GEBELK TAKB NASIL YAPILMALI RSKL GEBELK NE DEMEKTR

GEBELİK TAKİBİ NASIL YAPILMALI RİSKLİ GEBELİK NE DEMEKTİR Hazırlayan: Op. Dr. Kemal DİNÇ KADIN HASTALIKLARI VE DOĞUM UZMANI

Doğum öncesi bakımın amacı Gebelik, doğum ve doğum sonu dönemlerinin anne ve bebek yönünden sağlıklı geçirilmesini sağlamak, özelde aileye, genelde topluma sağlıklı bireyler kazandırmak.

GEBE TAKİBİNİ KİM YAPMALI VE NASIL YAPILMALI Aile Hekimliği Uygulama Yönetmeliği’nde yer alan görev yetki ve sorumluluklar kapsamında bu görev aile hekimlerinin primer görevleri arasında yer almaktadır.

GEBE TAKİBİNİ KİM YAPMALI VE NASIL YAPILMALI AİLE HEKİMLERİ KADIN DOĞUM UZMANLARI ÜNİVERSİTELER

DOĞUM ÖNCESİ BAKIMIN YÖNETİMİ • İyi iletişim • İzlemlerin zamanında, yeterli ve eksiksiz yapılması

İLETİŞİM • • Gebeyi nazik bir şekilde karşılama Gerekli mahremiyeti sağlama Kendini tanıtma Gebenin adını öğrenme ve kullanma Gerekli olumlu beden dilini kullanma İletişim için gerekli mesafeyi ayarlama Gebe ile yüze olma, göz teması kurma Her aşamada soru sorabileceğini belirtme

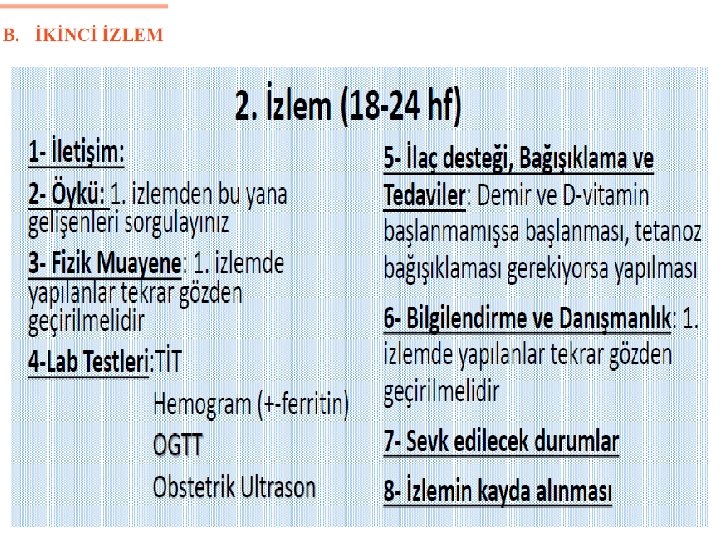
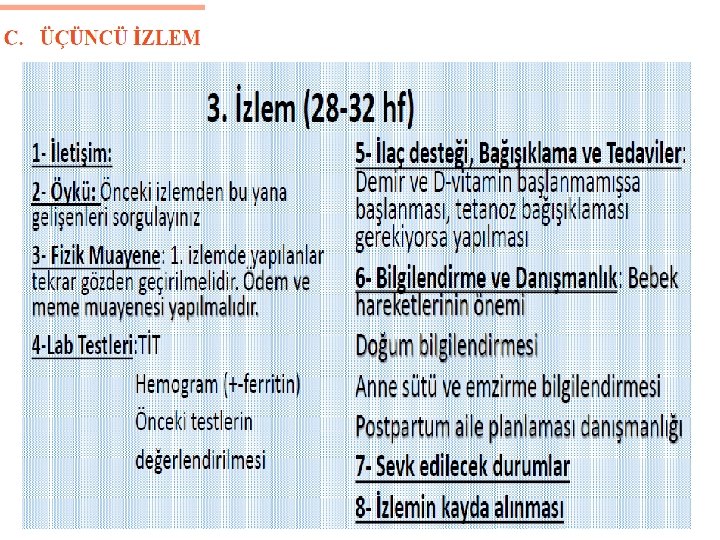
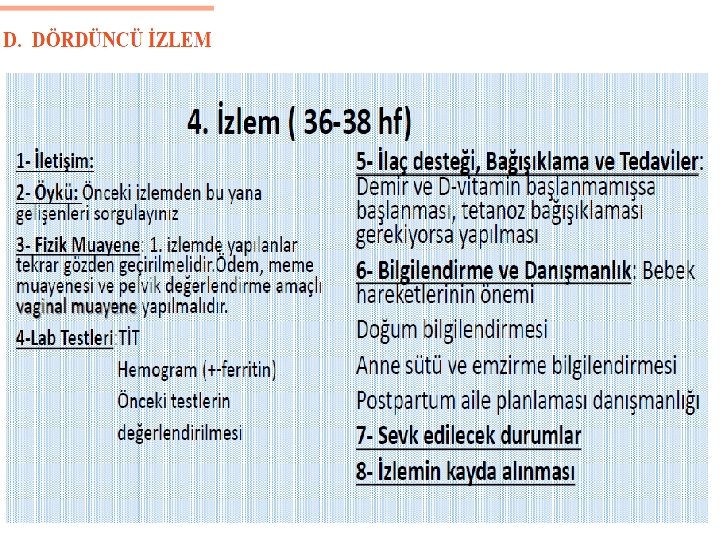
DOĞUM ÖNCESİ BAKIM TAKVİMİ • Gebenin en az bir bakıma eşi veya bir aile bireyiyle gelmesi teşvik edilmeli • Tüm gebeler en az 4 kez izlenmeli 1. izlem 2. izlem 3. izlem 4. aydan önce(14 hft ‘dan önce) 6. ayda(18 -24 hft arası) 8. ayda(30 -32 hft arası) 9. ayda(36 -38 hft arası) • Ciddi anemisi olanlar 2 haftada bir • Diğer riskli gebelikler (diyabet, preeklampsi vb. ) haftada bir • TDT bir hafta geçerse gebe sağlık kuruluşuna başvurmalı

