gall bladder The gallbladder is a pearshaped sac

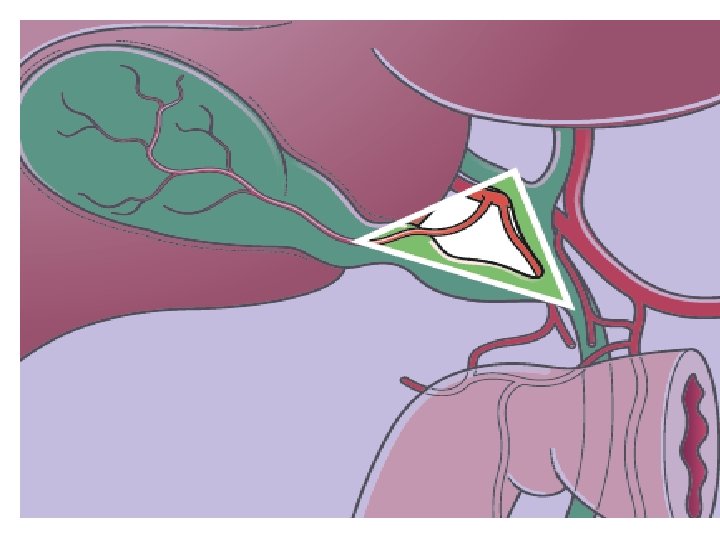
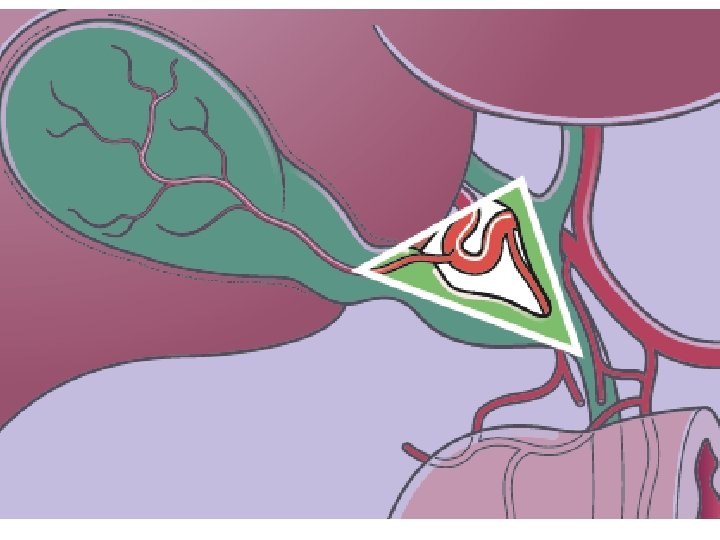
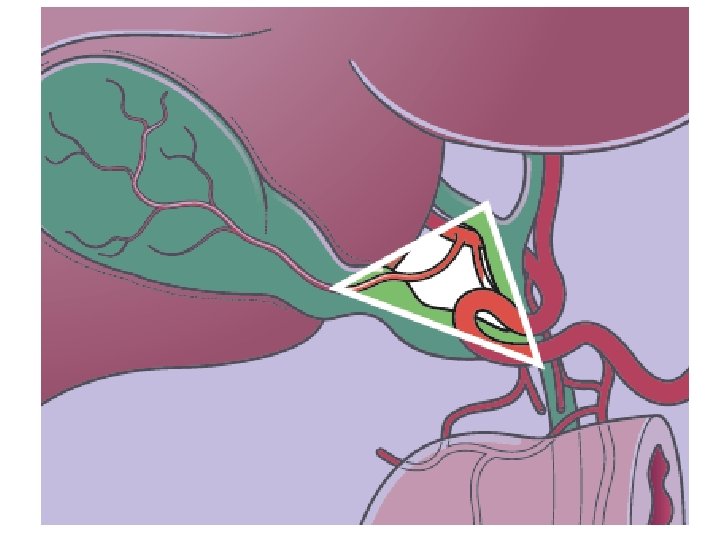
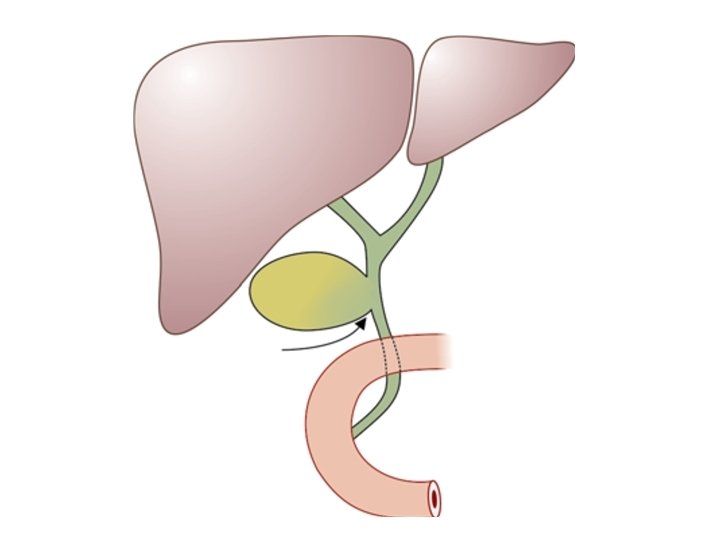
gall bladder The gallbladder is a pear-shaped sac, about 7 to 10 cm long, with an average capacity of 30 to 50 m. L. When obstructed, the gallbladder can distend markedly and contain up to 300 m. L The gallbladder is located in a fossa on the inferior surface of the liver. A line from this fossa to the inferior vena cava divides the liver into right and left liver lobes The cystic artery that supplies the gallbladder is usually a branch of the right hepatic artery (>90% of the time)an accessary cystic artery may arise from the gastroduodenal artery. The course of the cystic artery may vary, but it nearly always is found within the hepatocystic triangle, the area bound by the cystic duct, common hepatic duct, and the liver margin (triangle of Calot). Gall bladder lymphatics drain into nodes at the neck of the gallbladder. Frequently, a visible lymph node overlies the insertion of the cystic artery into the gallbladder wall (LN of LUDD).
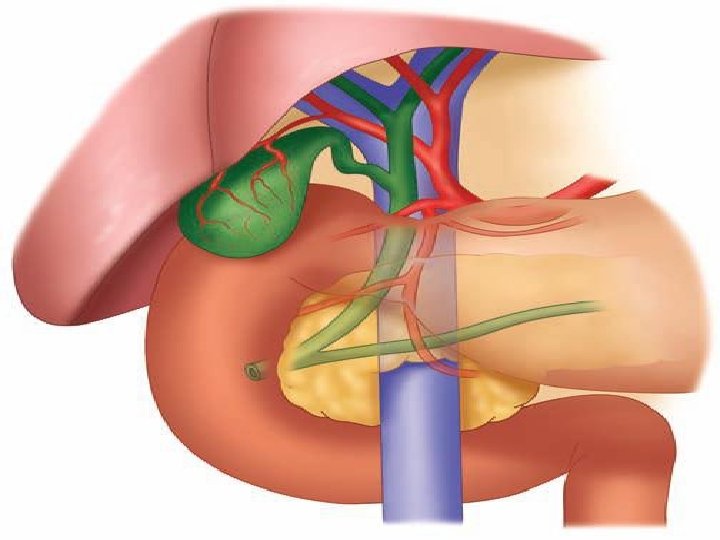

