GASTROINTESTINAL ANOMALY IN PAEDIATRIC presented by Dr ALIYA

GASTROINTESTINAL ANOMALY IN PAEDIATRIC presented by: Dr. ALIYA SHEMISA

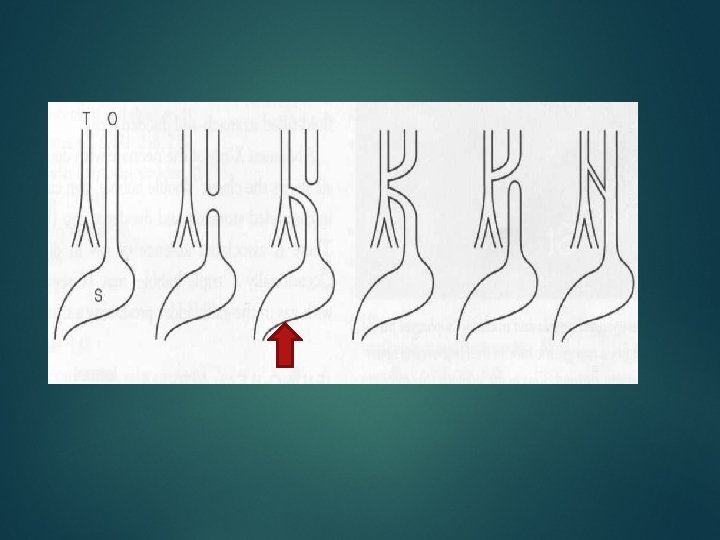
Esophageal atresia &tracheoesophageal fistua TEF Esophageal atresia : to be considered in newborn with feeding problems & recurrent aspiration. - most common congenital anomaly of the esophagus. - is an absence in contiguity of the esophagus due to an inappropriate division of the primitive foregut into the trachea teriorly & esophagus posteriorly at 4 th week of gestation. . General pathogenesis includes teratogenic effect caused by early pregnancy use of Anti-thyroid drug. Ante-natal USS. finding include polyhydramnios, Or in N. N failure to successfully pass NGT.

The most frequent is the proximal esophageal atresia “blind sac like” with distal TEF (85%). Associated anomalies in 50 -70% of the cases include : Other GIT atresia: D. A, Jej-Ileal atresia, anal atresia & pyloric stenosis. VACTERL association : (Vertebra: heimivertebri, spina bifida, caudal cord regression), ( Anal atresia) , ( Cardiac anomalies: VSD, ASD, & PDA), (Treacheo-Esophageal fistula & atresia), (Renal anomalies: ( MCDK & renal agenesis), (Limb anomalies : Radial dysplasia, radial club hand & polydactly or oligodactyly) Right sided aortic arch in 5%

: Air in the blind-ending upper esophageal pouch posterior to - NGT looping & turning back at the upper thoracic part. . - Gasless abdomen unless there is distal TEF. - Sign of aspiration pneumonia may be seen. - Contrast swallow/fluoroscopy : is modality of choice for the diagnosis ,

ESOPHAGEAL ATRESIA -Treatment & prognosis : surgical intervention with re- anastomosis. Prognosis is variable depends on other associated anomalies

ESOPHAGEAL ATRESIA
 GUT OBSTRUCTION HYPERTROPHIC PYLORIC STENOSIS (HPS) - HPS is idiopathickening of gastric pyloric")
1) GUT OBSTRUCTION HYPERTROPHIC PYLORIC STENOSIS (HPS) - HPS is idiopathickening of gastric pyloric musculature which then result in progressive gastric outlet obstruction. - Occurs typically between 1 st week -3 months of age - Symptom : non-bilious projectile vomiting , -Hyperatrophid Pyloric Muscle can be palpated as an olive size mass in Rt. Upper quadrant

Radiological features : USS abdomen is the modality of choice it directly visualizes the pyloric muscle without radiation exposure. Gastric distension & mottled retained gastric content. * ( > 3 mm thickness & >15 mm length is diagnostic for HPS) Sonographic signs cervix sign Target sign
 Fluoroscopy Barium")
Plain film : non-significant , distended stomach. (large single gastric air bubble) Fluoroscopy Barium meal : barium given orally by bottle , shows delayed gastric emptying with elongated narrow lumen Barium sign: Shoulder sign String sign Mushroom sign Treatment & prognosis: Rehydration & electrolyte correction prior to surgical Pyloromyotomy
 SINGLE AIR shouldering Mushroom sign")
Barium meal study x-ray plain abdomen ( string signs) SINGLE AIR shouldering Mushroom sign BUBBLE

