GAS GANGRENE Dr Ehsanur Reza Shovan It is

















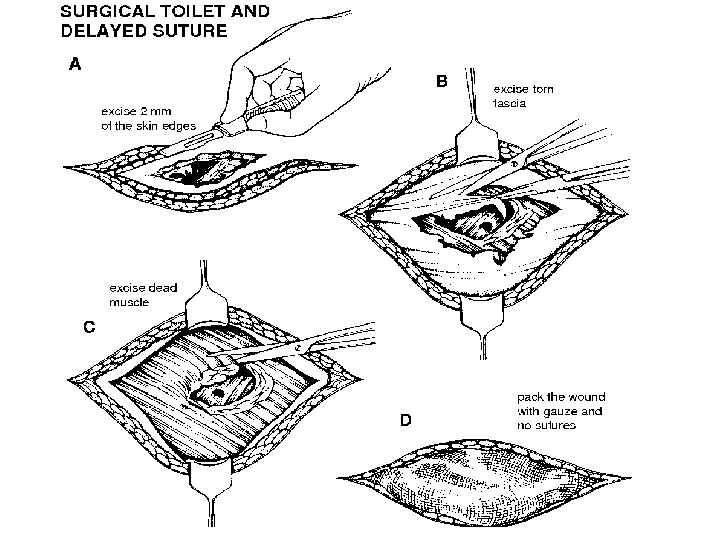
 Do a thorough wound toilet. (2) In high risk wounds give the")








- Slides: 28
GAS GANGRENE Dr. Ehsanur Reza Shovan
• It is a rapidly progressive, potentially fatal condition characterized by widespread necrosis of the muscles and subsequent soft-tissue destruction. • This is a dreaded consequence of inadequately treated missile wounds, crushing injuries and highvoltage electrical injuries.
Causative agent • Clostribium species – spore forming, Gram +ve c. sep ticum c. novyi c. Perfringens (mostly)
• They are present in the soil and have also been isolated from the human gastrointestinal tract and female genital tract. • Non-clostridial gasproducing organisms such as coliforms have also been isolated in 60– 85% of cases of gas gangrene.
Spores germinate Anaerobic environment vegetative cells multiply Carbohydrates Fermentation PATHOGENESIS Incubation period is Gas production In tissues 1 -7 days Toxemia and death Distension of tissues Interfering Blood supply Ischemia/ gangrene
Pathogenesis - Bacteria enters the broken skin or wound - Spores are produced - The toxins (lecithinase) and enzyme are produced - The bacteria are grow and ferment the muscle carbohydrate - The bacteria present in circulation system the anaerobic tissue present Examples of enzyme: colagenases, proteases and lipases - These enzymes will kill other host cell and extend the anaerobic environment - Produce gases (nitrogen, hydrogen sulphide and carbon dioxide) - Crepitant tissue ( destroyed tissue)
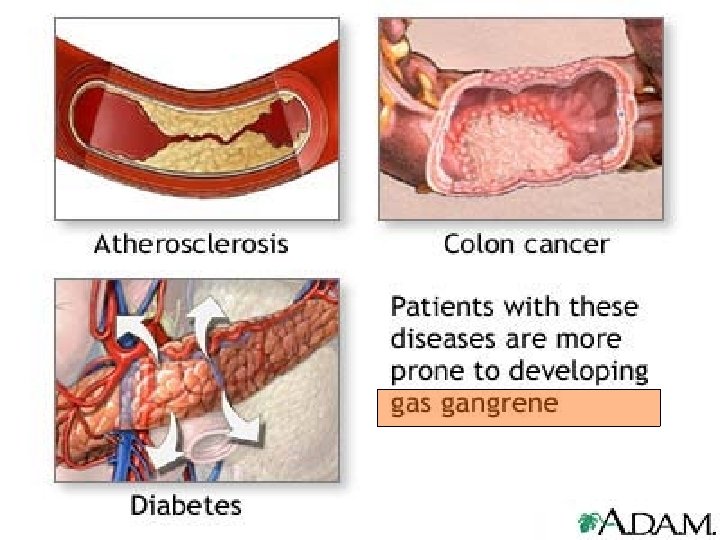
Epidemiology – The persons at risk those with Diabetes Mellitus, blood vessel disease and colon cancer – Contact with contaminated cloth and other foreign material – Trauma or recent surgical wound
Symptoms High fever Shock Massive tissue destruction Blackening of skin Severe pain around a skin of wound Blisters with gas bubbles form near the infected area, • the heartbeat and breathing become rapid. • • •
Presentation Crepitation in tissues, sickly sweet odor discharge, rapidly progressing necrosis, fever, hemolysis, toxemia, shock, renal failure, and death
Lab. Investigations Culture and sensitivity Storming fermentation Lecithinase test
G A S I N S O F T T I S S U E
G A S I N U T E R U S
G A S I N U T E R U S
G A S I N U T E R U S
Prevention • Cleaning the wound • Avoid the contaminated material • improve circulation in patients with poor circulation • antitoxin
Prevention (1) Do a thorough wound toilet. (2) In high risk wounds give the patient penicillin 1. 5 megaunits 4 hourly, or tetracycline
Treatment • High doses of antibiotic : Penicillin • The dead tissue is removed or limbs are amputated • No vaccine
10 megaunits of benzyl penicillin daily for 5 days as four 6 hourly doses. Or Tetracycline 0. 5 g intravenously or 1 g orally every 6 hours. Clostridia not sensitive to metronidazole, some other anaerobic bacteria are, so give it.
EXPLORATION Do this in a septic theatre, or even in the out-patient department, and not where clean cases go for operation.
AMPUTATION Amputate under a tourniquet Close the stump by delayed primary suture
Myonecrosis of right leg
Myonecrosis of left foot
Stump of above knee amputation
• Patients should be admitted to ICU and treated aggressively with careful monitoring. • The role of HBO is not as clear as in necrotising fasciitis but it is recommended in severe cases if the facilities are available. – increases the normal oxygen saturation in the infected wounds by 1000 -fold leading to • Bacteriocidal effect, • Improves neutrophil function, • Enhanced wound healing