The specificity of the APTT to LA is reduced: q Different reagents have varying sensitivity for the presence of Lupus anticoagulants on the basis of their phospholipid composition ( variability of the test) q The APTT test is affected by the presence of inhibitors to Factor VIII, IX and XI. q The APTT test is also the test of choice for monitoring heparin therapy.
TTI (TISSUE THROMBOPLASTIN INHIBITION TEST) q The Tissue Thromboplastin Inhibition test utilizes a diluted PT reagent. The results are expressed as ratio of patient values to normal control values. q The TTI test is affected by numerous variables: 1. 2. 3. Species and tissue origin of thromboplastin can affect the test results as different sources of thromboplastin have varying sensitivity and responsiveness. Choice of “Normal” reference plasma is the most critical variable, because depending on the laboratory the choice of reference plasma could be lyophilized plasma, a frozen plasma pool or fresh plasma. The ratio of patient to normal can therefore change according to the choice of “normal” plasma. Some Ig. M Lupus anticoagulants do not prolong the TTI test
KCT (KAOLIN CLOTTING TIME) KCT is similar to APTT, the difference being that KCT reagent is devoid of phospholipids and incorporates Kaolin as contact activator. The test is performed on a range of mixture of normal and patient’s plasma. Different patterns of response are obtained indicating the presence of Lupus anticoagulants or the deficiency of one or more coagulation factors. The KCT test though sensitive is not specific for LA, additionally: • It cannot be automized • The test shows prolonged results with factor VIII, IX, XI & XII deficiency or corresponding inhibitors • The test is also highly sensitive for the presence of heparin.
PNP (PLATELET NEUTRALIZATION PROCEDURE) q The platelet neutralization procedure (PNP) is based on the ability of platelets to significantly correct in vitro coagulation abnormalities. q The disrupted platelet membranes present in the freeze-thawed platelet suspension neutralize phospholipid antibodies present in the plasma of patients with LA. q After the patient plasma is mixed with the freeze-thawed platelet suspension, the APTT will be shortened when compared with the original baseline APTT. But if an inhibitor is directed against specific coagulation factor, the clotting time is not shortened. q A correction of the baseline APTT of a defined amount of time (i. e. , 3 to 5 seconds or more) by the platelet suspension as compared with the control is indicative of the presence of an LA.
• • Due to limited stability the platelet preparations loose their activities on storage hence do not show reproducible results. They cannot differentiate between Lupus anticoagulants and Factor VIII inhibitors.
HEXAGONAL PHOSPHOLIPID NEUTRALIZATION ASSAY The hexagonal phospholipid neutralization assay uses the same principle as the PNP assay, assay normalization of the a. PTT in the presence of added phospholipid, but this assay specifically uses a phospholipid in a hexagonal conformation, Neutralization by this hexagonal form in an assay with a very lupus-anticoagulant sensitive a. PTT reagent, is a more sensitive confirmation test than the PNP. Comment Specimen collection, centrifugation, and processing are critical when testing for the presence of an LA. •
CONFIRMATORY TESTS FOR LUPUS ANTICOAGULANTS Confirmatory tests to identify an LA include those that utilize a low concentration of phospholipid in the test system, thereby increasing the LA effect such as The tissue thromboplastin inhibition test (TTIT), Dilute Russell's viper venom time (d. RVVT), And the kaolin clotting time (KCT), or Those that increase the phospholipid, thereby neutralizing the LA effect, such as the platelet neutralization
DILUTE RUSSELL’S VIPER VENOM TIME (DRVVT) q d. RVVT : The test of choice for screening and confirmation of LA – Indicating the phospholipid dependence of LA – Achieving maximum sensitivty for the precence of LA’s. q In general d. RVVT based tests comprise of: SCREENING REAGENT, containing limited amount of phospholipids with RVV (Russell’s Viper Venom) – CONFIRMATION REAGENT, containing additional phospholipids with same amount of Russell’s Viper Venom, to confirm the presence of phospholipid dependent Lupus anticoagulants. –
PRINCIPLE OF DRVVT FOR LA DETECTION Russell’s Viper Venom directly activates Factor V and X in presence of phospholipid and calcium ions, bypassing Factor VII of the extrinsic pathway and the contact and antihaemophilic factors of the intrinsic pathway. In normal plasma, in the absence of lupus anticoagulants, Factor V and X is directly activated by Russell’s Viper Venom, which in presence of phospholipid and calcium ion leads to clot formation.