The common bile duct is about 7 to 11 cm in length and 5 to 10 mm in diameter. The upper third (supraduodenal portion)passes downward in the free edge of the hepatoduodenal ligament, to the right of the hepatic artery and anterior to the portal vein. The middle third (retroduodenal portion) of the common bile duct curves behind the first portion of the duodenum and diverges laterally from the portal vein and the hepatic arteries. The lower third (pancreatic portion) curves behind the head of the pancreas in a groove, or traverses through it and enters the second part of the duodenum, here, the pancreatic duct frequently joins it and opening in mucosa of the duodenum called ampula of vater while the sphincter around the duct called sphincter of oddi



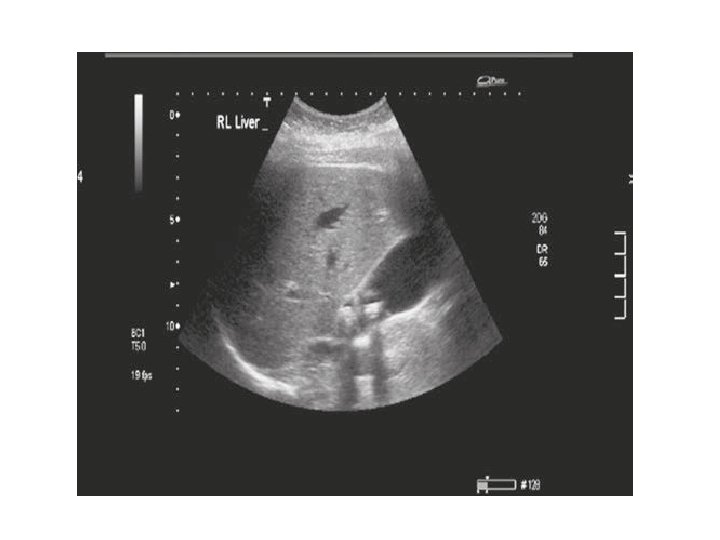
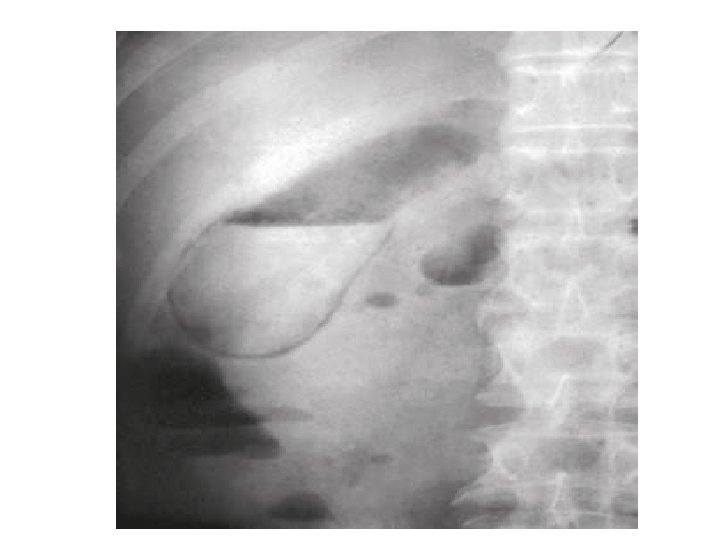
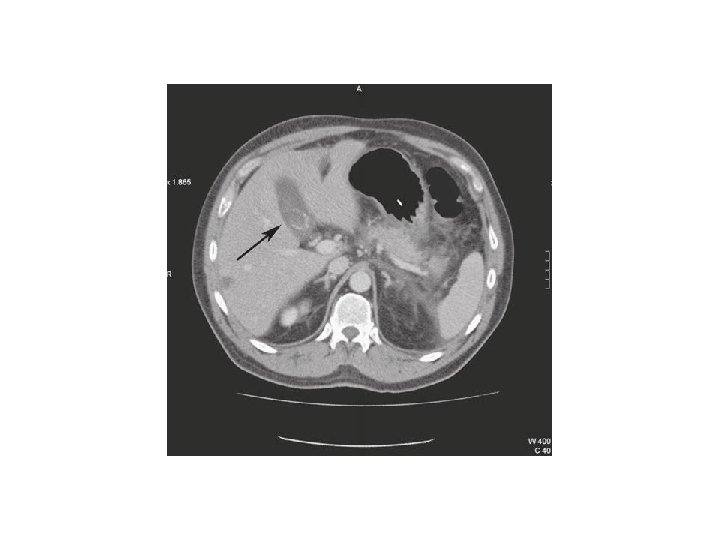
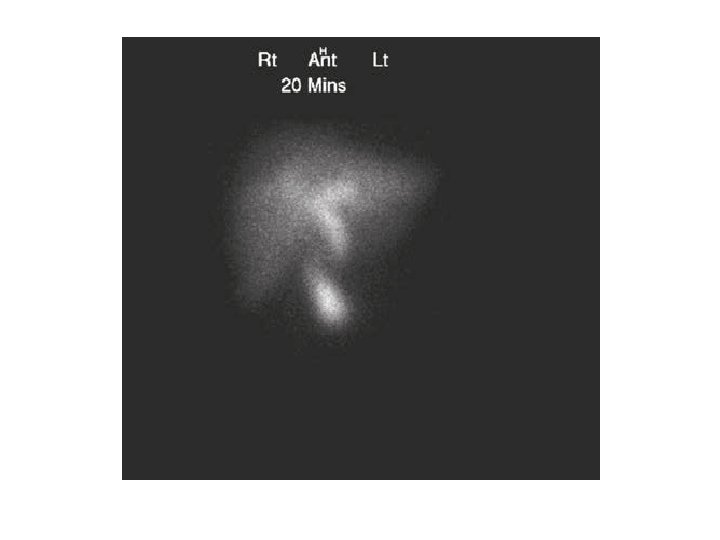
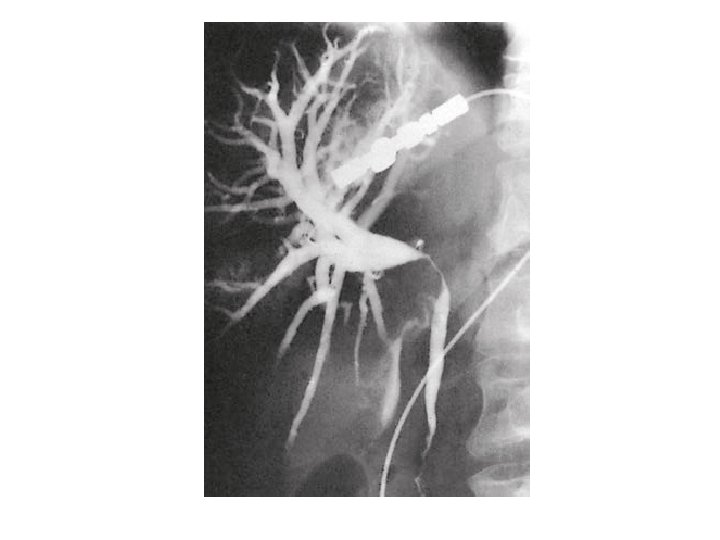
