Gastroesophageal Reflux Disease GERD Questions Answers Iranian College

 Questions & Answers Iranian College of Internal Medicine Hamid Kalantari")






 • The majority of patients with typical symptoms of")






 • Do you experience GERD or heartburn")
 • Have these symptoms been ongoing for")
 • Do you have pain after you")











 Reduce lower esophageal sphincter pressure: • Fatty foods")



 Medication (generic) Medication (trade) Uses Amitriptyline Elavil")
 Medication (generic) Medication (trade) Uses Labetalol n/a")
 Medication (generic) Medication")
 Medication (generic) Medication")








. •")
 • Ranitidine (Zantac) • Famotidine")


 l PPI inhibit H+/K+-ATPase in the")

 oral Omeprazole 20 mg/ day; maintenance dose, 20")











 • Achalasia • Esophageal cancer •")



 • Corpus predominant")




 therapy with an H 2 receptor antagonist or proton")



 • In patients with persistent heartburn despite PPI")
 • We usually begin by giving 10 mg")












- Slides: 95
Gastroesophageal Reflux Disease (GERD) Questions & Answers Iranian College of Internal Medicine Hamid Kalantari MD Professor of Gastroenterology Isfahan University of Medical Sciences
Gastroesophageal reflux goes by several names: • GERD • Reflux • Heart burn • Indigestion
Definition of GERD • When the reflux of gastric content causes troublesome symptoms or complications.
Diagnosis • GERD presents with typical signs and symptoms, such as heartburn or acid regurgitation, that are responsive to antisecretory therapy.
Montreal classification of GERD
Who should have endoscopy? • Individuals who: § Fail to respond to therapy. § Have alarm symptoms or signs such as: dysphagia, weight loss, anemia, gastrointestinal bleeding, persistent heartburn. § Require continuous maintenance medical therapy to rule out Barrett's esophagus.
What are the goals of endoscopy? • Detection of erosive esophagitis. • Complications such as: § Peptic stricture § Barrett's esophagus and cancer of esophagus. • Excludes conditions that can mimic GERD, such as eosinophilic esophagitis.
Nonerosive gastroesophageal reflux disease (NERD) • The majority of patients with typical symptoms of GERD do not have esophagitis.
NERD A. Normal levels of esophageal acid: Esophageal hypersensitivity – Assessed by a 24 hour p. H monitoring study. B. Abnormal levels of esophageal acid. C. heartburn not attributable to acid reflux: “Functional heartburn" – Groups (A, B), but not the Group C may respond to antisecretory therapy. – Proton pump inhibitors were associated with more effective symptom relief than placebo or H 2 receptor antagonists in such patients
Treatment of esophageal hypersensitivity • Pain modulators such as: § Tricyclic antidepressants § Trazodone § Selective serotonin reuptake inhibitors (Improve esophageal pain in patients with noncardiac chest pain (by acting at the central nervous system and/or sensory afferents level)
Can I have GERD without any symptoms? Yes, GERD can occur with "silent" symptoms.
Silent GERD" is one of the most difficult conditions to diagnose • Sleep disruption (A diagnosis of GERD with complaints of difficulty sleeping) • Persistent cough • Asthma attacks • Hoarseness • Dental erosions (may be the first symptom) • Bad breath • Water brash
Is there a difference between day time and night time GERD? • The major difference between day and night GERD management is in your body position.
Can GERD cause changes in my voice? • Repeated acid damage of the voice box can cause growths (polyps) to develop and can increase your risk of cancer.
What are alarm signs of GERD? (1) • Do you experience GERD or heartburn 3 or more times per week? • Is the pain in your chest from heartburn or reflux debilitating? • Does the pain radiate to your arm or cause you to become short of breath? • Does the pain wake you from sleep or prevent you from getting a full night's rest?
What are alarm signs of GERD? (2) • Have these symptoms been ongoing for more than 6 months? • Do you have a persistent and unexplained cough? • Is your asthma difficult to control with conventional medications? • Has the reflux caused you to lose weight over the past few months?