n ÖYKÜ ALMA 1. 2. 3. 4. n Kişisel Tıbbi Obstetrik Mevcut gebelik FİZİK MUAYENE Risk değerlendirme formu doldurulacak n n n LABORATUVAR BAĞIŞIKLAMA ve İLAÇ DESTEĞİ BİLGİLENDİRME ve DANIŞMANLIK 1. 2. n Gebeliğe bağlı yakınmalar Genel İZLEM FİŞİNİN KONTROLU
 Yaş (Doğum tarihi) Adres")
Kişisel bilgileri • • • T. C Kimlik Numarası (biliniyorsa) Yaş (Doğum tarihi) Adres ve telefon numarası Medeni hali Akraba evliliği/derecesi – Birinci derece akraba (kardeş çocukları arasında) – İkinci derece akraba (kardeş torunları arasında) • • • Yaşadığı ev tipi, büyüklüğü ve hane halkı sayısı Yaşadığı mekanın alt yapı koşulları; tuvalet, su kaynağı Yaşadığı mekanın elektrik ve ısınma kaynağı Eğitim düzeyi Ekonomik kaynakları; – – – Kendi mesleği ve çalışma durumu Eşinin mesleği ve çalışma durumu Yaşadığı yerin en yakın sağlık kuruluşuna uzaklığı Ulaşım şartları Sosyal güvencesi

Tıbbi öykü-1 – Kronik sistemik hastalıklar (Diabetes Mellitus, hipertansiyon, kardiyovasküler hastalıklar, kr. böbrek hastalığı, epilepsi, tiroid hastalıkları vb. ) – Geçirilmiş veya tedavisi sürmekte olan enfeksiyon hastalıkları (Tüberküloz, Brucella, paraziter hastalıklar, vb) – CYBE öyküsü – Madde bağımlılığı – Toprak vb yeme – Psikiyatrik hastalıklar – Kan transfüzyonu – Talasemi taşıyıcılığı – Geçirilmiş operasyonlar – Geçirilmiş jinekolojik operasyonlar ( Histerotomi, myomektomi vb)