USS signs of HPS Target sign Cervix sign

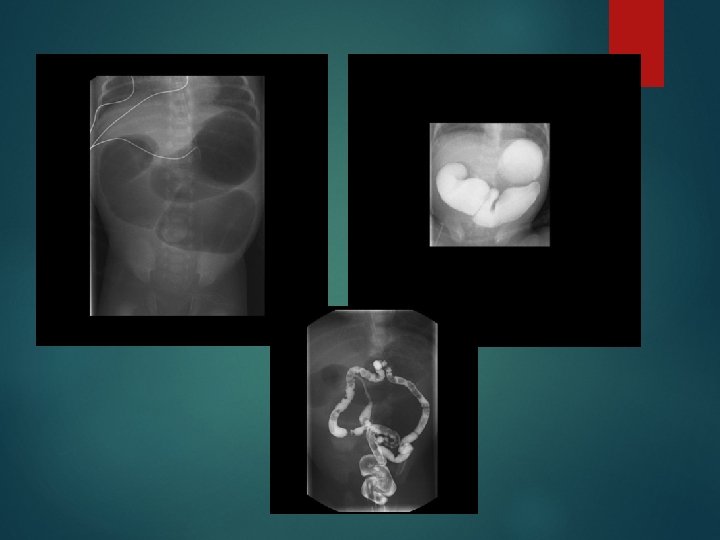
DUODENAL OBSTRUCTION Duodenal atresia is the most common intrinsic cause. other causes are extrinsic : annular pancreas, peritoneal Ladd’s band. - D. atresia is congenital malformation of duodenum as failure of recanalisation of the bowl lumen. -20 - 30% of the cases are Down syndrome. -Associated anomalies VACTERL, Annular pancreas. - Baby presented with abd. Distention & bile-stained vomiting. -Plain abdomen X-ray: - Gas filled stomach & duodenum (double bubble sign) - Absence of distal bowl gasses. Some distal gas bubbles indicate partial obstruction. - Small amount of Upper GIT contrast study helpful to confirm the diagnosis

DUODENAL ATRESIA DOUBLE BUBBLE SING n

JEJUNAL ATRESIA -The site of the atresia can be anywhere from the ligament of Treitz to the jejunoileal junction. There can be more than one atretic segment. most commonly occurs in the proximal jejunum with triple bubble appearance in Abdomen X-ray Ba. Enema : unused microcolon NN abdominal distension with bilious vomiting at D 1 of life.

Anorectal Atresia -membranous separation or complete absence of an anus “ No anal opening”. - Anorectal atresia is classified as either a low or high anomaly. - with a high anomaly the bowel ends above the levator sling, and is usually associated with a fistula into the vagina or posterior urethra.

-A lateral rectal radiograph is performed - Gas in the bladder or vagina indicates the presence of fistula. - associated sacral anomalies may also be seen as sacral agenesis.

Malrotation & mid gut Volvulus - All of the small bowel from the second part of duodenum plus the proximal large bowel to the distal transverse colon is formed from the embryological midgut in several stages. - Up to the week 6 of gestation the midgut lies within the abdominal cavity. - From the weeks 6 to 10 of gestation the midgut develops outside the abdominal cavity (physiological herniation). - By week 10 the midgut returns to the abdominal cavity. During these various stages of embryological development the midgut rotates through 270 degrees

Malrotation

Barium meal follow through Malrotation Normal

- These anatomical variants may produce clinically significant complications, including duodenum obstruction by Ladd’s bands , volvulus of the small bowel, intestinal ischemia & necrosis in the distribution of the SMA. -These complications lead to two common types of clinical presentation: 1. Severe bile-stained vomiting in neonates. 2. Intermittent symptoms in older children: vomiting, nausea, and abdominal pain. Barium meal – follow through is modality of choice for diagnosis. - -

-The Abdomen X-R may show non-specific signs - The upper GIT contrast study is usually definitive in the diagnose or exclude malrotation. - The anatomical key finding is malposition of the duodeno-jejunal Junction, this junction should lie to the left of midline at level of L 1 - Positioning of the duodeno-jejunal junction to the right or in the midline indicates malrotation. Other signs of malrotation that may be seen on the contrast study include: • Proximal jejunum lying in the right abdomen. • 'Corkscrew' appearance of small bowel loops. • Abnormally high location caecum on follow-through films.