What are alarm signs of GERD? (3) • Do you have pain after you eat? • Do you have any difficulty swallowing? • Do you wake up from sleep coughing, choking, or short of breath? • Do you have unexplained repeated episodes of bronchitis or pneumonia?
Pregnancy & GERD • Lifestyle modifications or antacids should be first line therapy. • H 2 receptor antagonists ranitidine and cimetidine, which appear to be safe during pregnancy. • Proton pump inhibitors. (Less experience) No significant difference in the risk for major congenital birth defects, spontaneous abortions, or preterm delivery.
Do children get GERD? Infants may exhibit symptoms different from adults • Irritable after eating • Repeatedly belch or vomit • Persistent coughing ü Poor feeding ü Impaired weight gain or colic or
Does GERD affect one gender more than the other? Females are slightly more affected by GERD
Can GERD happened out of patient’s control? • Factors out of a patient's control include: – Genetics – Personal background
How can I improve my symptoms of GERD?
How can I improve my symptoms of GERD? • Mild symptoms: lifestyle and dietary modifications along with antacids and histamine 2 (H 2) receptor antagonists. • Debilitating symptoms: acid suppressive therapy. • Between these extremes: “Step up" approach. “Step down" approach.
Lifestyle modifications
Aims of Lifestyle modifications • Enhancing esophageal acid clearance. • Minimizing the incidence of reflux.
Does my bed make a difference in nighttime symptoms? Head of bed elevation: • 6 to 8 inch (it is important for individuals with nocturnal or laryngeal symptoms). Night symptoms: • Heartburn • Regurgitation with coughing, aspiration and pneumonia • Choking • Gasping for air • Bitter taste in your mouth or excessive drooling
What kind of foods can make GERD worse? • High fat foods • Alcohol • Spicy foods • Colas • Carbonated beverages • Red wine • Chocolate • Orange juice • Mint
What kind of foods should I eat if I Have GERD? • Smaller and lighter meals • Most food and vegetables • High protein diet • Low fat diet
Foods can make GERD worse (Mechanism) Reduce lower esophageal sphincter pressure: • Fatty foods • Chocolate • Peppermint • Excessive alcohol Acidic p. H can exacerbate symptoms: A number of beverages include: • Colas • Red wine • Orange juice (p. H 2. 5 to 3. 9).
Can smoking cause GERD? Smoking does not directly cause GERD, it can exacerbate GERD symptoms. Smoking is deleterious in part because it diminishes salivation. Promotion of salivation by either chewing gum or use of oral lozenges.
Can stress increase GERD symptoms? • Some people do experience heartburn in times of stress. • Stress hormones cause stomach relaxation • Stress hormones may increase stomach acid production.
Can medicines exacerbate GERD? • Relaxes the LES of the esophagus. • Irritates and directly damages the lining of the esophagus. • Can cause the body's digestive system to slow down, which leads to food lingering in and more acid production in the stomach.
Medications that May Cause Reflux or Heartburn(1) Medication (generic) Medication (trade) Uses Amitriptyline Elavil Antidepressant medication Diazepam Valium Antianxiety Diltiazem Cardizem, Cartia, Tiazac Calcium channel blocker High blood pressure Doxepin Sinequan Antidepressant medication Felodipine Plendil Calcium channel blocker High blood pressure Imipramine Tofranil Antidepressant medication Isosorbide nitrate Imdur, Nitrodur Nitrates High blood pressure or angina
Medications that May Cause Reflux or Heartburn(2) Medication (generic) Medication (trade) Uses Labetalol n/a Beta Blocker High blood pressure Levodopa Sinemet Anti Parkinsons Nifedipine Adalat, Procardia Calcium channel blocker High blood pressure Nortriptyline Aventyl, Pamelor Antidepressant medication Progestin n/a Birth control or abnormal menstmal bleeding Theophylline Theolair, Uniphyl Anti. Asthma Mctoprolol Toprol Beta blocker High blood pressure
Medications that can Cause Direct Damage to the Esophagus Medication (1) Medication (generic) Medication (trade) Uses Alendronate Fosomax Osteoporosis Medication Aspirin Anti inflammatory Azithromycin Zithromax Antibiotic Clarithromycin Biaxin Antibiotic Erythromycin E mycin Antibiotic Ibuprofen Advil, Motrin Anti inflammatory
