GASTROINTESTINAL BLEEDING CLASSIFICATION Upper GI Bleeding proximal to

GASTROINTESTINAL BLEEDING

CLASSIFICATION • Upper GI Bleeding- proximal to ligament of Treitz • Lower GI Bleeding – distal to ligament of Treitz

Presentations of Upper GI bleeding • Hematemesis is passage of vomited material that is black (“coffee grounds”) or contains frank fresh blood • Melena is the passage of black, tarry, sticky offensive loose stools (due to effect of intestinal bacteria on blood leading to oxidising hemoglobin to hematin ( To form black, tarry stools (melena), there must be 150 -200 cc of blood and the blood must be in the gastrointestinal tract for 8 hours to turn black )

Presentations of Lower GI bleeding • Hematochezia is passage of bright or dark red blood per rectum; indicates colonic source or massive upper GI bleeding. • May be mixed with stool or seen on toilet paper • • In general, the redder the blood, the more distal the site of bleeding

• Obscure GI Bleed- overt g. I bleed where bidirectional endoscopy could not reveal etiology of bleeding • Occult GI Bleed-an invisible bleeding that can be detected by a specific test on the stool. (UGI OR LGI bleeding) • Both UGI and LGI bleeds can be painless/associated with abdominal pain

Spurious Haematemesis • Red: beets, laxatives, phenytoin, rifampin� • Black: bismuth, activated charcoal, iron, spinach, blueberry. • Bleeding from gums tonsils tongue

ETIOLOGY UPPER GI BLEED • Swallowed maternal blood • Gastritis • Vitamin K Deficiency • Malformation IN NEONATES LOWER GI BLEED • Swallowed maternal blood • NEC • Vitamin k deficiency • Malformation (volovulus)

ETIOLOGY IN CHILDREN UPPER GI BLEED • • Gastritis Esophagitis Stress Ulcer Peptic Ulcer Mallory Weiss Tear AV Malformation Esophageal Varices LOWER GI BLEED • • • Allergic enteropathy Intussusception Infective colitis Meckels diverticulum Malformation Anal fissure Juvenile Polyps NSAIDS IBD

APPROACH • Hemodynamic stability • Decide whether it is UGI/LGI bleeding • Manage the bleeding lesion

• • CBC Coagulation profile LFT Stool examination Plain xray USG Abdomen Angiography ENDOSCOPY Colonoscopy Enteroscopy Wireless capsule endoscopy Bleeding Scan(Tagged RBC Scintigraphy)

MANAGEMENT OF ACTIVE BLEEDING • ABC • Packed RBC in case of acute drop in hemoglobin • NPO • Nasogastric tube with gastric lavage • Acid suppression by PPI • FFP/Vitamin K/Platelet transfusion • Treatment according to cause

Variceal Bleeding 1. Pharmacotherapyq Octreotide q. Somatostatin q. Vasopressin q. Terlipressin
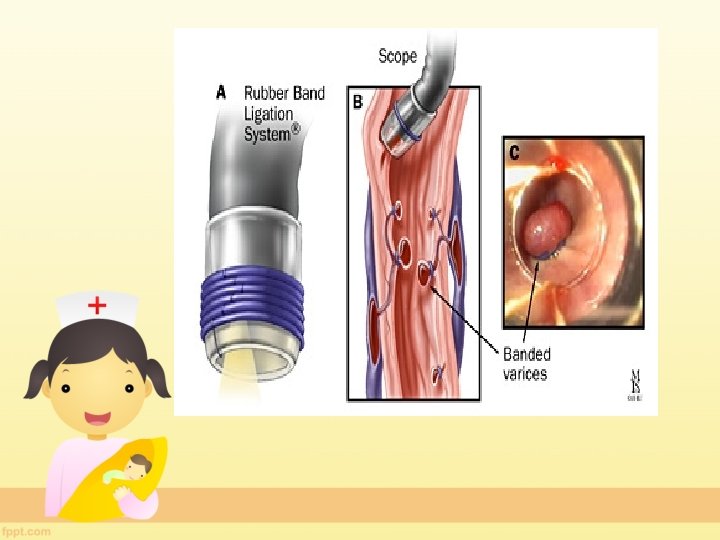
 – ENDOSCOPIC VARICEAL LIGATION(EVL)")
Variceal bleeding • 2. ENDOSCOPY – ENDOSCOPIC SCLEROTHERAPY(EST) – ENDOSCOPIC VARICEAL LIGATION(EVL)