Tıbbi öykü-2 – İlaç allerjisi – Aile öyküsü (Diabetes mellitus, tekraralayan fetal anomaliler, çift yumurta ikizi vb. ) – Sürekli kullanmak zorunda olduğu ilaçlar (Antiepileptikler, insülin, antihipertansifler vb). • Madde bağımlılığı (sigara, alkol, uyuşturucu) Toprak vb. yeme – Gebelik öncesi kullanılan aile planlaması yöntemi – İnfertilite mevcut ise süresi, gördüğü tedaviler
 1 • • • Bu gebeliği dahil")
Obstetrik öykü (Daha önceki gebelikleri ile ilgili) 1 • • • Bu gebeliği dahil toplam gebelik sayısı ( Gravida) Daha önceki doğum sayısı (Parite) Yaşayan çocuk sayısı Son gebeliğin sonlanma tarihi-yeri Gebenin her gebeliği ile ilgili öyküsünün ve gebelik sonucunun irdelenmesi; • Doğumların kim tarafından nerede yapıldığı • Gebeliklerin sonlanma şekli ve gebelik haftası • Canlı doğum, ölü doğum, kendiliğinden düşük, isteyerek düşük, ektopik gebelik, mol gebelik • Bebek ölümü ve nedenleri • Çocuk ölümü ve nedenleri • Prematür doğum • Postmatür doğum • İkiz veya çoğul gebelik • Tekrarlayan birinci trimester düşükleri • Tekrarlayan ikinci trimester düşükleri • Yasal tahliye ve isteyerek düşük ve komplikasyonları
2 • Gebelik sırasında yaşanan komplikasyonlar (Kanama, preeklampsi, gestasyonel")
Obstetrik öykü (Daha önceki gebelikleri ileilgili)2 • Gebelik sırasında yaşanan komplikasyonlar (Kanama, preeklampsi, gestasyonel diyabet, tromboz, emboli) • Doğum sırasında yaşanan komplikasyonlar (Plasentanın erken ayrılması, plasenta previa, makat, transvers ve diğer prezentasyon anomalileri, uzamış doğum eylemi, üçüncü derece perine yırtıkları ve masif kanama, plasentanın elle çıkarılması ) • Doğumun şekli (Normal doğum, sezaryen doğum, forseps veya vakumla müdahaleli doğum) • Doğum sonrası dönemde yaşanan komplikasyonlar (Sepsis, kanama, depresyon, meme absesi vb. ) • Daha önceki canlı doğumlara ait yaşanan komplikasyonlar (Hidrops Fetalis, resüsitasyon veya başka tedavi almış yenidoğan, kromozomal anomali veya malformasyon, düşük doğum ağırlığı, intrauterin gelişme geriliği ve makrozomi) • Daha önceki canlı doğumlara ait bilgiler (cinsiyeti, doğum ağırlığı, anne sütü alma süresi) • Tetanoz toksoid immünizasyon uygulaması