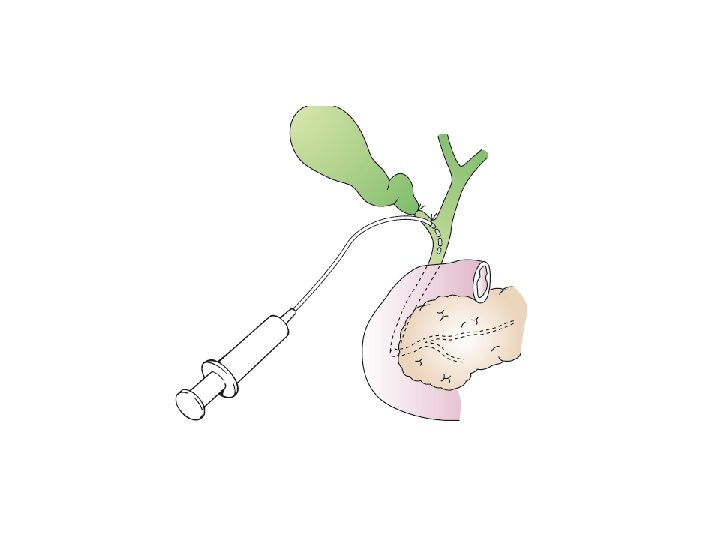
Investigation of gall bladder diseases; A-lab. investigation; 1 -CBP&ESR+blood film 2 -Liver function test B-radiological investigation 1 -Ultrasound: stones and biliary dilation 2 -Plain radiograph: calcification (porcelain gall bladder)in 25% associated with carcinoma, gas in gall bladder and biliary tree(airobilia), radio opague stones(10%) and need lateral view to differentiated from the right renal stone 3 - MRCP: anatomy and stones 4 -MDR-CT scan(multi-detecter scanner CT): anatomy liver, gall bladder and pancreatic cancer 5 -Radioisotope scanning (HIDA scan): function 6 -ERCP: anatomy, stones and biliary strictures(diagnostic or therapeutic) 7 --PTC: anatomy and biliary strictures and PTCD(therapeutic drainage of the biliary tree) 8 -Endoscopic ultrasound (EUS): anatomy, stones 9 -per operative choledochoscopy 10 -per operative pre exploratery cholangiography 11 -post operative post exploratery T-tube cholangiography



