Gastrointestinal Assessment NURS 101 Anatomy and Physiology Review




")




, rectum, anus �Most important function:")





 �Food intolerance or gall bladder dz may increase gas")












- Slides: 37
Gastrointestinal Assessment NURS 101
Anatomy and Physiology Review
GI Tract �Extends from mouth to anus �Function is to supply nutrients to body cells �Ingestion-digestion-absorption �Elimination excretes waste productions of digestion
GI organs �Mouth �Esophagus �Stomach �Small intestine �Large intestine �Rectum �Anus �Liver �Pancreas �gallbladder
GI Tract �Receives approx. 25 -30% of cardiac output �Enteric nervous system (gut brain) coordinates motor and secretory activities
Factors that affect function �Stress, anxiety �Dietary intake �Alcohol or caffeine, cigarettes �Poor sleep, fatigue �Medications �Disease
Digestion/Absorption �Begins in mouth: chemical and mechanical �Stomach holds food and empties into small intestine at rate at which digestion can occur. �Low p. H (acidic) gastric fluids aids in protection against ingested organisms �Most absorption occurs in small intestine (transfer of end products of digestion across intestinal wall to circulation)
Small Intestine �Functional unit is villi, microvilli �Digestive enzymes break down nutrients to be absorbed.
Digestive Secretions �Salivary glands: amylase �Stomach: Pepsinogen, HCl acid, Lipase, Intrinsic factor �Small Intestine: Enterokinase, Amylase, Peptidases, Aminopeptidase, Maltase, Sucrase, Lactase, Lipase �Pancreas: Trypsinogen, Chymotrypsin, Amylase, Lipase �Liver and Gall Bladder: Bile
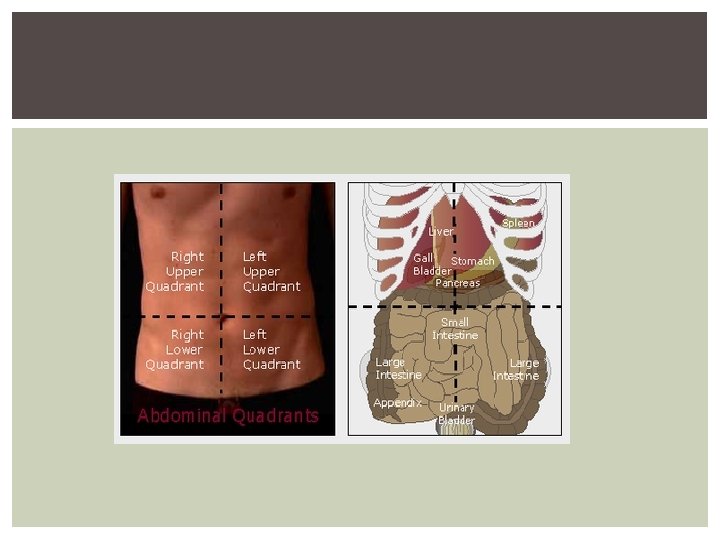
Elimination �Large intestine: Cecum/appendix, colon (ascending, transverse, descending, sigmoid), rectum, anus �Most important function: absorption of water and electrolytes �Feces is 75% water, bacteria, unabsorbed minerals, undigested food, bile pigments, shedded eptithelial cells.