In patients with LA, autoantibodies bind the epitopes of reagent phospholipids thereby preventing the activation of prothrombinase complex. This results in a prolongation of clotting time with SCREENING reagent. The CONFIRMATION reagent incorporates additional phospholipids to neutralize the LA. Once LA are neutralized clot formation proceeds relatively uninterrupted achieving a lower clotting time, to prove the phospholipids dependence of the autoantibodies.
INTERPRETATION OF RESULTS WITH DRVVT TEST • • • If SCREEN TIME is prolonged, to confirm the presence of lupus anticoagulants the plasma sample is tested with CONFIRMATION REAGENT. If CONFIRM TIME results shows a lower clotting time as compared to SCREEN TIME, it indicates the presence of phospholipid dependant Lupus Anticoagulants. Also the results can be expressed as ratio, The results expressed, as ratio is further useful in classifying the patient as normal, moderate, high and very high LA. If results of the ratio are borderline, mixing studies may be done further with the sample specimen. The mixing studies should be carried out with a 50: 50 mixture of test plasma and normal plasma.
General Approach of Haemostasis D-Dimer
D-DIMER (FRAGMENT D-DIMER; FIBRIN DEGRADATION )FRAGMENT D-dimer is a fibrin degradation product (or FDP), a small protein fragment present in the blood after a blood clot is degraded by fibrinolysis. It is so named because it contains two crosslinked D fragments of the fibrinogen protein. D-dimer test used to diagnose thrombosis, disseminated intravascular coagulation. The circulating enzyme plasminncleaves the fibrin gel in a number of places. The resultant fragments, "high molecular weight polymers", are digested several times more by plasmin to lead to intermediate and then to small polymers (fibrin degradation products or FDPs). The cross-link between two D fragments remains intact, however, and these are exposed on the surface when the fibrin fragments are sufficiently digested. The typical D-dimer containing fragment contains two D domains and one E domain of the original fibrinogen molecule
the D-dimer assay depends on the binding of a monoclonal antibody to a particular epitope on the D-dimer fragment. Several detection kits are commercially available; all of them rely on a different monoclonal antibody against D-dimer. Of some of these it is known to which area on the D-dimer the antibody binds. The binding of the antibody is then measured quantitatively by one of various laboratory methods. D-dimer testing is of clinical use when: There is a suspicion of deep Venous Thrombosis (DVT) Pulmonary Embolism (PE) Disseminated Intravascular Coagulation (DIC). It can also rise Postoperatively. It is under investigation in the diagnosis of Aortic Dissection
INTERPRETATIONS OF RESULTS A very high score, or pretest probability, a D-dimer will make little difference and anticoagulant therapy will be initiated regardless of test results, and additional testing for DVT or pulmonary embolism may be performed. For a moderate or low score, or pretest probability A negative D-dimer test will virtually rule out thromboembolism: the degree to which the D-dimer reduces the probability of thrombotic disease is dependent on the test properties of the specific test used in the clinical setting: most available D-dimer tests with a negative result will reduce the probability of thromboembolic disease to less than 1% if the pretest probability is less than 15 -20% If the D-dimer reads high, then further testing (ultrasound of the leg veins or lung scintigraphy or CT scanning) is required to confirm the presence of thrombus. Anticoagulant therapy may be started at this point or withheld until further tests confirm the diagnosis, depending on the clinical situation.
False positive readings can be due to various causes: liver disease, high rheumatoid factor, inflammation, malignancy, trauma, pregnancy, recent surgery as well as advanced age[citation needed] False negative readings can occur if the sample is taken either too early after thrombus formation or if testing is delayed for several days. Additionally, the presence of anti-coagulation can render the test negative because it prevents thrombus extension. Likelihood ratios are derived from sensitivity and specificity to adjust pretest probability.