GASTROINTESTINAL TRACT PHYSIOLOGY PHG 222 by ADEJARE A
 by ADEJARE, A. A. Department of Physiology Faculty of")
GASTROINTESTINAL TRACT PHYSIOLOGY (PHG 222) by ADEJARE, A. A. Department of Physiology Faculty of Basic Medical Sciences College of Medicine University of Lagos

OUTLINE • • General organization/functional anatomy of the GIT Review of smooth muscle function GIT motility GIT secretions and hormones Digestion and absorption of food substances Nutrition and metabolism GIT disorders

ANOREXIA • lack of appetite, could be from emotional or physical factors • lab tests to assess nutritional status • Medical treatment: • supplements may be ordered • Nursing Interventions: – oral hygiene, clean room, determine cause of nausea and treat, include family and friends, respect likes and dislikes, education

Paralysis of the swallowing mechanism – Cause: v. Damage to 5 th, 9 th, 10 th and 12 th CNs v. Poliomyelitis vencephalitis v. Deep anaesthesia – Symptoms: q. Swallowing fails to occur q. Epiglottis fails to close q. Posterior nares fail to close

Achalasia • Failure of LES to relax • S/S Ø Megaesophagus Ø Ulceration of the esophageal mucosa Ø Substernal pain Ø Death • Treatment Ø Intubation Ø Antispasmotic drugs
 • Causes: trauma, organisms, irritants, nutritional")
STOMATITIS • Inflammation of the oral mucosa (mouth) • Causes: trauma, organisms, irritants, nutritional deficiency, diseases, chemotherapy • S/S: swelling, pain, ulcerations, excessive salivation, sore mouth • Treatment: • pain relief, removal of causative factor, oral hygiene, medications, soft bland diet

GINGIVITIS • Inflammation of the gums • Causes: poor oral hygiene, poorly fitting dentures, nutritional deficiency • S/S: red, swollen, bleeding gums, painful • Treatment: dental hygiene, prevention of complications

ESOPHAGITIS • Inflammation or irritation of the esophagus • Causes: Reflux of stomach contents, irritants, fungal infections, trauma, malignancy, intubation • S/S: heartburn, pain, dysphagia • Treatment: treat underlying cause • Interventions: soft bland diet, administer meds, observe for complications

DISORDERS OF DIGESTION AND ABSORPTION • • • N/V Hiatal Hernia Gastritis Peptic Ulcer Stomach Cancer Obesity

DISORDERS OF DIGESTION AND ABSORPTION • N/V • Hiatal Hernia • Gastritis • Peptic Ulcer • Stomach Cancer • Obesity

NAUSEA AND VOMITING • Nausea: unpleasant sensation usually preceding vomiting, may have abdominal pain, sweating, • Causes: irritating food, infection, radiation, drugs, hormonal changes, surgery, inner ear disorders, distention of the GI tract

• Vomiting: forceful expulsions of stomach contents through the mouth. Occurs when vomiting reflex in the brain is stimulated. • Projectile vomiting- is forceful ejection of stomach contents. • Regurgitation- gentle ejection of stomach contents without nausea or retching

Complications and Treatment • May lead to dehydration, metabolic alkalosis, aspiration • Treatment: Antiemetics ( Phenergan, Dramamine, Scopolamine patch Reglan), IV fluids • Nursing care: through assessment, keep patient comfortable, offer liquids, position on side

HIATAL HERNIA • Protrusion of the lower esophagus and stomach upward through the diaphragm into the chest • Causes; weakness in the lower esophageal sphincter, related to increased abdominal pressure, long term bedrest, trauma

Signs and Symptoms • • Feelings of fullness dysphagia eruption regurgitation heartburn Complications: Ulcerations, bleeding, aspiration seen in 50% of people over 60.