Large Intestine
defecation �Feces stimulates sensory nerves �Nerve fibers produce contraction of rectum and relaxation of sphincter �Controlled voluntarily by relaxing the internal and external sphnicter �“acceptable environment” is necessary �Facilitated by Valsalva maneuver
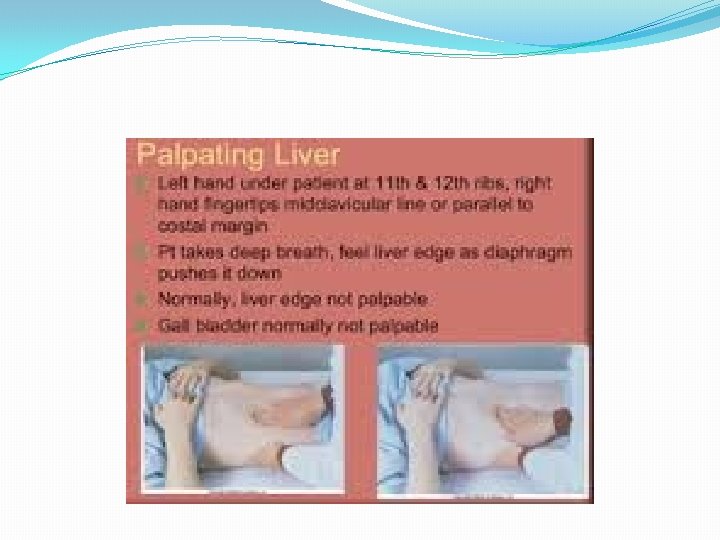
Liver �Carbohydrate metabolism �Protein metabolism �Fat metabolism �Steroid metabolism �Detoxification �Bile synthesis �Storage �Breakdown old blood cells
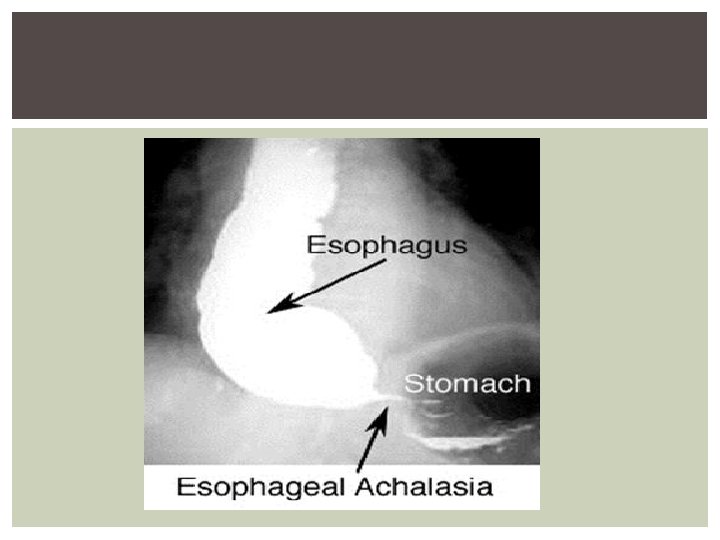
Age Related Changes to GI �Tooth/gum breakdown and disease �Salivary secretions diminish �Delayed esophogeal clearance �Increased GERD �Delayed motility �Increase incidence of gallstones �Decreased sphincter tone �Increased incidence of constipation
Assessment �Health History �Abdominal pain �Dyspepsia �Gas �Diarrhea or constipation �Fecal incontinence �Jaundice �Previous GI disease
“gas” �Belching or flatulence (“flatus”) �Food intolerance or gall bladder dz may increase gas �Excess gas may lead to bloating and discomfort
history �Personal and social history �Oral care �Medications �Nutrition and eating habits �Family history �CA
Physical Assessment
OBJECTIVE DATA Inspect Auscultate Percuss Palpate
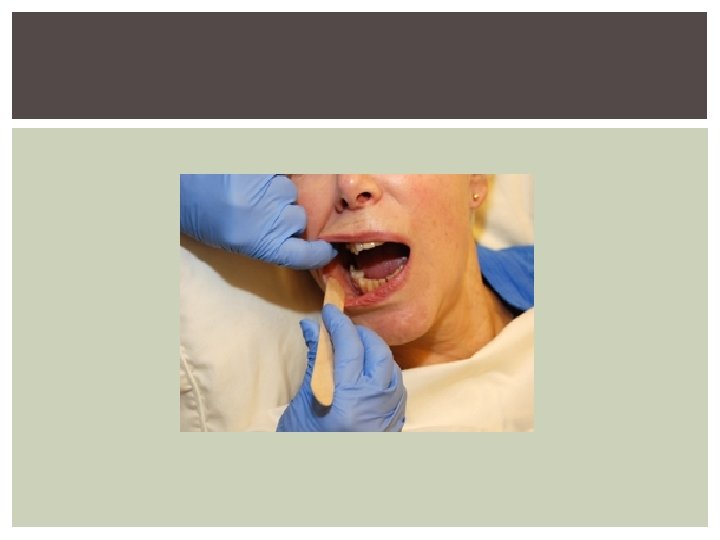
MOUTH Symmetry, color, size Pallor, cyanosis, cracking, ulcers, fissures, lesions Loose teeth, swollen gums, note breath Palpate any suspicious areas. Note presence of dentures and ask pt to remove for thorough exam. Use a tongue blade.