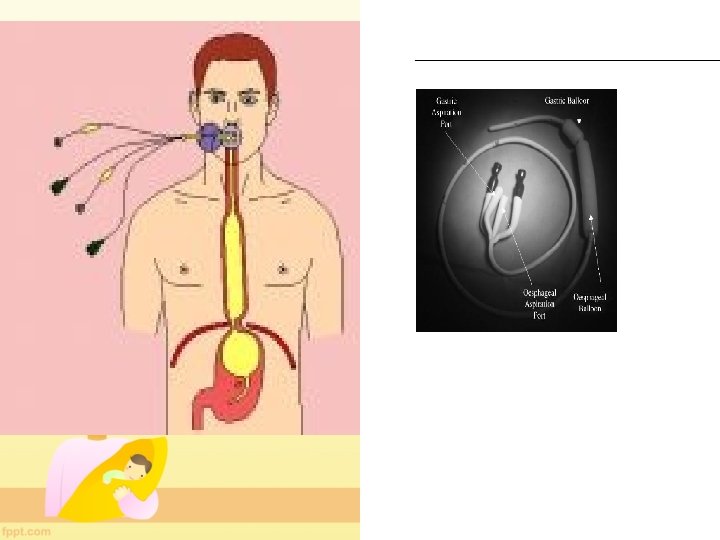
• 3. TAMPONADE OF VARICES – SENGSTAKEN BLACKMORE TUBE • 4. TIPS-Transjugular Intrahepatic Portosystemic Shunt • 5. Surgery is rarely necessary now (if patient continues to bleed despite EST. )

PHARMACOLOGICAL PROPHYLAXIS: Non-selective beta-blockers M. O. A. they reduce the cardiac output and thereby lower portal pressure PROPANOL.

PORTAL HYPERTENSION

PORTAL HYPERTENSION is the commonest cause of gastrointestinal bleeding in India. Mortality after index hematemesis in variceal bleeding is 30% and after recurrent variceal bleeding is as high as 70%. Indian studies revealed that extrahepatic portal vein obstruction is the predominant cause of portal hypertension in india. In developed countries cirrhosis account for 55 -60% of all portal hypertension in children.

Definition Elevation of portal pressure above 1012 mm Hg It occurs because of increased portal resistance or portal blood flow

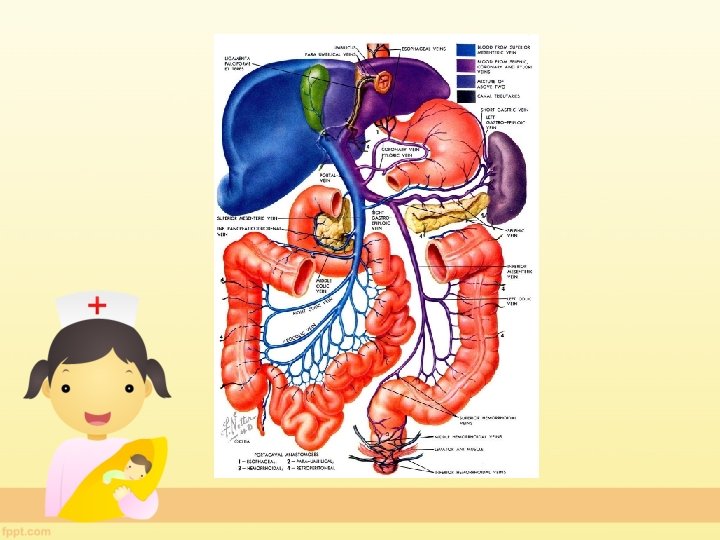
Anatomy The portal system includes all veins, which carry blood from the digestive tract (expect lower part of rectum and anal canal), spleen, pancreas and gall bladder to the liver, via the portal vein.
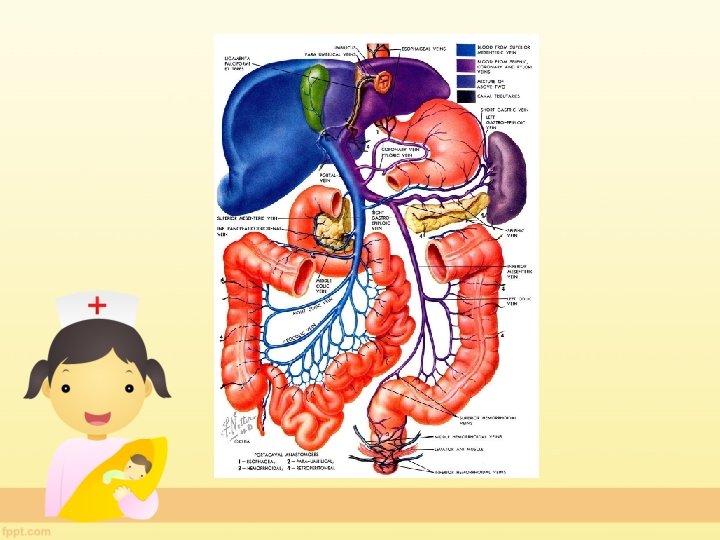

