Gastrointestinal System Jane Bordner RN BSN Nursing Instructor

Gastrointestinal System Jane Bordner, RN BSN Nursing Instructor HACC, Central Pennsylvania’s Community College N 100 Spring 2015

Anatomy and Physiology

GI Tract Flexible, hollow, muscular tube 26 feet Lined with mucous membrane
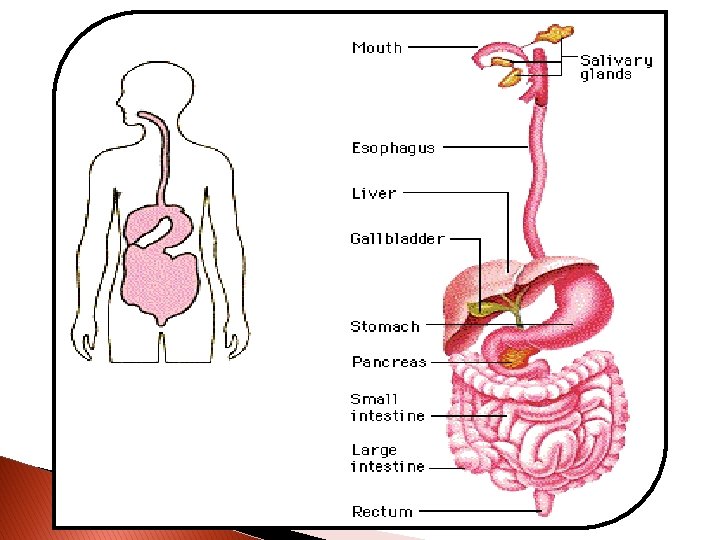

Digestion Principle responsibility of GI tract Occurs in mouth, stomach, and small intestines Majority in small intestines

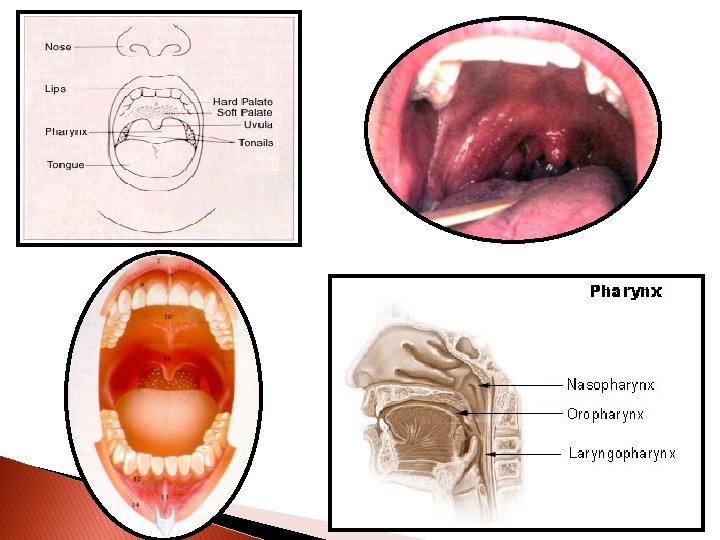
Oral Cavity Teeth break food into smaller pieces Saliva dilutes and softens bolus of food Amylase begins chemical break down Tongue: ◦ ◦ Made of skeletal muscle Contains taste buds Keeps food between teeth Elevates to move food back into pharynx

Pharynx Passage of food from oral cavity to esophagus Muscular tube Constrictor muscles that contract as part of swallowing

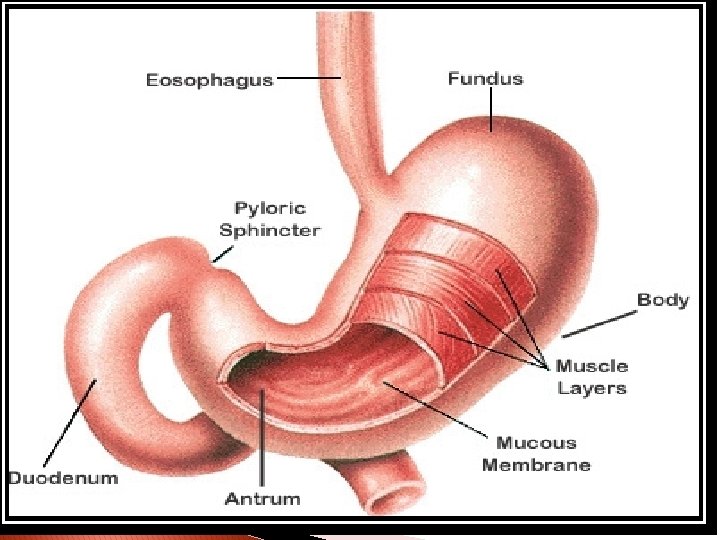
Esophagus Carries food from pharynx to stomach No digestion Food passes through upper esophageal sphincter Peristalsis pushes food through cardiac sphincter