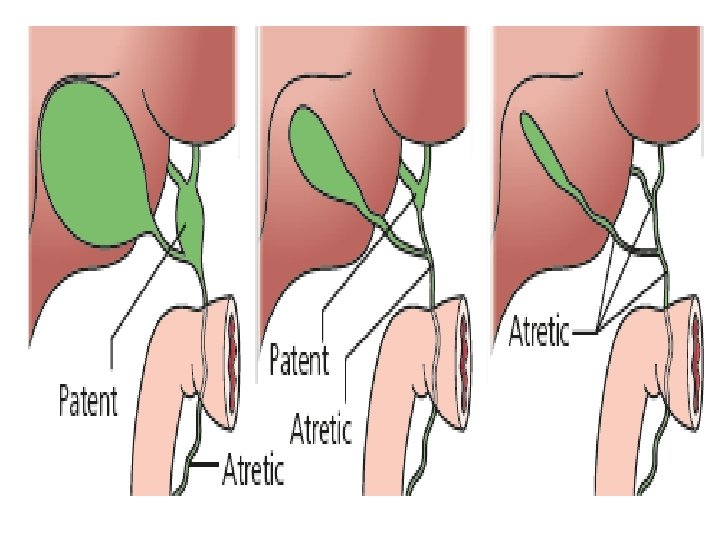
EXTRAHEPATIC BILIARY ATRESIA Aetiology and physiology Atresia is present in approximately 1 per 12 000 live births, and affects males and females equally. The extrahepatic bile ducts are progressively destroyed by an inflammatory process which starts around the time of birth. The aetiology is unclear. Intrahepatic changes also occur and eventually result in biliary cirrhosis and portal hypertension. Untreated, death from the consequences of liver failure occurs before the age of three years. The inflammatory destruction of the bile ducts has been classified into three main types; • type I: atresia restricted to the common bile duct; • type II: atresia of the common hepatic duct; • type III: atresia of the right and left hepatic ducts.