Medications that can Cause Direct Damage to the Esophagus Medication (2) Medication (generic) Medication (trade) Iron Uses Mineral supplementation Naproxen Aleve, Naprosyn Anti inflammatory Potassium K Dur Mineral supplementation Quinidine Duraquin Heart rate medication Risedronate Actonel Osteoporosis medication Tertracycline Sumycin Antibiotic Vitamin C Vitamins
How can I avoid GERD problems if I have to take my pills?
Can exercise affect my reflux?
Does GERD get worse with age?
Can my weight affect my GERD?
Obesity Risk factor for: • GERD • Erosive esophagitis • Esophageal adenocarcinoma
Aims of Acid-Suppressive Medications: Reduce gastric acid secretion The goal being to raise the intragastric p. H above 4
Reduce gastric acid secretion • The most common and effective treatment of peptic esophagitis or symptomatic GERD: – H 2 blocker – Proton pump inhibitor These therapies do not prevent reflux, but they reduce the acidity of the refluxate.
Therapeutic gain relative to the placebo for healing esophagitis • The H 2 receptor antagonists: 10 to 24 percent. • The proton pump inhibitors: 57 to 74 percent.
Complete relief from heartburn per week • Proton pump inhibitor (11. 5 percent). • H 2 receptor antagonist (6. 4 percent).
Acid-suppressive Medications H 2 receptor antagonists: • Cimetidine (Tagamet) • Ranitidine (Zantac) • Famotidine (Pepcid) • Nizatidine (Axid)
What do you do? • Patients who continue to have heartburn after six weeks of treatment with a standard dose of an H 2 antagonist.
Proton Pump Inhibitors
Mode of action of proton pump inhibitors (PPIs) l PPI inhibit H+/K+-ATPase in the secretory canaliculi of the stimulated parietal cell, thereby blocking the final common pathway of gastric acid secretion
What are the different proton pump inhibitors? How should they be taken?
Proton pump inhibitors Drug Dose (adult) oral Omeprazole 20 mg/ day; maintenance dose, 20 mg/ day Lansoprazole 30 mg/ day; maintenance dose, 15 mg/ day Pantoprazole 40 mg/ day; maintenance dose, 40 mg/ day Rabeprazole 20 mg/ day; maintenance dose, 20 mg/ day Esomeprazole 20 -40 mg/day; maintenance dose, 20 mg/day Dexlansoprazole 30 -60 mg/day; maintenance dose, 30 mg/day
Binding sites of different PPIs on the proton pump Cys 822 is the unique additional binding site for Pantoprazole only Cys 813 Cys 822 Cys 321 Pantoprazole � � Omeprazole � Esomeprazole � Lansoprazole � � Rabeprazole � � = Binding = No binding
No reactivation of ATPase activity by reducing agents after proton pump inhibition by Pantoprazole % reactivation of ATPase activity* H+K+ ATPase activity after Pantoprazole treatment depends entirely on de novo synthesis of pump 100 90 80 70 60 50 40 30 20 100 100 Omeprazole Esomeprazole Rabeprazole Lansoprazole Pantoprazole 70 0 *After 1 hour incubation with DTT (dithiotreitol) or GSH (glutathione) single oral doses (mg)
100 Pantoprazole Omeprazole Lansoprazole Rabeprazole Cytosol Lysosomes 50 Parietal cell Activated PPI after 1 hour (%) Activation of PPIs as a function of p. H 0 1 3 5 7 p. H
Pharmacokinetic comparison of five PPIs Pantoprazole shows a significantly higher AUC in comparison to other PPIs Concentration (u. Mol/L) 7. 0 6. 5 6. 0 Pantoprazole 40 mg 5. 5 5. 0 4. 5 Omeprazole 20 mg 4. 0 3. 5 Esomeprazole 20 mg 3. 0 Rabeprazole 20 mg Esomeprazole 40 mg 2. 5 2. 0 1. 5 Lansoprazole 30 mg 1. 0 0. 5 0. 0 0 2 4 6 8 10 12 14 Hours after dose 16 18 20 22 24
Do I need to take the medication every day or just when I have reflux?
What is Barrett’s Esophagus? The normal squamous epithelium is replaced by columnar epithelium.
Will I get cancer from having Barrett’s esophagus?
What can be done to make Barrett’s esophagus better or make it go away?
If I have Barrett’s esophagus, does it need to be followed?
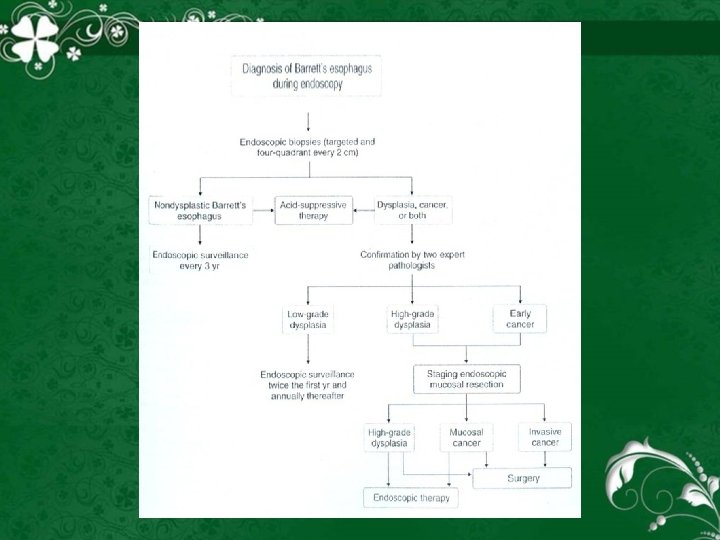
Treatment algorithm for patients Barrett’s esophagus.
Refractory GERD The definition of "refractory" GERD is unsettled. • Lack of a clinical response to: A PPI given one or twice daily.
Differential diagnosis • Nonerosive gastroesophageal reflux disease (NERD) • Achalasia • Esophageal cancer • Esophageal stricture • Other causes of esophagitis (NSAIDS, Pills, Caustic ingestion, Candida, herpes, radiation) • Gastric stasis • Sensitization to foods
Refractory GERD • Most patients with GERD who do not respond to a PPI have nonerosive reflux disease (NERD) or functional heartburn.