Stomach Tasks Produces and secretes ◦ Storage ◦ Mixing ◦ Emptying ◦ Hydrochloric Acid (HCl) ◦ Pepsin ◦ Mucus ◦ Intrinsic factor

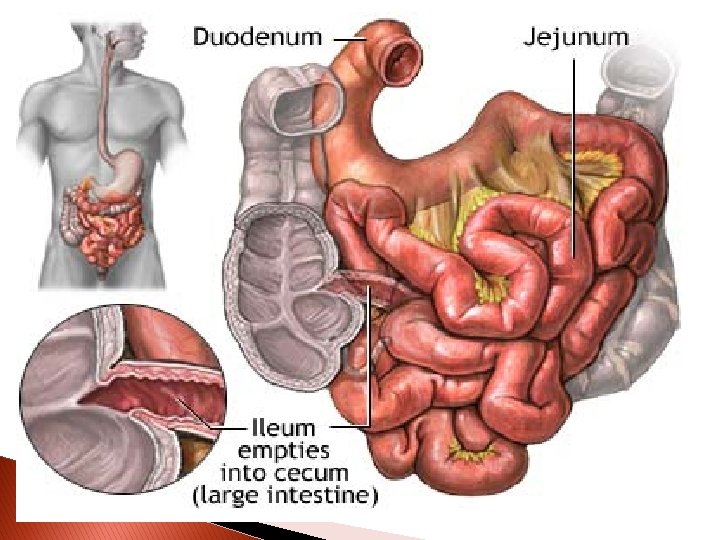
Small Intestine Segmentation Peristalsis 7 to 10 L of liquid moves through in one day Chyme is reduced to a volume of 600 to 800 ml that is paste-like consistency

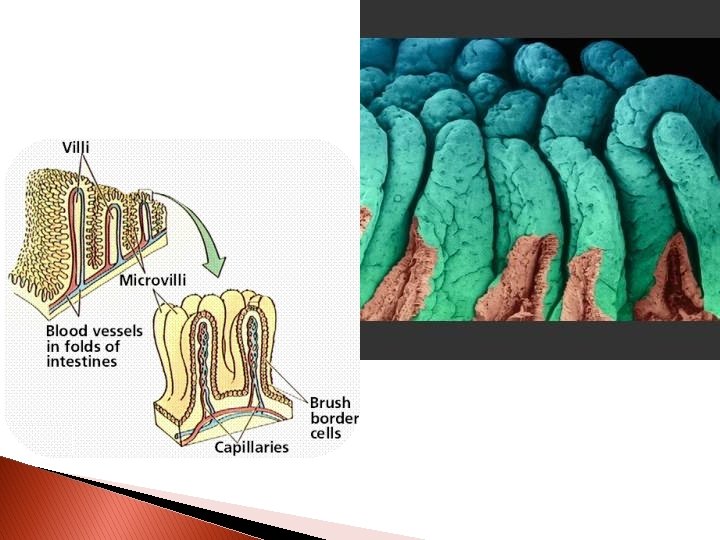
Small Intestine 3 Sections: ◦ Duodenum – 2 feet long Continues to process chyme ◦ Jejunum – 5 feet long Absorption of CHO and protein ◦ Ileum – 12 feet long Absorption of H 2 O, fat, and bile salts Most nutrients and electrolytes are absorbed

Small Intestine Impaired function Digestive process is altered ◦ Conditions such as Inflammation Ulceration Surgical resection Obstruction

Large Intestine Lower GI tract/Large Colon Bowel elimination Larger diameter 5 to 6 feet in length 3 sections ◦ Cecum ◦ Colon ◦ Rectum

Large Intestine Chyme enters through ileocecal valve Cecum is 1 st part Colon sections ◦ ◦ Ascending Transverse Descending Sigmoid Rectum and Anal Canal