Clinical features About one-third of patients are jaundiced at birth. In all, however, jaundice is present by the end of the first week and deepens progressively. Liver function tests show an obstructive pattern with elevated bilirubin and alkaline phosphatase. The meconium may be a little bile stained, but later the stools are pale and the urine is dark. Prolonged steatorrhoea gives rise to osteomalacia (biliary rickets). Pruritus is severe. Clubbing and skin xanthomas, probably related to a raised serum cholesterol, may be present. Differential diagnosis This includes any form of jaundice in a neonate giving a cholestatic picture. Examples are; 1 - alpha -antitrypsin deficiency, 2 -cholestasis associated with intravenous feeding, 3 - choledochal cyst 4 - inspissated bile syndrome. 5 - Neonatal hepatitis is the most difficult to differentiate. Both extrahepatic biliary atresia and neonatal hepatitis are associated with giant cell transformation of the hepatocytes. Liver biopsy and radionuclide excretion scans are essential 1

Treatment Patent segments of proximal bile duct are found in 10 per cent of type I lesions. A direct Roux-en-Y hepaticojejunostomy will achieve bile flow in 75 per cent, but progressive fibrosis results in disappointing long-term results. A simple biliary-enteric anastomosis is not possible in the majority of cases in which the proximal hepatic ducts are either very small (type II) or atretic (type III). These are treated by the Kasai procedure, in which radical excision of all bile duct tissue up to the liver capsule is performed. A Roux-en-Y loop of jejunum is anastomosed to the exposed area of liver capsule above the bifurcation of the portal vein creating a portoenterostomy. Postoperative complications include bacterial cholangitis, which occurs in 40 per cent of patients. Repeated attacks lead to hepatic fibrosis and 50 per cent of long-term survivors develop portal hypertension, with one-third having variceal bleeding. Liver transplantation should be considered in children in whom a portoenterostomy is unsuccessful. Results are improving with 70– 80 per cent alive two to five years following transplant