Portocaval anastamosis

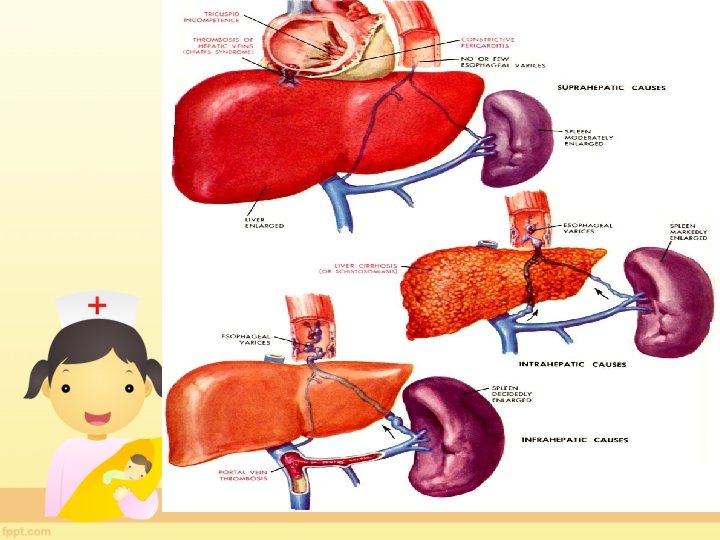
Causes of Portal Hypertension 1. EXTRAHEPATIC PORTAL HYPERTENSION 2. INTRAHEPATIC PORTAL HYPERTENSION 3. POST SINUSOIDAL OBSTRUCTION

EXTRAHEPATIC PORTAL HYPERTENSIOIN • Portal vein thrombosis • Splenic vein thrombosis • Arteriovenous fistula • -increased portal flow

Precipitating Factors Of Vein THROMBOSIS: • umblical catheterization in neonates • Umblical infection • Intraabdominal infection • Biliary tract infection • Hypercoagulable states like Dehydration Polycythemia • Trauma to portal vein.

INTRAHEPATIC PORTAL HYPERTENSION • Cirrhosis • Infection –liver/biliary tract • Metabolic • Autoimmune hepatitis • Drugs • Schistosomiasis –ova causes reaction in minute portal venous radicles

Post sinusoidal POST SINUSOIDAL A. BUDD-CHIARI SYNDROMEOccurs because of obstruction to hepatic veins anywhere between efferent hepatic veins and entry of inferior vene cava in right atrium B. CONSTRICTIVE PERICARDITIS

CLINICAL FEATURES Upper Gastrointestinal Bleeding *Bleeding from esophageal varices is the most common presentation especially in EHPHT. *Usual manifestations are haematemesis or malaena

Bleeding can be precipitated by minor illnesses. NSAIDS use is one of its contributing factors. coughing during respiratory illness may increse intracaval pressure and lead to bleeding. Colour of the vomited blood is usually fresh red Volume is usually Large. Bleed is usually PAINLESS
")
Gastrointesinal hemorrhage can also originate from gastric , duodonal or rectal varices (hematochezia)

SPLEENOMEGALY Second most common manifestation after bleeding. Spleen is usually moderately enlarged, massive splenomegaly is rare. However size of spleen DOES NOT correlate well with portal pressure. Spleen is firm or hard depending on duration of of PHT

May be discovered first on routine physical examination. IF SPLEEN CANNOT BE FELT OR IS NOT ENLARGED ON IMAGING, DIAGNOSIS OF PVT IS QUESTIONABLE. However, sometimes spleen becomes impalpable following massive bleed causing diagnostic confusion.

COMBINATION OF GASTROINTESTINAL BLEEDING + SPLENOMEGALY IS PATHOGNOMIC OF PHT UNLESS PROVED OTHERWISE.