Large Intestine 4 Functions ◦ Absorption H 2 O Na & Cl ◦ Protection bacteria ◦ Secretion Bicarbonate and K ◦ Elimination Bulk waste

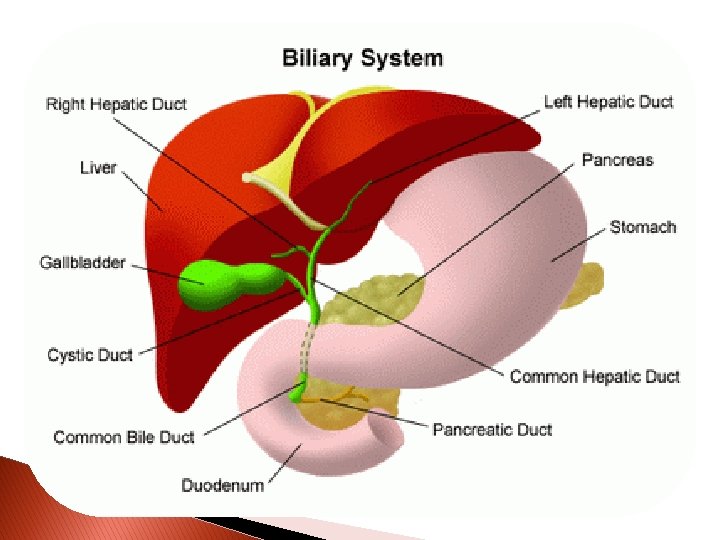
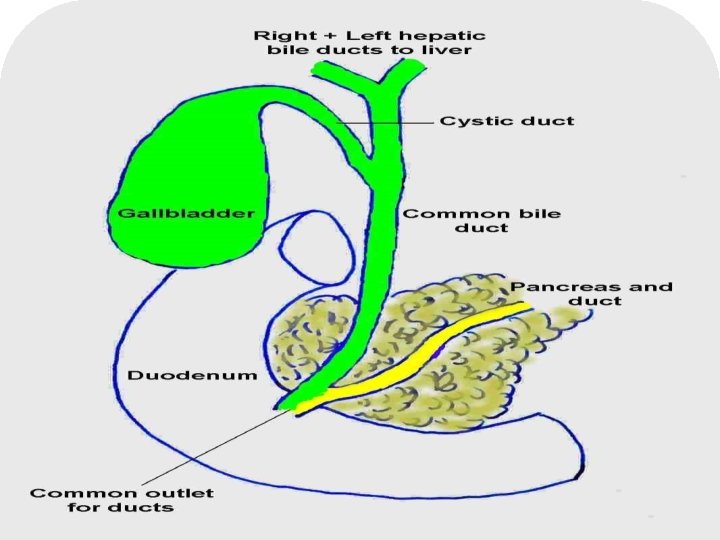
Accessory Structures of Digestion Pancreas Liver Gall bladder

Pancreas Gland Posterior to stomach Exocrine = secretes pancreatic juices ◦ Amylase = CHO ◦ Lipase = Fats ◦ Trypsin = Protein and bicarbonate Endocrine

Pancreatic Duct

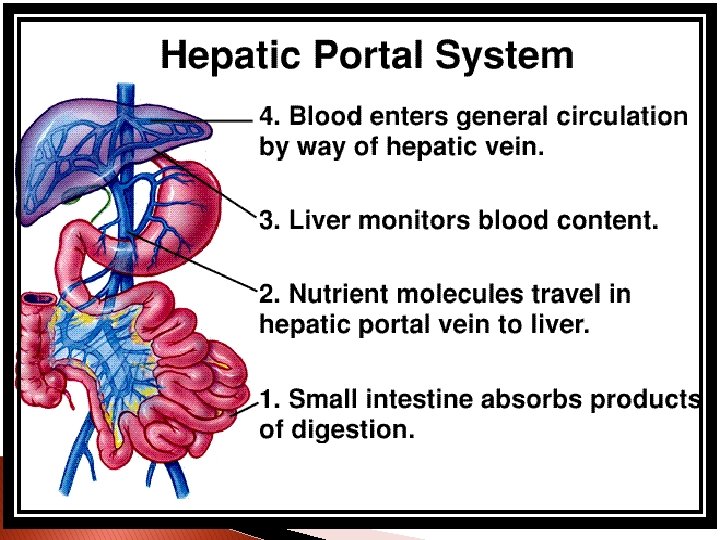
Liver Largest organ in body Remarkable and complex O 2 rich blood received through hepatic arteries Nutrient rich blood received through portal vein 2 lobes