Ba. Meal – follow through shows Malrotation deudeno-jeujenal junction at Rt. side

Corkscrew appearance

MECONIUM ILEUS New born bowel obstruction of the distal ileum due to bnormally thick impacted meconium Plain radiographic abdominal X-ray : Small bowel obstruction, dilated bowel loops proximal to impaction (bubbly pattern) with absence of Air-fluid level.
. -")
- Fluoroscopy/ contrast enema : Microcolon of entire large colon. (unused colon). - Fluoroscopy/ meal / follow through : Small amount of Oral water soluble contrast by NGT just to opacified small loops & visualize the meconium as filling defect. Complication: ileal atresia / stenosis or ileal perforation leading to meconium peritonitis. Treatment & prognosis: evacuated within 6 hrs of birth or earlier by contrast enema, if failed or perforation suspected ; surgical intervention.

Meconium ileus Soap bubbles sign in muconium ileus.

Ba. Enema: microcolon in meconium ilus

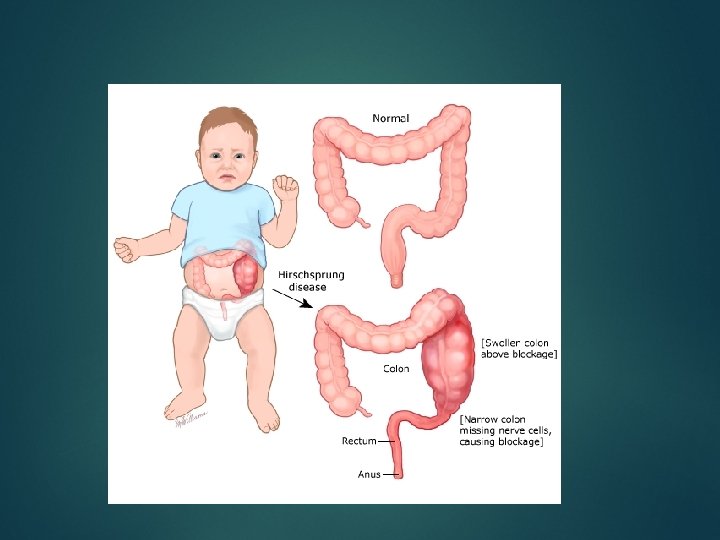
Hirschsprung’s disease - Hirschsprung disease involves an aganglionic segment of distal large bowel. (missing nerve cells in the colonic muscle) - A distal short aganglionic segment is the most common form, this causes distal obstruction with dilatation of normally innervated bowel proximal to the aganglionic segment

- Hirschsprung disease usually presents in neonates with abdominal distension and constipation with delayed passing muconium with in 1 st day of age. Contrast enema & rectal biopsy is modality of choice for diagnosis , it shows a transition zone from the aganglionic segment to dilated normally innervated bowel.

Hirschsprung disease Ba. Enema AP view

Hirschsprung disease Barium enema lateral view No preparation is needed before the enema to avoid water intoxication The barium limited to amount required to show the zone of transition from the agangolionic to dilated bowels.

Intussusception refers to prolapsed or telescoping of a segment of bowel (referred to as the intussusceptum) into the lumen of more distal bowel (the intussuscepi-ens). The most common form is ileo-colic (i. e. prolapse of distal small bowel into the colon).

- usually from 6 months to 2 years of age , common cause of intestinal obstruction. - Clinical presentation: excessive crying, abdominal pain, palpable upper Rt. Quadrant abdominal mass & red-currant jelly stained stool.

Ultrasound: -is the first choice modality for diagnosis. - appears as heterogeneous soft tissue mass seen closed to the area of RHC. - Characteristic appearance is(target or doughnut) sign, (pseudo-kidney) sign in longitudinal section. - Doppler USS is important.

Pseudokidney sign. Target or doughnut sign. Doppler uss

Plain abdomen X-ray : Mass in the Rt. Upper quadrant. Ba. Enema , water soluble contrast or gas enema show : filling defect at transverse colon at hepatic flexure. (contra-indicated if perforation is suspected).

Ba. Enema shows filling defect intussusception Plain abdomen x-ray

Treatment : -It is a surgical emergency & it is fatal condition if not treated. - needs surgical & radiological team involvement. - Reduction - Absolute contraindication for reduction: shock not corrected with IV fluids, perforation with clinical signs of peritonitis. Complication : bowel ischemia and perforation

- Slides: 43