Treatment of refractory GERD • Reinforcement of lifestyle modification. • Switching to another PPI or doubling the PPI dose (divided at morning and at night before meal). F We usually double the dose for eight weeks before considering an alternative PPI.
Adjunctive therapy Prokinetic drugs • Prokinetic agents • Bethanechol • Metoclopramide • Domperidone Mechanisms • Increasing lower esophageal sphincter pressure • Enhancing gastric emptying, or improving peristalsis.
Treatment of helicobacter pylori & GERD • Antrum predominant gastritis (hypersecretors) • Corpus predominant gastritis (hyposecretors)
Chronic GERD • Symptoms occurring in three or more episodes a week for 6 months or longer.
If my GERD is chronic and possibly lifelong, do I need to take medications for life or are there any other options?
If my symptoms get better, can I stop taking medication?
Maintenance therapy It is determined by the rapidity of recurrence. • Recurrent symptoms in less than three months suggest disease best managed with continuous therapy. • Recurrences occurring after more than three months can be managed by repeated courses of acute therapy as necessary. PPIs at a standard dose is recommended.
Intermittent therapy • Intermittent (on-demand) therapy with an H 2 receptor antagonist or proton pump inhibitor may be successful in some patients with mild to moderate heartburn without moderate or severe esophagitis.
Safety of Medications • Hypergastrinemia • Pneumonia • Hypergastrinemia • Atrophic gastritis • Enteric infections • Vitamin B 12 malabsorption • Hip fracture and calcium malabsorption • Magnesium absorption
Bedtime H 2 receptor antagonist • Only in patients who failed PPI twice daily. • In patients with persistent acid reflux after the addition of an H 2 RA, antacids (eg, aluminum hydroxide, magnesium hydroxide) or sucralfate may provide some relief
Reducing weakly acidic reflux • Baclofen, a gamma aminobutyric acid B receptor agonist, was introduced as a potential add on treatment for patients who failed PPI treatment (once or twice daily). • The drug reduced TLESR rate by 40 to 60 percent, reduced reflux episodes by 43 percent, increased lower esophageal sphincter basal pressure, and accelerated gastric emptying.
Reducing weakly acidic reflux (cont. ) • In patients with persistent heartburn despite PPI treatment, doses up to 20 mg three times daily have been used. • CNS related side effects: (Somnolence, confusion, dizziness, lightheadedness, drowsiness, weakness, and trembling)
Reducing weakly acidic reflux (cont. ) • We usually begin by giving 10 mg twice daily, which can be increased slowly to 20 mg three times daily while carefully monitoring for side effects.
Esophageal p. H testing • Patients who fail PPI twice daily. • While off treatment to determine if reflux is the cause of their symptoms. • While on treatment to determine if there is continued pathological acid exposure despite a PPI.
Esophageal Manometry • Suspected achalasia, esophageal manometry should be considered. • The value of esophageal manometry in refractory GERD is very limited. • This is primarily because most of treatment failure patients have NERD or functional heartburn.
Management of heartburn or regurgitation symptoms
What should I do if the medication is not working?
Should I have surgery for my GERD?
Preoperative GERD evaluation: The most useful tests in making surgical decisions: • Upper endoscopy • Esophageal manometry • Assessment of esophageal length • Degree of hiatal herniation
Indications for operation of GERD • Gastrointestinal indications • Non Gastrointestinal indications
Gastrointestinal indications: • Failed optimal medical management • Noncompliance with medical therapy • High volume reflux • Severe esophagitis by endoscopy • Benign stricture • Barrett's columnar lined epithelium (without severe dysplasia or carcinoma)
Non Gastrointestinal indications About one-half of patients with GERD report upper respiratory symptoms including: • Cough (the most common extraesophageal symptoms) • Hoarseness • Laryngitis • Wheezing • Nocturnal asthma • Aspiration • Dental erosion
Fundoplication • Antireflux surgery should be considered in patients who require high doses of proton pump inhibitors to control symptoms, particularly in young patients who may require lifelong therapy.
Conclusions
Thanks for your attention