Liver Functions Secretes bile Produces bilirubin Removes nutrients from blood Stores vitamins and iron Converts glucose to glycogen Stores glycogen

Liver Functions Converts excess fatty acids and urea Helps metabolize proteins, fats, and CHO Detoxifies drugs and poisons Phagocytizes bacteria and old RBC’s
 ◦ secreted by intestinal mucosa")
Gall Bladder Stores and concentrates bile Hormone CCK (cholecystokinin) ◦ secreted by intestinal mucosa ◦ stimulates gall bladder to contract and release bile

Factors that Affect GI Function Disease process Chemical/physical trauma Social/economic factors Stress/emotional factors Congenital defects Aging process

Assessment
 Inspection (LOOK) Auscultation (LISTEN) Palpation (FEEL)")
Assessment of GI Status History (SUBJECTIVE AND OBJECTIVE) Inspection (LOOK) Auscultation (LISTEN) Palpation (FEEL) Percussion

History W H A T S U P - Where is it? How does it feel? Aggravating and alleviating factors? Timing? Severity? Useful other data? Patient perception of problem? Also include medications, nutritional assessment, family history, cultural influences, height and weight
")
Inspection (LOOK)
")
Auscultation (LISTEN)
 RUQ RLQ LUQ LLQ")
Palpation (FEEL) RUQ RLQ LUQ LLQ

Percussion

Diagnostic Studies

Radiological Exams Obstruction Series Upper GI/Barium Swallow Lower GI/Barium Enema

Upper GI Series

Lower GI/Barium Enema

Patient Prep ◦ ◦ ◦ Light, low fat, low residue diet for 2 days Clear liquid dinner evening before NPO after midnight Stimulant laxative night before Enemas until clear or Colyte/Golytely prep **Bowel must be clean of stool for accurate results**

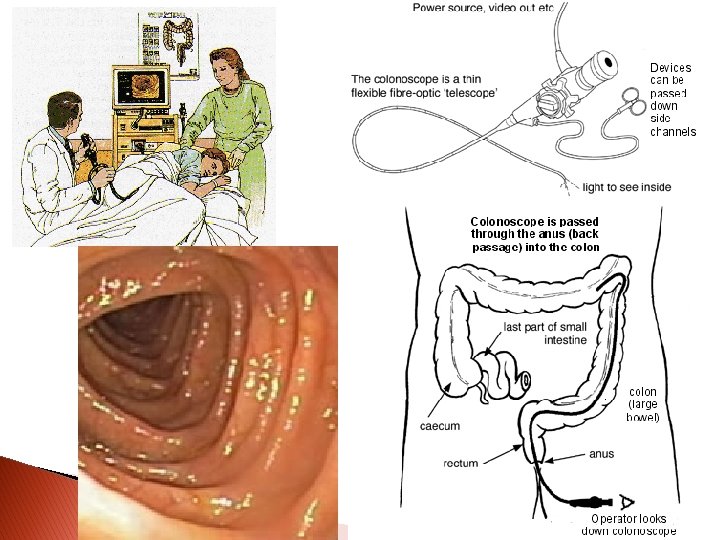
Endoscopy – Flexible scope EGD ERCP Sigmoidoscopy/Colonoscopy
 � Eliminates need for exploratory surgery � Collection of biopsy material �")
EGD (Esophagogstrodudenscopy) � Eliminates need for exploratory surgery � Collection of biopsy material � Remove foreign objects � Preparation ◦ NPO 6 to 12 hours before ◦ Use of local anesthetic to control gag reflex � Post-procedure ◦ NPO until gag reflex returns ◦ Watch for signs of perforation and/or bleeding post-op
")
ERCP (Endoscopic Retrograde Cholangiopancreatography)

Sigmoidoscopy/Colonoscopy Visualize colon and sigmoid area Empty bowel prior to test ◦ Bowel Prep 2 day prep (outpatient) Clear liquid diet for 1 - 2 days Enema until clear or Go-lytley prep ◦ IV sedation may be used during procedure ◦ Patients find this test intrusive
")
CT Scan More sensitive than x-ray Non-invasive, no pain May prep with contrast (clear)