Fizik Muayene • Gebenin boy ve kilosunu ölçünüz. • Kan Basıncını ölçünüz ( Sistolik kan basıncının 140, diastolik kan basıncının 90 mm. Hg altında olması normal kabul edilir) • Nabzını sayınız. • Ciddi anemi bulgularını kontrol ediniz El tırnakları, konjunktiva, ağız mukozasında solukluk, nefes almakta güçlük, 30’un üzerinde solunum sayısı • Hastalığı gösteren diğer tehlike işaretlerini kontrol ediniz Nefes darlığı, öksürük, yüksek ateş vb. • Gebelik haftası ile uterus büyüklüğünün uygunluğunu değerlendirmek • Semptomatik CYBE bulgusu varsa değerlendiriniz • Fetus kalp seslerini değerlendiriniz. Fetüs kalp atımları fetal steteskop ile 16 -20. , el Doppleri ile 10 -12. haftalardan itibaren duyulabilir • Bebeğin ilk hareketlerini hissetme zamanını kaydetmesini isteyiniz.
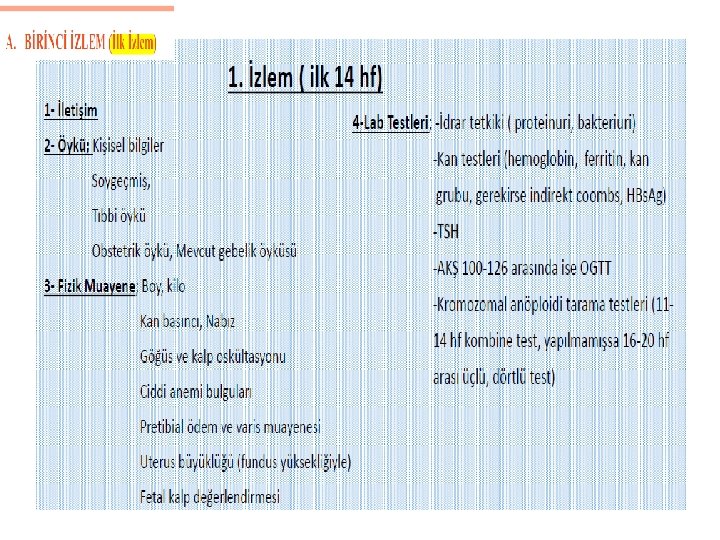

• Klavuza göre: Açlık Kan Glukozu, TİT, CBC, Ferrittin, HBs. Ag, TSH Kan Grubu (KG uygunsuzluğu varsa İndirect Commbs), • İdeal İlk Vizit Testleri: -CBC, Ferritin -BİYOKİMYA(Glukoz, BUN, Creatin, AST, ALT, LDH) -ELİZA (HBs. Ag, Anti-HBs, Anti-HCV, Anti-HİV) -TSH -TİT, İdrar Kültürü -Kan Grubu (KG uygunsuzluğu varsa İndirect Commbs),

İKİLİ TARAMA NEDİR DUYARLILIK %79 -87

DÖRTLÜ TARAMA DUYARLILIK %67 -81

DETAYLI ULTRASON 18 -24 HAFTALAR ARASI YAPILABİLİR -DAHA DETAYLI ÜLÇÜMLER ALINIR -ANOMALİ VARSA TESBİT EDİLİR -ASLA %100 HERŞEYİ GÖREMEYİZ ORGAN TARAMASI İLERİ DÜZEY USG AYRINTILI USG ANOMALİ TARAMASI

BAĞIŞIKLAMA

OGTT 75 GR ÖNERİLİR 24 -28 HAFTALAR ARASI YAPILABİLİR ANNE VE BEBEĞE KESİNLİKLE ZARARI YOKTUR

Fizik muayeneden sonraki aşamada risk değerlendirme formundaki sorgulamalar yapılmalı

• Risk değerlendirme formundaki kriterlerden birine bile “EVET”cevabı verilirse, mutlaka kadın doğum uzmanı bulunan bir sağlık kurumuna sevki yapılmalı • Uzman hekimce yapılan değerlendirme sonucunda izlemler birinci veya ikinci basamakta koordineli bir şekilde yapılmalı • İzlem sayısı ve sıklığının ne olacağı belirlenmeli

RİSK DEĞERLENDİRME FORMU • Bu risk değerlendirme formu “yüksek riskli gebeleri” saptamak için kullanılır; tüm gebelere uygulanır. • Bu form uzman görüşü alınarak izlem sayısı ve izlemin nerede, nasıl yapılacağı konusunda karar verilmesi içindir. • Risk değerlendirme formu sevk kriterlerini içermez.

RİSK DEĞERLENDİRME FORMU • A-Tıbbi Öykü • 1. Kardiyovasküler Hastalıklar • 2. Jinekolojik Hastalıklar: Pelvik Kitle, Myom, Uterin Malformasyon vb. • 3. Diabetes Mellitus • 4. Diğer Endokrin Hastalıklar: Hipotroidi, Hipertroidi, Guatr, Hiperlipidemi vb.