HEPATOMEGALY In case of cirrhosis, liver is enlarged in initial cases and firm. Later liver shrinks and span decreases. Hepatomegaly is rare in EHPHT, as liver is not directly affected. Post hepatic PHT usually present with tender hepatomegaly

ASCITES DIAGNOSIS OF PORTAL HYPERTENSION SHOULD ALWAYS BE KEPT IN MIND IN CASES OF ASCITES + SPLENOMEGALY

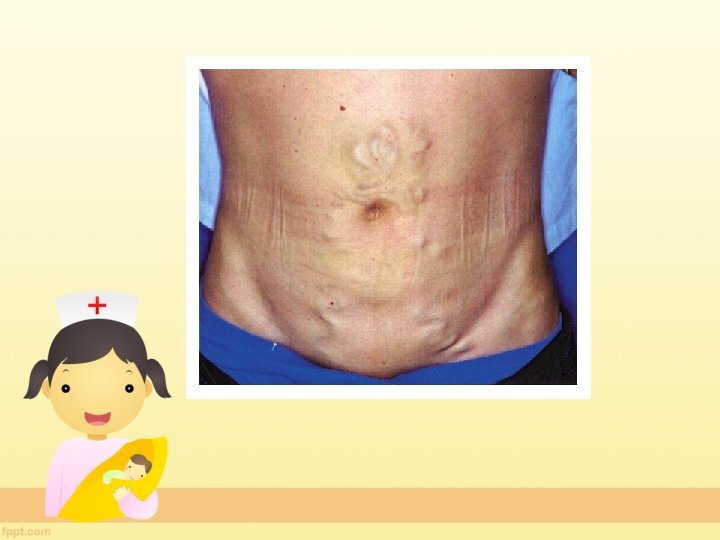
CAPUT MEDUSA-Indicates prominent collateral vessels in peri umblical region in sinusoidal PHT. Dilated veins in anterior abdominal wall

Investigatory Approach to Portal HT This is directed towards : - 1. Assessment of current hematological status of the child 2. Concomitant information on the liver function and etiology of the liver disease. 3. Demonstration of site of bleeding collaterals

HISTORY AND PHYSICAL EXAMINATION History of symptoms History directing to underlying cause of Portal Hypertension. Physical examination: Stunted growth Pallor Splenomegaly , hepatomegaly Jaundice Ascites Tender hepatomegaly, tender abdomen Anterior abd. wall dilated veins, caput medusa Hemorrhoids Stigmata of chronic liver disease Signs of hepatic encephalopathy

LAB STUDIES : Complete hemogram Peripheral smear LFT, RFT PT/APTT Investigations relating to specific diagnosis: Hepatitis A, B, C Alpha antitrypsin deficiency Anti nuclear antibodies, anti LKM, etc Ceruloplasmin, 24 hour urine copper Liver biopsy

*ULTRASONOGRAPHY It is the easiest non invasive diagnostic means.

ENDOSCOPY Demonstration of esophageal varices. Congestive gastropathy and gastric varices may be demonstrated.

MANAGEMENT RESUSCITATION ENDOSCOPY + PHARMACOTREHAPEUTICS DEFINITIVE MANAGEMENT

TREATMENT OF VARICEAL BLEEDING INITIAL RESUSCITATION TR CRYSTALLOID INFUSION REPLACEMENT OF RED BLOOD CELLS VITAMIN K PLATELET/FFP/BOTH H-2 BLOCKERS MONITORING OF ONGOING BLEEDING IN EHPHT where liver functions are not much compromised , bleeding may stop spontaneously

PROGNOSIS: 1. Portal hypertension secondary to intrahepatic disease has a poorer prognosis Usually progressive and associated with deteriorating liver funtion and ultimately require liver transplantation. Liver transplantation is the only effective therapy for hepatopulmonary syndrome and patients secondary to hepatic vein obstruction

TAKE HOME MESSAGE: • Portal hypertension is a CLINICAL DIAGNOSIS. • Always try to find underlying cause of portal hypertension. • NO PATIENT SHOULD DIE OF VARICEAL BLEEDING.

THANK YOU

IDIOPATHIC PORTAL HYPERTENSION An idiopathic form of portal hypertension characterised by splenomegaly , hypersplenism , and portal hypertension without occlusion of portal or splenic veins and with no obvious disease in the liver has been described.

ETIOLOGY in Older Children UPPER GI BLEED • • Gasrtitis Esophagitis Stress Ulcer Peptic Ulcer Mallory Weiss Tear Av Malformation Swallowed Blood From Nasopharynx LOWER GI BLEED • • Anal fissure Infective colitis Meckels diverticulum Malformation
- Slides: 53