MRI Extremely sensitive Visualizes changes in structure and tissue

Ultrasound Outlines borders of structures ◦ liver, pancreas, gall bladder
 Bilirubin Ammonia")
Laboratory Studies Amylase and lipase blood levels Liver enzymes (AST, ALT, LDH) Bilirubin Ammonia ◦ Pancreatic function ◦ Liver function ◦ Breakdown of RBC’s ◦ Liver function

Laboratory Studies Albumin Prothrombin time Gastric Analysis Stool Exams ◦ Liver function ◦ p. H ◦ ◦ ◦ Infection, parasites, organisms Hemoccult (guaiac) Consistency Color Odor

GI System Review Anatomy and Physiology

Where is the cardiac sphincter located? Where is the pyloric sphincter located? Where is the ileocecal valve located? List the 3 segments of the small intestine ◦ _____________________ ◦ ___________ Where does most absorption of nutrients take place?

List 5 digestive juices and the organs that secrete them ◦ ◦ ◦ _________________ ___________________ ___________________ Which nutrients enter the blood stream directly? Which nutrients enter the lymph system first? Describe peristalsis

List exocrine function of pancreas List function of gall bladder List functions of liver ◦ ◦ ◦ ◦ ___________________________________________ ___________________________________________
")
Therapeutic Uses of Salem Sump Tube Remove gas and fluids from stomach (decompression) Obtain gastric secretions for analysis To relieve/reduce obstructions or bleeding Promote healing after surgery – prevent strain on sutures Remove toxic substances (lavage with poisonings)

Assessing Placement Ask client to speak Inspect pharynx Instill 15 – 30 ml of air while listening over stomach Aspirate gastric contents ◦ Assess color ◦ Assess p. H Gastric secretions: < 4

Assessing Drainage Irrigation

Total Parenteral Nutrtion Intravenous hyperalimentation o Burns, trauma, malnutrition, cancer o

Common Problems Constipation Impaction Diarrhea Flatulence Incontinence Hemorrhoids Gastritis Gastric Ulcer Disease GERD

Constipation Decreased BM Hard, dry stool Causes Nursing Interventions

Constipation Nursing Diagnosis Goal Interventions Who is at risk? ? ?

Fecal Impaction Risk factors S&S ◦ ◦ History of constipation Chronic confusion Comatose Weak and debilitated ◦ ◦ ◦ No BM for several days Distended abd. Anorexia/Nausea/Vomiting Oozing of diarrhea stool Feel hard fecal mass with digital exam

Fecal Impaction

Constipation Treatment Stimulants Stimulates peristalsis Pulls fluid into stool Used for bowel prep Used for acute constipation ◦ Side Effects Pain/cramps Diarrhea Dehydration ◦ Examples magnesium citrate Milk of Magnesia (MOM) Senokot (sennosides) Dulcolax (bisacodyl)
")
Stool Softeners Increase water in stool Prevents straining Side Effects ◦ Colace (docusate sodium)

Bulk-Forming Laxatives Increase stool mass and water content Prevent and treat simple constipation Side Effects ◦ Metamucil (psyllium) ◦ Fiber. Con/Fiber-Lax (polycarbophil) ◦ Always give with 8 ounces of fluid

Lubricants Create slippery barrier between stool and intestinal wall Softens impacted stool ◦ Fleets Mineral Oil

Osmotics Uses osmotic pressure to draw water into stool Used for bowel cleansing or occasional constipation ◦ Colyte/Go-Lytely (polyethylene glycol/electrolyte) ◦ Miralax (polyethylene glycol) ◦ Fleet Enema, Fleet Phospho-Soda (phosphate/biphosphate Side Effects