• 5. Epilepsi • 6. Diğer Serebrovasküler ve Nörolojik Hastalıklar: Anevrizma, Fistül vb. • 7. Psikiyatrik Hastalıklar: Depresyon vb. • 8. Kronik Hipertansiyon • 9. Solunum Sistemi Hastalıkları: Astım, KOAH vb. • 10. Renal Hastalıklar: Pyelonefrit, Nefrotik Sendrom, Kronik Böbrek Yetmezliği vb.

• 11. Hematolojik Hastalıklar: Orak Hücreli Anemi, Talasemi, Koagülasyon Bozukluğu vb. • 12. Enfeksiyon Hastalıkları: Tüberküloz, Sıtma, HBV, HCV, HIV, vb. • 13. Romatolojik Hastalıklar: Sistemik Lupus Eritematozus vb. • 14. Venöz Tromboemboli • 15. Neoplazmlar

• 16. Kalıtsal Hastalıklar: Konjenital Hastalıklar, Kas Hastalıklar, Metabolik Hastalıklar vb. • 17. Ortopedik bozukluk : DKÇ, Skolyoz vb. • 18. Akraba Evliliği • 19. ilaç Kullanımı ve Zararlı Madde Bağımlılığı: Sigara, Alkol vb. • 20. Düşük Sosyoekonomik Durum

B-Obstetrik Öykü • 1. GeçirilmiĢ Uterin Cerrahi: Sezaryen, Myomektomi, Metroplasti, Septum Rezeksiyonu vb. • 2. Pelvik Kitle, Myom, Uterin Malformasyon • 3. Tekrarlayan Düşük: 3 ve üzeri • 4. Düşük Doğum Ağırlığı 2500 gr. ↓ Öyküsü • 5. Makrozomik Bebek 4000 gr. ↑ Öyküsü • 6. Ölü Doğum, Yeni Doğan Ölümü • 7. Eklampsi-Preeklampsi Öyküsü • 8. Erken Doğum Öyküsü,

• • • 9. Postterm Doğum Öyküsü 10. Anomalili Bebek Öyküsü 11. Gestasyonel Diabetes Mellitus Öyküsü 12. Venöz Tromboemboli Öyküsü 13. Ektopik Gebelik Öyküsü 14. RH/rh Uygunsuzluğu 15. Antepartum ve Postpartum kanama Öyküsü 16. Zor ve Müdahaleli Doğum Öyküsü 17. Plasenta Previa , Plasenta Dekolmanı Öyküsü

C- Mevcut Gebeliğin Değerlendirilmesi • • • 1. 18 Yaş Altı 2. 35 Yaş Üstü 3. RH/rh Uygunsuzluğu 4. Çoğul Gebelik 5. iki Yıldan Sık Gebelik 6. Sigara , Alkol Kullanımı 7. Grandmultiparite: 5 ve üzeri doğum 8. Gestasyonel Diyabet 9. Plasenta Previa 10. Venöz Tromboemboli 11. Varis

• • • 12. Polihidramnios-Oligohidramnios 13. Anomalili Fetüs 14. Servikal Yetmezlik 15. Vajinal Kanama 16. Preeklampsi-Eklampsi 17. Gebelikte Cerrahi Müdahale Geçirilmesi: Appendektomi vb.

• • 18. Yatış Gerektiren Hiperemezis Gravidarum 19. Preterm Eylem 20. Gebelikte Travma Geçirilmesi 21. şiddetli Enfeksiyon 22. Ciddi Anemi 23. Preterm Erken Membran Rüptür (EMR) 24. Vücut Kitle Ġndeksi >30 kg/m 2 25. Vücut Kitle indeksi

