Gastroesophageal Reflux Disease Dr khorram GERD Physiologic refluxe




 80 males females")

















")













")










- Slides: 51
Gastroesophageal Reflux Disease Dr. khorram
GERD • Physiologic refluxe • Postprandial • Short-lived • Asymptomatic • Pathalogical refluxe • Symptomatic • Mucosal injery • nucturnal
• Epidemiology
GERD • 10 -20. / in the western world • 5. / in Asia
GERD is a common and significant problem: US study Prevalence (%) 80 males females 60 Any episode of GERD symptoms 40 At least weekly episodes of GERD symptoms 20 0 25– 34 35– 44 45– 54 55– 64 Age (years) Locke GR et al. Gastroenterology 1997; 112: 1448. 65– 74
GERD has a greater impact on quality of life than other common diseases Psychiatric patients Esophagitis, untreated Duodenal ulcer, untreated Angina pectoris Heart failure (mild) Normal female Normal male Hypertension, untreated 60 70 80 90 PGWB Index score Dimenas E. Scand J Gastroenterol 1993; 28 Suppl 199: 18. 100 110
Clinical Presentation of GERD Typical Esophageal • Heartburn • Acid regurgitation Atypical Dysphagia odynophagia Supraesophageal • Chest pain • Laryngitis • Asthma • Chronic cough • Aspiration pneumonia Tooth decay Water brush Globus sensation
Patients do not always correctly identify the symptom of heartburn Describing heartburn as “a burning feeling rising from the stomach or lower chest up towards the neck” can help patients recognise this symptom. 42% n=196 Carlsson R et al. Scand J Gastroenterol 1998; 33: 1023 Clinician interview/endoscopy • Functional dyspepsia diagnosed • Predominant heartburn excluded Reflux questionnaire • Identified a burning feeling rising from the stomach or lower chest up towards the neck as their main symptom
Pathophysiology of GERD Impaired acid neutralization by saliva and HCO 3 Impaired esophageal motility LES (inappropriate relaxation) Hiatal hernia Delayed gastric emptying/ gastroparesis LES=lower esophageal sphincter
Medications may aggravate GERD symptoms Impairment of LES function: Damage to the esophageal mucosa: • beta-adrenergic agonists • theophylline • acetylsalicylic acid and other NSAIDs • anticholinergics • tricyclic antidepressants • tetracycline • progesterone • quinidine • alpha-adrenergic antagonists • bisphosphates. • diazepam • calcium channel blockers.
• Diagnosis
• Diagnosis • Clinical if there is typical symptom
What are the Symptoms of Symptomatic GERD? • Heartburn • Regurgitation • Chest pain • Impaired QOL • Others (burning mouth/tongue) • Atypical (“supraesophageal”) symptoms
• Response to PPI?
• Indication of Endoscopy • • Alarm symptom Refractory GERD Barrett ‘s esophagus Duration of Gerd >5 -10 y