Choledochal cyst Cystic disease of the biliary system is rare. Choledochal cysts are congenital dilations of the intra- and/or extrahepatic biliary system. The pathogenesis is unclear. Patients may present at any age with jaundice, fever, abdominal pain and a right upper quadrant mass. 60 per cent of cases are diagnosed before the age of ten years. Pancreatitis is not an infrequent presentation in adults. Patients with choledochal cysts have an increased risk of developing cholangiocarcinoma. Diagnosis by US, CT scan, . MRI, and MRCP Radical excision of the cyst is the treatment of choice with Reconstruction of the biliary tract using a Roux-en-Y loop of jejunum. Complete resection of the cyst is important because of the association with the development of cholangiocarcinoma. Resection and Roux-en-Y reconstruction is also associated with a reduced incidence of stricture formation and recurrent cholangitis
 11; -diverticulum)")
Classifications of the cholodochal cyst; 1 a&b; -diffuse cystic type(fusiform or saccular) 11; -diverticulum) 111; -diverticulum within the pancreas 1 V; -extension within the liver V; -only intrahepatic diletation
 Gallstones are the most common biliary pathology. It is estimated that gallstones")
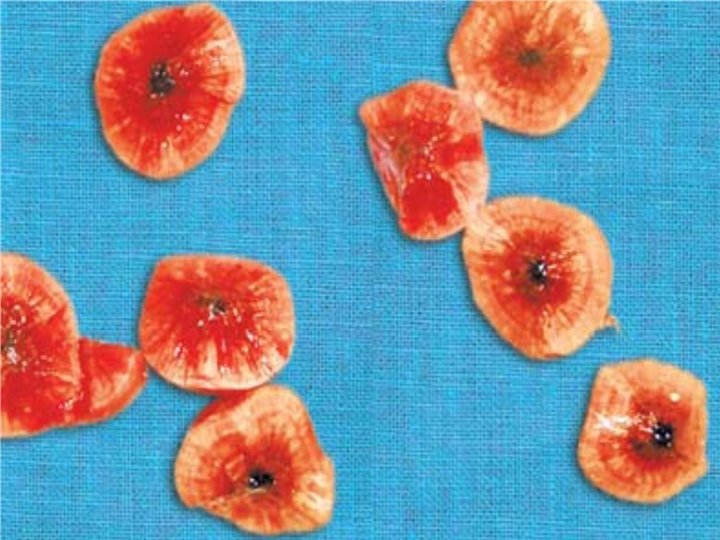
GALLSTONES (CHOLELITHIASIS) Gallstones are the most common biliary pathology. It is estimated that gallstones affect 10 – 15 per cent of the population in western societies. Causal factors in gallstone formation; Gallstones can be divided into three main types 1 -cholesterol 2 -pigment (brown/black) 3 - mixed stones. In the United States and Europe, 80 per cent are cholesterol or mixed stones, whereas in Asia, 80 per cent are pigment stones Pathophysiology of gall stones formation; -. 1 -metabolic theory; For Cholesterol to remain in the solution need the bile acid and phospholipid and bile acid with the cholesterol will form the micell which is hydrophilic and can remain and absorbed in the solution and any cause that increase the cholesterol or decrease the bile acid lead to supersaturated bile(lithogenic bile) and lead to formation of the gall stones ; a-high caloric diet B-obesity C-contraceptive pills and cholystyramine D-Resection of the terminal ileum, which diminishes the enterohepatic circulation, will deplete the bile acid pool and result in cholesterol supersaturation

2 -nidus of infection lead to aggregation of nucleated cholesterol crystal and stone formation 3 -stasis of bile lead to stone formation e. g vagatomy, total parenteral therapy, 4 -pigmented stones associated with haemolysis e. g spherocytosis, sickle cell anemia 5 -Stone formation is related to the deconjugation of bilirubin deglucuronide by bacterial-glucuronidase. Insoluble unconjugated bilirubinate precipitates. 6 -Brown pigment stones are also associated with the presence of foreign bodies within the bile ducts, such as endoprosthesis (stents), or parasites, such as Clonorchis sinensis and Ascaris lumbricoides.