We know that it’s a problem Song That we all too often see. It may go on for several days Sometimes it worries me Yes, it’s a private matter But I can clearly see We just don’t do enough ‘bout constipation. We listen to heir bowel sounds and we ask them how they feel We make sure they have lots to drink with each and every meal. I hate to have to say it, but I very firmly feel: We just don’t do enough ‘bout constipation! I’d like to say a word on our behalf. Constipation is a pain in the …… How do you help the soul with constipation? How do you keep their bowel from standing still? How do you treat the soul with constipation? An enema? A suppository? A pill? Many a thing you know you’d like to tell them Many a thing they ought to understand But how do you make them stay and listen to all you say? How do you make them comply with the plan? Oh how do you help the soul with constipation? We must prevent impaction if we can! When they’re rushed and when they’re hurried When they’re stressed and when they’re worried And they don’t eat a healthy foods they way they should Then they come in when they’re sick, And their bowels don’t move a lick Then we give them opioids, O that’s not good! “cuz it slows down their digestion, causing problems without question But they need it for their pain and that’s a fact. So we give them Senekot, some will take it, some will not, document it when they go and what you got!! (REPEAT CHORUS)

http: //www. sunnycorner. com/movies/f eatured/som/music/mariasom. php

Diarrhea Increased number of BM’s Loose, unformed stools Risk for fluid and electrolyte imbalance Risk for skin breakdown

Diarrhea Nursing Diagnosis Goal Interventions
 Imodium (lopermide)")
Anti-Diarrheal Medications Systemic Anti-Diarrheal Agents ◦ Decrease peristalsis Lomotil (diphenoxylate & atropine) Imodium (lopermide) ◦ Side effects Constipation Fatigue Locally-Acting Agents ◦ Absorbs water from stool Kaopectate (bismuth subsalicylate)

Incontinence Inability to control passage of feces and/or gas Causes Impact Body image, disturbed Risk for skin breakdown Nursing Interventions Bowel schedule Meticulous skin care

Flatulence S&S Abd. pain Abd. distention SOA Nursing Interventions Increase mobility Limit carbonation Comfort measures

Hemorrhoids Nursing Interventions Assess size, color and bleeding Prevent constipation Comfort measures

Nausea and Vomiting Nausea – subjective feeling of urge to vomit Vomiting – expelling stomach contents May cause fluid and electrolyte imbalance Treat cause

Nursing Interventions for N&V Protect airway Monitor fluid and electrolyte balance Provide replacement fluids (po and/or IV) Prevent further N&V Administer Antiemetics

Nursing Diagnosis for N&V Diagnosis Goal Interventions
 ◦ Phenergan (promethazine) Side Effects")
Phenothiazines Inhibit dopamine receptors in brain ◦ Compazine (prochlorperazine) ◦ Phenergan (promethazine) Side Effects ◦ ◦ Dry eyes and mouth Constipation Confusion and sedation Extrapyramidal reactions

5 -HT 3 antagonists Blocks effects of serotonin at receptor sites in vagal nerve and chemoreceptors in CNS ◦ ◦ Anzetmet (dolasetron) Zofran (ondansetron) Side Effects ◦ ◦ ◦ Headache Constipation Diarrhea
 Anivert (meclizine) Inhibits vestibular stimulation Used for motion sickness Side effects ◦")
Dramamine (dimenhydrinate) Anivert (meclizine) Inhibits vestibular stimulation Used for motion sickness Side effects ◦ Drowsiness ◦ Anorexia
 Blocks dopamine Increases GI motility Prevention of chemo induced N&V Tx of")
Reglan (metoclopramide) Blocks dopamine Increases GI motility Prevention of chemo induced N&V Tx of gastric stasis and post-op N&V Side effects ◦ Drowsiness ◦ Restlessness ◦ Extrapyramidal reactions
 CNS depressant and histamine 1 receptor blocker Used as adjunct to opioid")
Vistaril (hydroxyzine) CNS depressant and histamine 1 receptor blocker Used as adjunct to opioid analgesic Side effects ◦ Drowsiness ◦ Dry mouth ◦ Pain at injection site

Gastritis Inflammation of stomach lining Abd. Pain, nausea and anorexia Interventions ◦ ◦ ◦ Bland diet/soft food (no caffeine, spicy food) No smoking Antacids Medication to decrease stomach acid Antiemetics
 in mucosal wall of esophagus, stomach or")
Peptic Ulcer Disease Loss of tissue (erosion) in mucosal wall of esophagus, stomach or duodenum Referred to as ◦ Gastric ◦ Duodenal ◦ Esophageal ◦ Stress