Treatment for Hiatal Hernia • Drug therapy – H 2 receptor antagonists: Tagamet, Zantac, Pepsidreduce stomach secretions – Urecholine- increase LES tone – Antacids- neutralize stomach acids – Reglan, Propulsid - increase stomach emptying • diet therapy- decrease caffeine fatty foods, acidic and spicy foods

• SURGERY • Nissen Fundoplication • NURSING CARE: assessment, pain relief, watch for aspiration, nutrition, education

GASTRITIS • Inflammation of the lining of the stomach • ACUTE: excessive intake of food or alcohol. Food poisoning, chemical irritation, alcohol, aspirin • CHRONIC: repeated episodes of acute, H Pylori

In gastritis, the gastric barrier i. e. the adherent mucous and the tight junction between the epithelial cells of the stomach is destroyed The permeability of the barrier is thus increased. Diffusion of acid into the epithelium and susceptibility of the mucosa to digestion by the peptic digestive enzymes thus cause gastric ulcer

Signs/Symptoms and Complications • Nausea, vomiting, feeling of fullness, pain in stomach, indigestion. • With chronic may have only mild indigestion • changes in stomach lining and gastric atrophy would lead to achlorhydria or hypochlorhydria (decrease in acid) and intrinsic factor (high risk for pernicious anemia)

Treatment • Treat symptoms, and fluid replacement • Medications: antacids, H 2 receptor blockers, B 12 injections, corticosteroids analgesics, antibiotics if H Pylori • bland diet, frequent meals • Eliminate the cause • surgical intervention

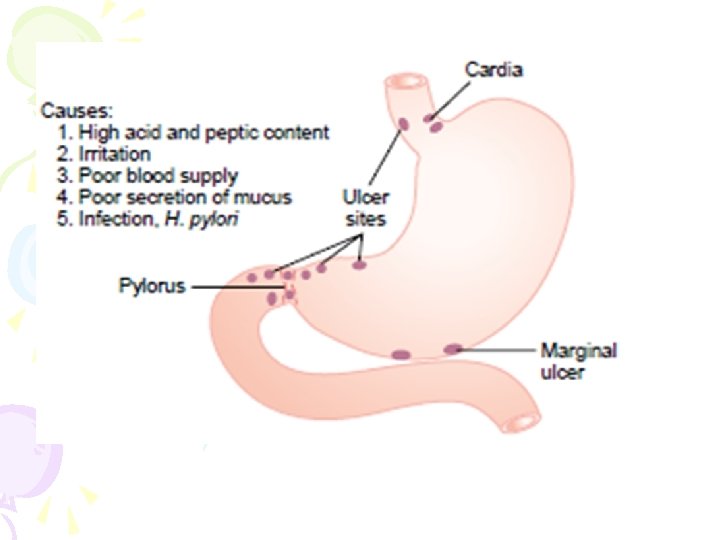
PEPTIC ULCER • Is an excoriated area of stomach or intestinal mucosa caused by the digestive action of gastric juice or upper small intestinal secretions • The defects often extend through the muscularis mucosa • Loss of tissue from the lining of the digestive tract. May be acute or chronic. • Aggressive factors: NSAIDS, H pylori, alcohol, bile salts, acid, pepsin • Other factors lifestyle factor, physiologic stress: increased BAO and MAO, genetic factors, accelerated gastric emptying

Protective mechanisms • • Ø Ø • • • Tight intercellular junctions Mucous glands: Compound mucous gland in the lower esophagus Mucous cell coating of the stomach mucosa, Pyloric glands Alkalinity of the small intestinal secretions Brunners glands in the upper duodenum: HCO 3 -, Pancreatic secretion Bile secretion Nervous control mechanisms Duodenogastric and hormonal inhibitory reflexes secretin PGE Mucosal blood flow Cellular restitution and epithelial renewal
")
Causes a peptic ulcer can be caused in either of two ways: • (1) excess secretion of acid and pepsin by the gastric • mucosa or (2) diminished ability of the gastroduodenal mucosal barrier • to protect against the digestive properties of the stomach acid–pepsin secretion juices. Classified as • gastric or • duodenal •

Peptic Ulcer comparison • Gastric Ulcers • burning pain 1 -2 hrs. after meals, upper left abd/back, relieved by food • N/V, anorexia, wgt loss • Shallow/ gastric secretions deceased • Older men, working class, bld type A, under stress • Duodenal Ulcers • burning/ cramping pain 2 -4 hrs. P meal, beneath xiphoid and back, relieved by antacids/food • increased gastric acid • Young men, all social classes, bld type O, chronic illnesses