Clinical features; Usually female more than male , fertile , forty years of age, fatty and flatulence dyspepsia(5 f) 1 -patient may be asymptomatic and we call it silent gall stone 2 -chronic cholecystitis; A-pain in the epigastric or right hypochondrial region of the abdomen radiating to the back and interscapular region and to the right shoulder, agrivated by fatty meal associated with nausea and vomiting, belching and dyspepsia and particularly flatulence dyspepsia B-on examination; tenderness in the epigastric and right hypochondrium 3 -acute cholecystitis; when the pain continue for more than 12 hrs and abdomen tenderness more sever with muscle guarding and positive murphy's and Boas sign with leukocytosis and moderately elevated liver function tests Differential diagnosis of acute cholecystitis Common Appendicitis Perforated peptic ulcer Acute pancreatitis Rare Acute pyelonephritis Myocardial infarction Pneumonia – right lower lobe

Complication of gall stones 1 -Biliary colic 2 -Acute cholecystitis 3 -Chronic cholecystitis 4 -Empyema of the gall bladder 5 -Mucocoele 6 -Perforation 7 -Biliary obstruction 8 -Acute cholangitis 9 -Acute pancreatitis 10 -Intestinal obstruction (gallstone ileus)

Diagnosis; 1 -history and physical examination 2 -US and Scan 3 -MRCP

Treatment of symptomatic gall stones is surgery and it is save to observe patients with asymptomatic gall stones but the indications of cholecystectomy in asymptomatic gall stones are; 1 -diabetic patient or immunosuppressed patient 2 -stones more than 2. 5 cm 3 -porcelian gall bladder carry 25% risk of malignancy 4 -those with congenital haemolytic anaemia when doing splenectomy 5 -those patients who are undergoing bariatric surgery for morbid obesity

Conservative treatment of acute cholecystitis; - more than 90 per cent of cases, the symptoms of acute cholecystitis subside with conservative measures. Non-operative treatment is based on four principles: • Nil per mouth (NPO) and intravenous fluid administration until the pain resolves. • Administration of analgesics. • Administration of antibiotics. As the cystic duct is blocked in most instances, the concentration of antibiotic in the serum is more important than its concentration in bile. A broad-spectrum antibiotic effective against Gram-negative aerobes is most appropriate (e. g. cefazolin, cefuroxime or gentamicin). • Subsequent management. When the temperature, pulse and other physical signs show that the inflammation is subsiding, oral fluids are reinstated followed by regular diet. .

The timing of surgery in acute cholecystitis remains controversial with many units favouring an early intervention within the first week, whereas others suggest that a delayed approach is preferable. 1 -Early cholecystectomy during acute cholecystitis appears to be safe and shortens the total hospital stay. Provided that the operation is undertaken within 5– 7 days of the onset of the attack, the conversion rate in laparoscopic cholecystectomy is higher in acute than in elective surgery. 2 -If an early operation is not indicated, one should wait approximately 6 weeks for the inflammation to subside before operating
 approach 2 -laproscopic cholecystectomy(lap. chole. ) Preparation for operation 1 -Full")
Cholecystectomy; 1 -conventional(open) approach 2 -laproscopic cholecystectomy(lap. chole. ) Preparation for operation 1 -Full blood count 2 -Renal profile and liver function tests 3 -Prothrombin time 4 -Chest x-ray and electrocardiogram (if over 45 years or medically indicated) 5 -Antibiotic prophylaxis 6 -Deep vein thrombosis prophylaxis 7 -Informed consent The golden role in cholecystectomy open or lap. is the identification of the Calots triangle

Lap. chole; 1 -supine position and general anesthesia with anti trendlenberg position with tilt to the left 2 -umbilical pneumoperitonium(Co 2 gas) with open(Hasson method)or close method using verres needle 3 -add epigastric port(surgeon port) and mid-clavicular port with additional optional port 4 -identy the calot triangle 5 -release the anterior and posterior peritoneal reflection 6 -identification and clipping of the cystic artery and cystic duct 7 -removal of the gall bladder with secure bed hemostasis

Open cholecystectomy Indication; 1 -For patients in whom a laparoscopic approach is not indicated 2 -in whom conversion from a laparoscopic approach is required an upper midline or a short right upper transverse incision is made centred over the lateral border of the rectus muscle. The gall bladder is appropriately exposed and packs are placed on the hepatic flexure of the colon, the duodenum and the lesser omentum to ensure a clear view of the anatomy of the porta hepatis. These packs may be retracted using the hand of the assistant (‘It is the left hand of the assistant that does all the work’ – Moynihan) or, alternatively, a stabilised ring retractor can be used to keep the packs in position.