Peptic Ulcer Disease Ulcers may extend deeply into muscle layers or through muscle to peritoneum ◦ Etiology Poorly understood H. pylori bacteria May be acute or chronic
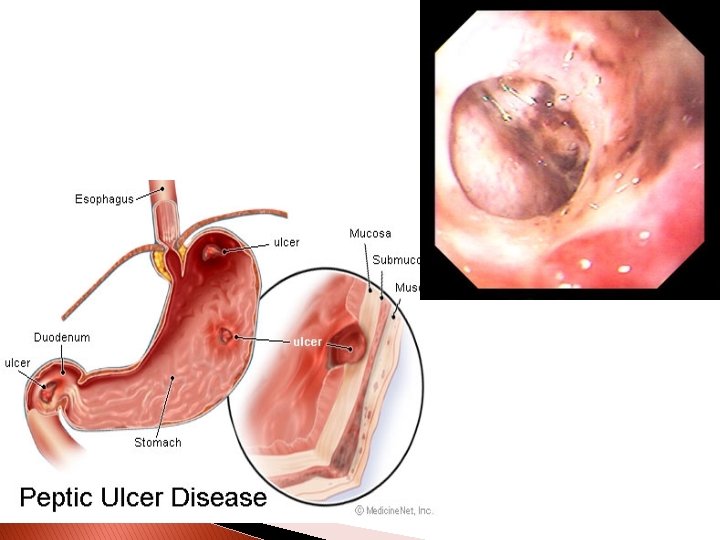

Peptic Ulcer Disease S&S ◦ Sharp, burning, gnawing, midepigastric pain ◦ Pain occurs 1 -3 hours after meals or with meals ◦ Heartburn and belching ◦ Melena or Hematemesis

Peptic Ulcer Disease Diagnosis ◦ Urea breath test ◦ Ig. G antibody for H. pylori infection ◦ Upper GI ◦ EGD ◦ Gastric secretion analysis ◦ Stools for occult blood (Melena) ◦ Gastrocult/Hematemesis

Peptic Ulcer Disease Management ◦ Diet ◦ Rest ◦ Stress reduction ◦ No smoking or ETOH use ◦ Medication

GERD Back flow of stomach contents into esophagus Incompetent cardiac sphincter S&S ◦ Burning pain in esophagus Diagnosis ◦ Clinical S&S ◦ EGD
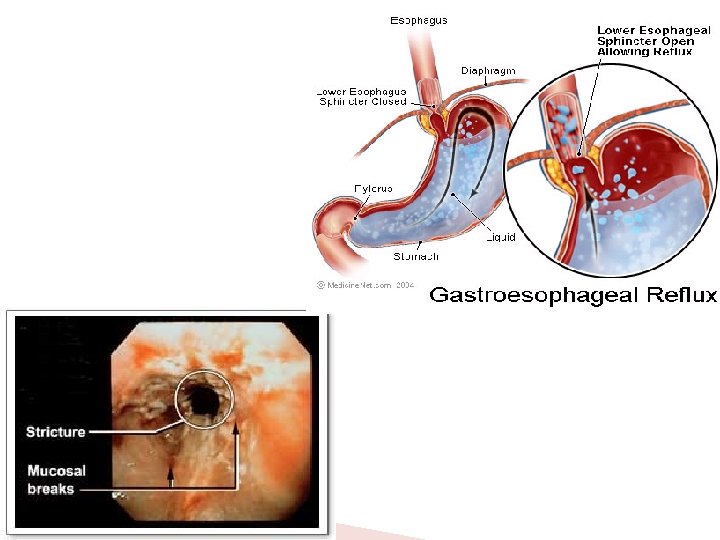

GERD Potential complications ◦ Esophagitis ◦ Esophageal stricture ◦ Esophageal ulceration ◦ Barrett’s Esophagus ◦ Esophageal Cancer

GERD Treatment ◦ Elevate HOB ◦ Avoid acid-stimulating foods ◦ Antacids ◦ Histamine blockers (H 2 receptor antagonists)

Gastric Medications

Antacids � � 1 st line for GERD Buffers HCL acid ◦ Maalox (magnesium & aluminum hydroxide) ◦ Mylanta (magnesium & aluminum hydroxide) ◦ Riopan (magaldrate) � Side Effects