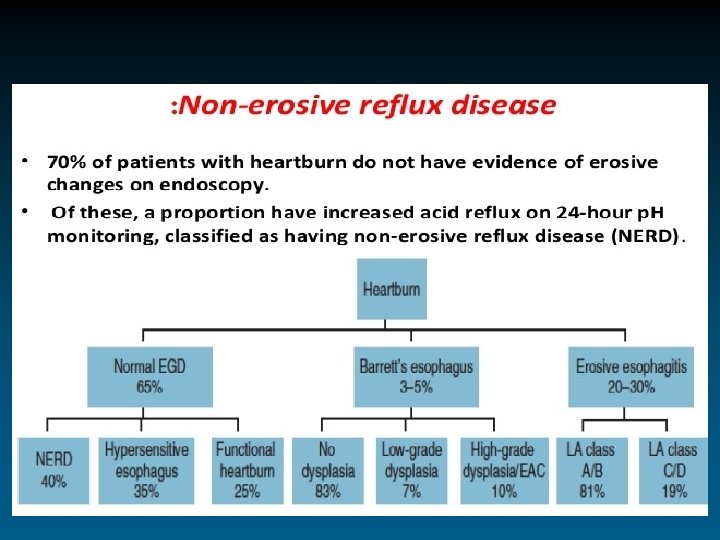
Phenotypic Classification of GERD NERD* 60 -70% Erosive Esophagitis 20 -30% *NERD: Non-Erosive Reflux Disease Fass et al. Alim Pharm Ther 2005 Barrett’s Esophagus 6 -10%
Taken from Medscape. com
Endoscopic Images Normal Squamocolumnar junction LA Grade A Esophagitis LA Grade D Esophagitis
Complication
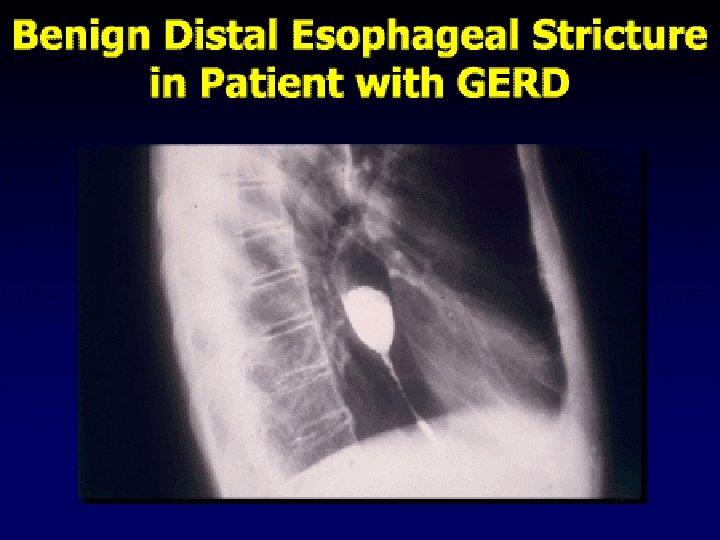
Esophageal stricture – endoscopic appearance
Metaplasia of the esophagus: Barrett’s esophagus Definition: a change in the esophageal epithelium of any length that can be recognised at endoscopy and is confirmed to have intestinal metaplasia by biopsy of the tubular esophagus and excludes intestinal metaplasia of the cardia. Squamous epithelium Columnar epithelium
Risk factor for barrett’s Eso • • Duration of GERD >5 -10 y Age >50 y Male H. H Smoker Obesity FH+
Barrett’s esophagus is associated with prolonged acid reflux Number of episodes 20 Time (minutes) 3 15 Barrett’s esophagus n=51 severe esophagitis n=30 moderate esophagitis n=45 controls n=24 2 10 1 5 0 Reflux episodes >5 minutes 0 Coenraad M et al. Am J Gastroenterol 1998; 93: 1068. Mean duration of reflux episode
The prevalence of Barrett’s esophagus increases with the duration of reflux symptoms Prevalence of endoscopic Barrett's esophagus (%) 25 20 15 10 5 0 <1 1– 5 5– 10 >10 Duration of symptoms (years) Lieberman DA et al. Am J Gastroenterol 1997; 92: 1293.
Does Barrett’s Esophagus Occur in the Absence of Heartburn? • EGD done on 961 pts scheduled for endoscopy; 556 never had heartburn • Conclusions: – BE is relatively common in persons age >40 years with no prior endoscopy – LSBE is very uncommon in patients who have no history of heartburn Rex D et al. Gastro 2003 HB (-) Overall (n=556) (n=961) Barrett’s 5. 6% 6. 8% LSBE 0. 36% 1. 2%
Reported adenocarcinoma risk in Barrett’s esophagus is dependent on the study size Size of study (patient-years) 1500 True risk is estimated as 0. 5% per patient-year 1000 500 0 0 10 20 Cancer risk per 1000 patient-years 30 Shaheen & Ransohoff 2002
Dysplasia in Barrett’s • Prevalence: LGD: 7. 3%; HGD: 3%1 • Dysplasia MUST be confirmed • HGD: must aggressively look for prevalent cancers • Screening and surveillance intervals? • Management options for HGD: – Esophagectomy – Ablation – Endoscopic mucosal resection 1 Sharma et al. Clin Gastro Hep 2006
A 35 -year old woman presents to her primary care physician because of six months of heartburn. Her medical history is only notable for chronic migraines. She has no dysphagia, odynophagia, or weight loss. She experiences symptoms 2 times a week, usually during stressful days at her job as a high school teacher. • What should be done at this point?