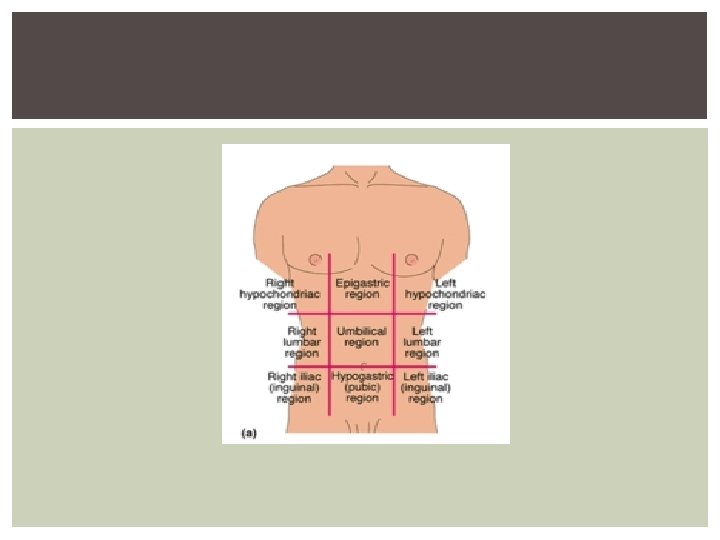
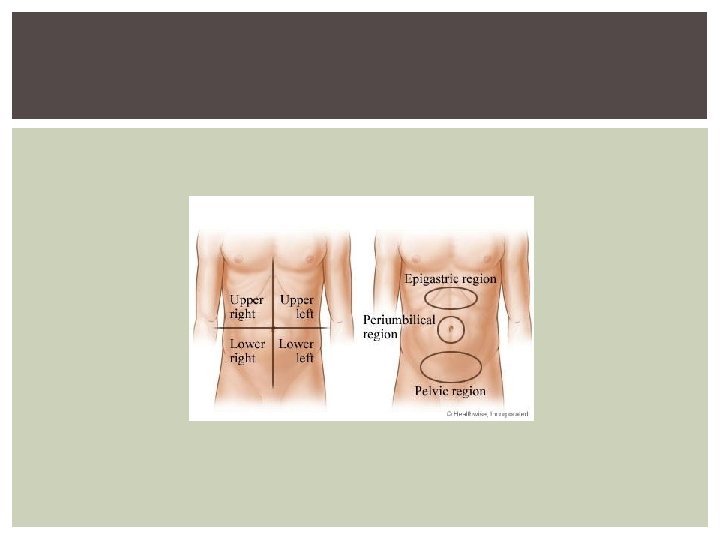
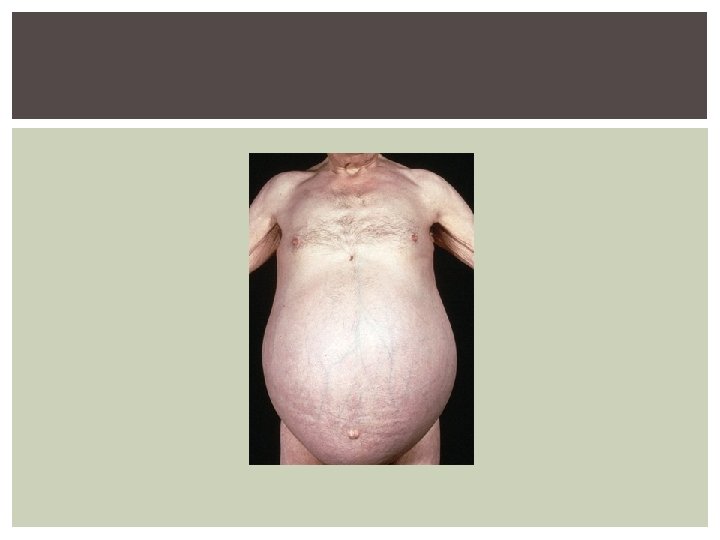
abdomen �Inspect for skin changes, dilated veins, contour, symmetry �Contour: flat, round, concave, distended �Movement: pulses or peristalsis �Auscultate next!!! Why? ? ? �Use diaphragm of stethoscope for high pitched bowel tones; should hear clicks or gurgles �Starting in lower right quadrant (why? ) listen in all 4 quadrants �Percuss to determine presence of fluid, distention, masses. Tympany is predominant sound. �Palpate to detect tenderness, masses, muscular resistance.