Low-dose Histamine H-2 Antagonist Inhibits action of histamine at H 2 receptor sites in gastric parietal cells 2 nd choice for GERD Tx of peptic ulcer disease ◦ ◦ Zantac (ranitidine) Pepcid (famotidine) Tagamet (cimetidine) Axid (nizatidine) Side effects Confusion Decrease in WBC and RBC
 Inhibit gastric secretions by blocking the effect of histamine or")
H 2 inhibitors (Blockers) Inhibit gastric secretions by blocking the effect of histamine or acetylcholine on receptors found in parietal cells Tagamet Zantac Pepcid

Proton-Pump Inhibitors ◦ ◦ ◦ 3 rd choice for GERD Tx of duodenal ulcers Prevention of GI bleeding in critically ill ICU pt. Binds to an enzyme on gastric parietal cells in presence of acidic gastric p. H, preventing final transport of H ions into gastric lumen Prilosec (omeprazole) Prevacid (lansoprazole) Nexium (esomeprazole) Acip. Hex (rabeprazole) Side effects Diarrhea Abdominal pain Rash (allergic reaction)

Proton Pump Inhibitors Bind to an enzyme in the presence of acidic gastric p. H, preventing final transport of hydrogen ions into the gastric lumen Prilosec Prevacid
 Tx of pathological gastric")
Gastric Acid Pump Inhibitor Used for severe GERD (Big guns) Tx of pathological gastric hypersecretory disorders Adjunct tx of duodenal ulcers (Unlabeled) Same as proton-pump inhibitors ◦ Protonix (pantoprazole)
 Forms")
GI Protectant � � � Tx/prevention of duodenal ulcers Tx of GERD (Unlabeled) Forms a complex that adheres to ulcers; protecting and promoting healing ◦ Carafate (sucralfate) ◦ ◦ Constipation Dry mouth Side Effects Take on empty stomach

GI Prostaglandin ◦ ◦ ◦ ◦ Increased prostaglandin decreases gastric acid and pepsin secretion and increases protective mucus production Use for patient on NSAIDS and ASA Cytotec (misoprostol) Side Effects Diarrhea Abdominal pain Miscarriage

Antibiotics Tx H. pylori Usually combo of 1 – 2 antibiotics with proton pump inhibitor &/or H 2 antagonist ◦ ◦ Amoxil (amoxicillin) Biaxin (clarithromycin) Flagyl (metromidazole) tetracycline

Nursing Diagnosis for PUD Nursing Diagnosis Goal Interventions

Miscellaneous Topics

Pathology of GI Tract Obstruction Hemorrhage Perforation Neurological Inflammation Neoplasms

Intestinal Stomas Intestinal Stoma = artificial opening in abdominal wall Types Assessment Care ◦ Colostomy ◦ Ileostomy ◦ Stool ◦ Stoma ◦ Soap and water
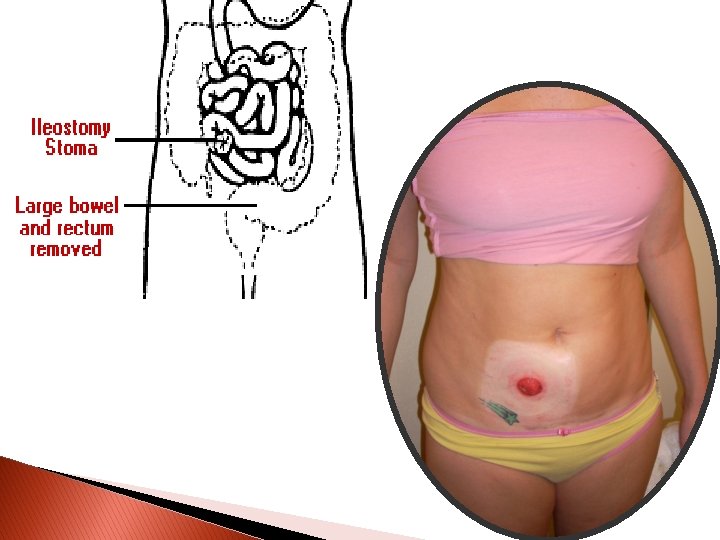

Intestinal Stomas Colostomies And Ileostomies ◦ Patient may lose up to 1000 ml/day of fluid through ileostomy ◦ Patients should avoid high fiber foods because of increase in GI transit time ◦ May be temporary or permanent


Stoma picture Ileostomy Descending colostomy Transverse colostomy Ascending colostomy Sigmoid colostomy


Nursing Diagnosis

Nursing Care
- Slides: 122