Initial Management of Heartburn A. Antacids and lifestyle changes B. H 2 -receptor antagonists C. Standard Proton pump inhibitor therapy D. High-dose Proton pump inhibitor therapy • Continuous? • On-Demand? E. Endoscopy and/or p. H testing followed by therapy based on results
Indications for additional investigations • Atypical history. • Symptoms are frequent and long-standing or do not respond to therapy. • Alarm symptoms are present: – severe dysphagia – weight loss – bleeding – hematemesis – mass in the upper abdomen – anemia
• Step up • Mild symptom <2 times per week • No evidence of erosive esophagitis • Step down • Sever symptom • Frequent symptom >2 times per week • Erosive esophagitis
The PCP places her on H 2 -receptor antagonists and recommends lifestyle changes and intermittent antacids. She returns a month later with no change in her symptoms. What should be done now?
• She is placed on once daily PPI therapy and referred for an upper endoscopy 2 weeks later, which is normal. She is still symptomatic.
A. Increase proton pump inhibitor to twice a day B. Refer for endoscopic treatment (Stretta) C. Refer for surgical treatment D. Perform p. H study E. Something else (like what? )
Why Do PPI’s Fail to Control Symptoms?
Reasons for PPI “Failure” • Patient non-compliance • Persistent esophageal acid exposure – Hypersecretory state – Large hiatal hernia – Nocturnal acid breakthrough • Acid-sensitive esophagus • Non-acid reflux • Wrong diagnosis • Functional heartburn (NOT GERD!!)
Wireless p. H monitoring (Bravo®)
Placement of Bravo® capsule
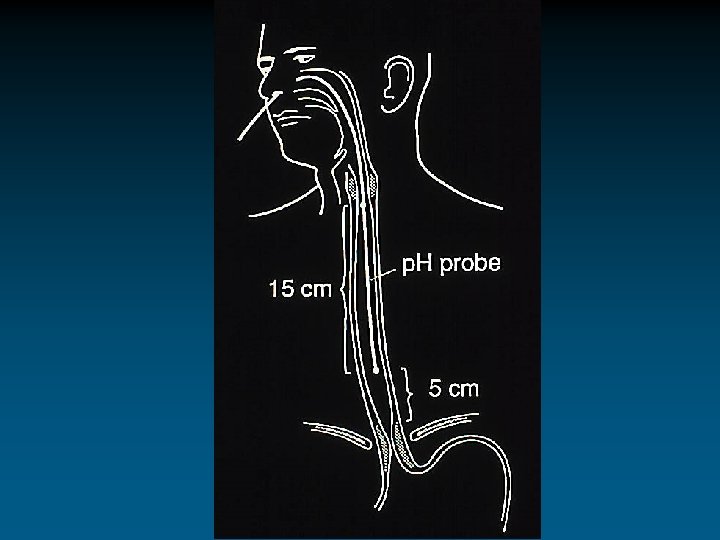
MII-p. H detected reflux Acid reflux Non-acid reflux 17 cm Impedance 15 cm 9 cm 7 cm 5 cm 3 cm 4 p. H esophageal gastric 4
Treatment Goals for GERD • • Eliminate symptoms Heal esophagitis Manage or prevent complications Maintain remission
Changes to diet and lifestyle can impair quality of life without improving GERD symptoms • Changes to diet and lifestyle are difficult for some patients and can significantly impair patient quality of life. • Studies into the negative effects of diet and lifestyle on GERD are few in number and the findings are statistically weak. • The criteria for evidence-based medicine are not met when diet and lifestyle changes are recommended. Dent 1992; Meining & Classen 2000
Mechanisms of Action of GERD Pharmacotherapy HCI H+ K+ PPIs block acid at its source in the proton pump H 2 RAs block the histamine receptor, interfering with one of the stimulation pathways Gastrin ACh=acetylcholine Antacids neutralize secreted HCl Histamine
Antireflux surgery – an alternative to pharmacological therapy • The efficacy of antireflux surgery in controlling GERD is similar to that of chronic PPI therapy. • The outcome of antireflux surgery is highly dependent on the skill and experience of the surgeon. • Surgery does not always end the need for antisecretory therapy to control the symptoms of GERD. Lundell et al 2001; Spechler et al 2001
Nissen fundoplication and the Toupet procedure Nissen fundoplication Toupet procedure
Predictors of success of surgery
Medication use in follow-up of patients from VA cooperative GERD study Spechler et al, JAMA 2001; 285: 2331
No evidence that antireflux surgery protects against cancer development Ye et al, Gastroenterology 2001; 121: 1286