PEPTIC ULCER COMPLICATIONS • HEMORRHAGE • PERFORATION • PYLORIC OBSTRUCTION

TREATMENT • Drug therapy – – – – – Antacids Stopping further use of NSAIDs Cimetidine, ranitidine H 2 RECEPTOR BLOCKERS ANTICHOLINERGICS-Pro-Banthine, Robinul, Bentyl, vagotomy, Surgical removal of gastrinomas omeprazole SUCRALFATE- Carafate Antibiotics –Flagyl, tetracycline, Biaxin • treatment goals- relieve symptoms, promote healing, prevent complications and recurrence

Physiological and pharmacological regulation of gastric secretion: the basis for therapy of acidpeptic disorders

Nursing Interventions • Three meals a day – decreases acid production • decrease foods that stimulate acid secretions and cause discomfort • treat pain with rest, diet and drug therapy • educate on stress management and relaxation

education • Reinforce diet • teach signs of complicatons • Avoid risk factors
, common in males, African American, over 70 and")
STOMACH CANCER • Rare(25, 000/yr. ), common in males, African American, over 70 and low socioeconomic status. 60% decrease in past 40 yrs. • No S/S in early stages • Late stages S/S: N/V, ascities, liver enlargement, abd. Mass • Mets to bone and lung • 10% survival rate after 5 yrs.

• Risk factors: pernicious anemia, chronic gastritis, cigarette smoking, diet high in starch, salted meat, pickled foods, nitrates • Treatment: surgery/ chemotherapy/ radiation – subtotal gastrectomy, total gastrectomy

OBESITY • Increase in body weight, caused by excessive fat. • Causes: heredity, body build, metabolism, psychosocial factors. Calorie intake exceeds demands. •

Treatment and nursing care • • Weight reduction diet drug therapy, mainly Amphetamines Surgical procedures: Nursing care-assessment, diet monitoring, education

Pancreatic failure • Failure of the pancreas to secrete pancreatic juice into the small intestine • Causes q Pancreatitis: acute or chronic: alcohol q Blockage of the papilla of Vater by a gallstone q Removal of head of pancrease during malignancy

Sprue • Means malabsorption by the small intestine following proper digestion • Types Ø Nontropical sprue/ gluten enteropathy: results from toxic effects of gluten present in some grains. Gluten destroys the microvilli of the enterocytes Ø Tropical sprue: caused by unidentified infectious agents in the tropics • Both leads to steatorrhea formation • Malabsorption of proteins, carbohydrates, calcium, vitamin K, folic acid, and vitamin B 12

• As a result, the person suffers • Severe nutritional deficiency • osteomalacia (demineralization of the bones because of lack of calcium); • inadequate blood coagulation caused by lack of vitamin K; and • Macrocytic anemia of the pernicious anemia type, owing to diminished vitamin B 12 and folic acid absorption.

Constipation • Slow movement of feces through the large intestine. • Cause ü Tumors ü Adhesions ü Ulcers ü Irregular bowel habit ü Spasm of small segment of the sigmoid colon • Can lead to megacolon/ Hirschsprung’s disease

Diarrhea • Results from rapid movement of fecal matter through the large intestine • Causes Ø Enteritis: inflammation of the enteron causing increased irritation and secretion of the mucosa. Ø There is also increased motility and propulsive movements of the colon Ø Cholera : • cholera toxin directly stimulates excessive secretion of electrolytes and fluid from the crypts of Lieberkühn in the distal ileum and colon.

Treatment Ø Replacement of fluid and electrolytes using IV solutions Ø Use of antibiotics • Psychogenic diarrhea: • Accompanies periods of nervous tension • Cause • Excessive stimulation of the PNS

FLATUS • Sources ü Swallowed air ü Gases formed from bacteria actions ü Gases that diffuse from blood to the GIT • Could be expelled by belching, lungs • Components: CO 2, CH 4, H 2 • Foods: beans, cabbage, onion

Thanks for your cooperation
- Slides: 43