RECTUM AND ANUS Inspect perianal and anal areas for color, texture, lumps, scars, hemorrhoids, discharge, prolapse. Gloved finger to palpate inside rectum (point toward umbilicus) and to obtain fecal occult blood specimen.
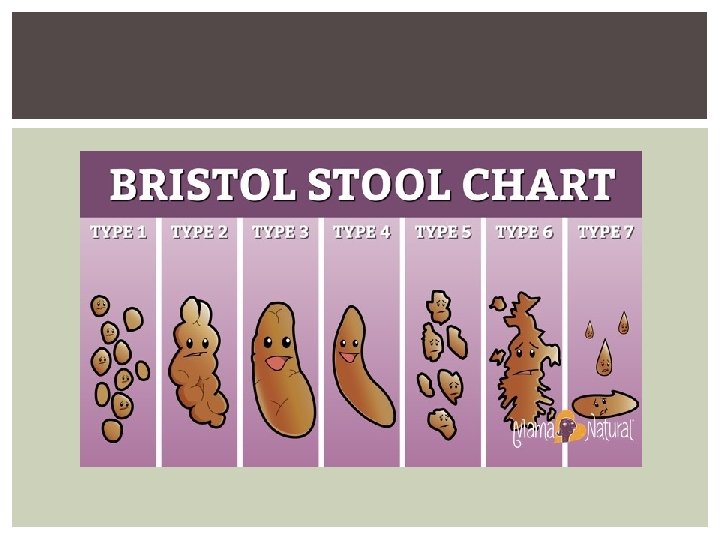
STOOL APPEARANCE
LABS ASSOCIATED WITH GI ASSESSMENT LFT’S AMYLASE LIPASE
FECAL OCCULT BLOOD TEST Detects “hidden blood” Small smear of feces on testing card, apply reagent Positive test is _______ Single test has limited value in detecting colorectal CA Sometimes called “Guaiac” Certain foods may cause false-positive reading. § § ______________ Vit C may cause false neg
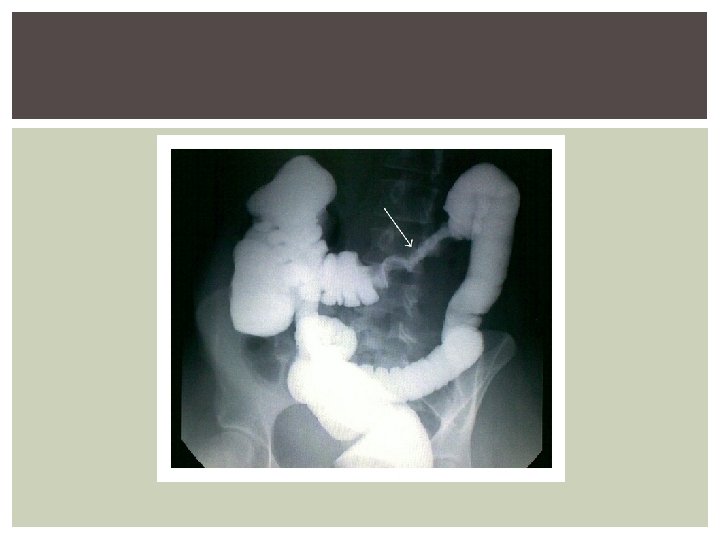
UPPER GI SERIES AKA ___________ Diagnoses structural abnormalities of esophagus, stomach, and duodenum Nurses explain procedure to pt, position during fluoroscopy NPO for 8 -12 hours, including smoking Oral contrast Fluids, laxatives to prevent post study impaction. Expect white stool
LOWER GI SERIES Aka barium enema Nurses: administer laxatives and enemas until colon is clear before study. NPO 8 hours prior. Explain procedure and position patient. Explain that urge to defecate may occur during procedure. After procedure, give laxatives and enemas to help expel contrast
ABDOMINAL ULTRASOUND Used to show size and configuration of organs. Non invasive. Conductive gel is applied to skin and transducer is placed on area. NPO ____ hours before. For gall bladder studies, ______meal the night before. Air, gas, or presence of food in GI tract can result in reduced quality of images