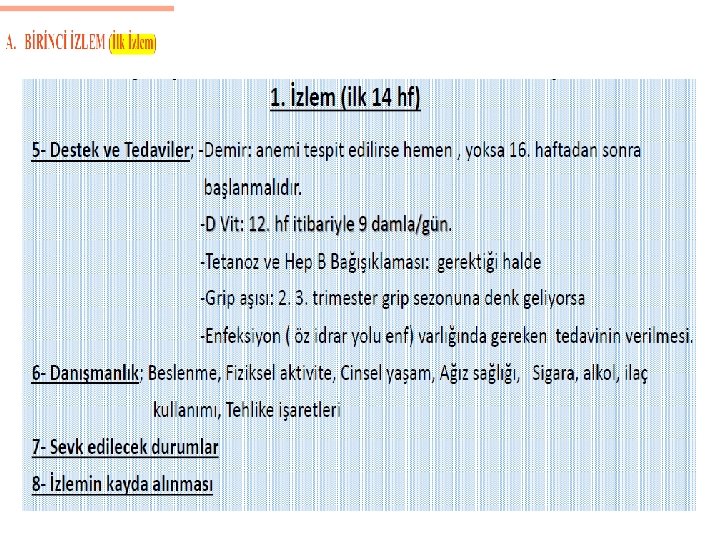
SEVK EDi. LECEK DURUMLAR • Hemoglobinin 7 gr/dl altında olması • Kanama ve lekelenme olması • Preeklampsi belirtileri, hipertansiyon ve/veya proteinüri olması • Uterus yüksekliğinin (fundus-pubis mesafesi) beklenen haftaya göre büyük veya küçük olması (± 4 cm. ) • Gebenin fetus hareketlerini hissetmemesi veya el doppleri ile fetal kalp seslerinin duyulmaması • Bakteriüri tespit edilen gebede tedaviye rağmen bakteriürinin devam ediyor olması • Tehlike işaretlerinin varlığı • Gebeliğe eşlik eden sistemik hastalıkların varlığı • Çoğul gebelik şüphesi olması

Gebelikte tehlike işaretleri Semptom Olası neden • Abdominal ağrı • Preterm eylem, ablasio plasenta • Enfeksiyon • Vücut ısısının 380 nin üzerinde olması • Baş dönmesi, bulanık görme, çift görme, lekeli görme • Sürekli kusma • Hipertansiyon, preeklampsi • Hiperemezis gravidarum

Gebelikte tehlike işaretleri Semptom Olası neden • Aşırı baş ağrısı • Hipertansiyon, preeklampsi • Elde, yüzde, bacaklarda ve ayaklarda ödem • Müsküler irritabilite, konvülsiyon • Epigastrik ağrı • Preeklampsi, eklampsi • Preeklampsi, abdominal damarlarda iskemi

Gebelikte tehlike işaretleri Semptom Olası neden • Oligüri • Renal hasar, yetersiz sıvı alımı • Üriner sistem enfeksiyonu • Annenin ilaç kullanımı, obesite, fetal ölüm • Dizüri • Fetal hareketlerin yokluğu

Riskli Gebelik: Tanım �Bir gebeliğin Anne ve Bebek açısından kötü sonuçlarının olma sıklığı, normal popülasyondan daha fazla ise; O gebelik RİSKLİ GEBELİK olarak adlandırılır. � RİSK; �Maternal �Fetal

Riskli gebelik nedenleri nelerdir? • Annenin 18 yaşın altında ya da 35 yaş üstünde olması • Annede hipertansiyon, tiroid hastalığı, Diabetes Mellitus, kalp, karaciğer, kollajen doku hastalıkları (lupus, sjogren vb) , damar ve diğer yapıları tutan hastalıklar gibi gebelik dönemine ait olmayan, gebe kalmadan önce zaten var olan sistemik hastalıklar var , • Annenin çok zayıf ya da çok şişman olması,

• Anne baba arasında akrabalık olması, • Annenin herhangi bir nedenle ilaç kullanıyor olması, (epilepsi, psikiyatrik hastalıklar vb) • Anne sigara ya da alkol kullanıyor ise, • Annenin tekrarlayan düşükleri var ise, • Annenin gebelik dönemi öncesinde hiçbir sağlık problemi olmamasına rağmen, hamile kaldıktan sonra tamamen gebeliğe bağlı olarak ortaya çıkan gebelik dönemi sorunları varsa

Fetusa bağlı gebelik dönemi sorunları • Çoğul ve ikiz gebelikler • Bebekte gelişme geriliği (IUGR) • Oligohidramnios • Polihidramnios • Rh İzoimmünizasyonu • Fetal anomaliler

Riskli gebelik takibi neden gereklidir? • Çoğu hamile anne gebelik dönemini herhangi bir sorun olmadan geçirmesine rağmen, gebelik dönemi süresince ne zaman sorunla karşılabileceğini öngörmek hamile anne için mümkün değildir. • Baştan çok normal görünen bir hamilelik döneminde bile sonradan ciddi sorunlar yaşanabileceği için, riskli gebelik olsun olmasın bütün hamileliklerin takip altında olması büyük önem taşır.

• Örneğin ; • Hamile kalmadan önce hiçbir hastalığı olmayan sağlıklı bir kadın hamile kalıyor; • Gebelik döneminin 24. haftasında (gestasyonel diyabet) ortaya çıkıyor. • Gebelik döneminin 28 ile 30. haftası itibariyle (preeklampsi ) ortaya çıkıyor. • Gebelik döneminin 28 ile 30. haftası civarında bebek gelişimi ile ilgili sorunlar (bebekte gelişme geriliği-İUGR) ortaya çıkıyor.

ÖNEMLİ • Prekonsepsiyonel bakımda “Risk Belirleme ve buna göre yönetim” esas olup, temel amaç olmalıdır.

Riskli Gebelik Takibi Esasları • İdeal: Prekonsepsiyonel risk belirlenmesi • Riskli gebelik değerlendirmesinde en azından ilk prenatal vizitte belirlenmesi • Spesifik hastalık neden ile ilgili branşlardan konsültasyon • Hasta ve Hasta yakını bilgilendirmesi • Gebelik devamı isteniyorsa risklerin anlatılıp onam formu alınması • Bireyselleştirilmiş takip çizelgesi oluşturulması

YAPMAMIZ GEREKEN NEDİR ÖNCELİKLE RİSKLİ GEBELERİ TESBİT ETMEK MUTLAKA BİR KADIN DOĞUM UZMANINA ULAŞMASINI SAĞLAMAK KADIN DOĞUM TAKİBİNE DÜZENLİ GİTTİĞİNİ KONTROL ETMEK
, Anti HBs negatif çıkan ve gebelik")
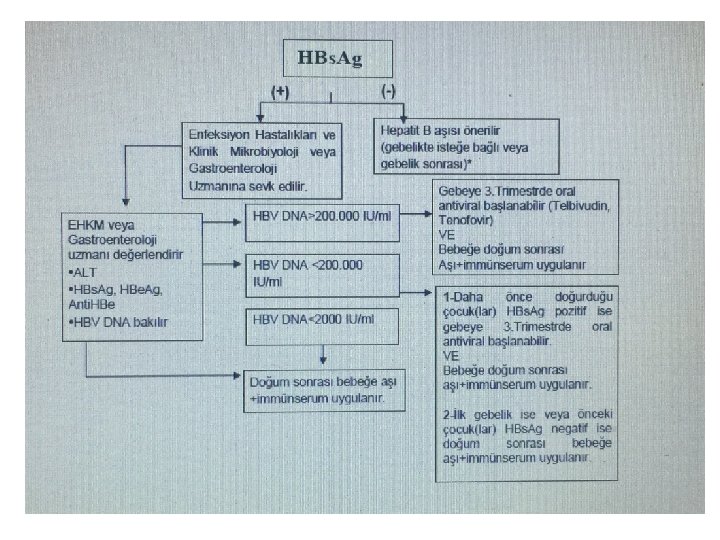
• Gebelikte yapılan tetkikte Hbs. Ag (-), Anti HBs negatif çıkan ve gebelik sırasında HBV ile enfekte olma riski bulunan gebelere; gebelik sırasında da (2. veya 3. trimesterde) hepatit B aşısı 0 -1 -6 ay aşı şemasıyla yapılabilir. Gebelikte aşılanmayan anneler doğumdan sonra aşılanabilir.
 GEBE KADINLARDAKİ TETANOZ AŞI TAKVi. Mi")
DOĞURGANLIK ÇAĞI (15 – 49 YAŞ) GEBE KADINLARDAKİ TETANOZ AŞI TAKVi. Mi

TEŞEKKÜRLER
- Slides: 61