Some golden rules to observe in case of difficulty: 1 • When the anatomy of the triangle of Calot is unclear, blind dissection should stop. 2 • Bleeding adjacent to the triangle of Calot should be controlled by pressure and not by blind clipping or clamping. 3 • When there is doubt about the anatomy, a retrograde or ‘fundusfirst’ cholecystectomy dissecting on the gall bladder wall down from the fundus to the cystic duct can be helpful. 4 • If the cystic duct is densely adherent to the common bile duct and there is the possibility of a Mirizzi syndrome (a stone ulcerating through the neck of the gall bladder into the common hepatic duct), the infundibulum of the gall bladder should be opened, the stone removed and the infundibulum oversewn. Attempts to completely dissect out the cystic duct will only lead to common hepatic or common bile duct injury. 5 • A cholecystostomy is rarely indicated, but, if it has to be done, as many stones as possible should be extracted and a large Foley catheter (14 F) placed in the fundus of the gall bladder with a direct track externally. By so doing, should stones be left behind in the gall bladder, these can be subsequently extracted with a choledochoscope.

; Pre-operatively; 1 -history of jaundice")
Indication for exploration of the common bile duct (choledochotomy); Pre-operatively; 1 -history of jaundice or cholangitis 2 -dilated CBD or stones in CBD 3 -abnormal liver function tests or high serum alkaline phosphatase Per-operative indication; 1 -dilated CBD more than 1 cm with wide cystic duct and multiple small gall stones seen by per-operative cholangiography 2 -palpable stones in CBD 3 -on table cholangiography showed stone in CBD

CHOLEDOCHOLITHIASIS It is stones in the CBD and biliary tree. Classification i. Primary—Rare—brown pigment stones. ii. Secondary—Common—black pigment stones/cholesterol stones. It is seen in 15% of gallstone disease; 75% are cholesterol stones, 15% are pigment stones. Primary stones They are formed in CBD and biliary tree itself, and are multiple, often sludge like, commonly pigment or mixed type, extends into hepatic ducts (Brown pigment stones). Causes: 1. Defective pathophysiology of biliary tree causing stasis, biliary dyskinesia 2. Congenital conditions like Caroli’s disease, choledochal cyst. 3. Infections and infestations like clonorchiasis, ascariasis. 4. Others: Low protein diet, malnutrition, obesity, females, old age Secondary biliary stones They are from gallbladder (gallstones) passes through cystic duct to CBD. Here CBD and biliary tree are otherwise normal. Secondary stones are better and easier to manage than primary stones. Commonly gallstones get impacted in supraduodenal portion of CBD.

Clinical Features 1 - Incidental CBD stones along with jaundice/without jaundice. 2 -Pain: It may be biliary colic; nonspecific abdominal pain; pain of ascending cholangitis, pain of pancreatitis. 3 -Jaundice—most common clinical manifestation. 4 -Fever with chills and rigors. Complications 1 -Liver dysfunction and biliary cirrhosis. 2 -White bile formation and liver failure. 3 -Suppurative cholangitis. 4 -Liver abscess. 5 -Septicaemia. 6 -Pancreatitis if CBD stone is near sphincter of Oddi blocking drainage of bile and pancreatic duct.

Investigations 1 -U/S abdomen; CBD diameter > 1 cm indicates biliary obstruction. 2 -ERCP, gold standard for diagnosis. 3 -MRCP. 4 -Liver function tests. 5 -Endoultrasonography is useful (EUS). It is more accurate. 6 -PTC if only indicated Treatment Preparation of the patient; 1 -Injection Vit. K 10 mg IM once a day for 5 days or FFP infusion to correct the prothrombin time 2 -IV antibiotics (cefoperazone, cefotaxime). 3 -Correction of dehydration. 4 -IV Mannitol daily 200 ml BD to prevent hepatorenal Syndrome Treatment; 1 -ERCP 2 -open or lap. Choledochotomy

After choledochotomy, stones are removed using Des jardin‘s choledocholithotomy forceps. Bake’s CBD dilator is used to confirm the CBD patency. T-tube (Kehr‘s) is then placed in the CBD and kept for 14 days. After 14 days a postoperative T-tube cholangiogram is done to see for free flow of dye into the duodenum, so that T-tube can be removed. If T-tube cholangiogram shows persistent stone(retained stone), it can be extracted after 6 weeks, through a basket (Dormia) or catheter (Fogarty) through the track or through a choledochoscope. Retained stones can also be removed through ERCP.
 Definition It is the jaundice that develops due to biliary")
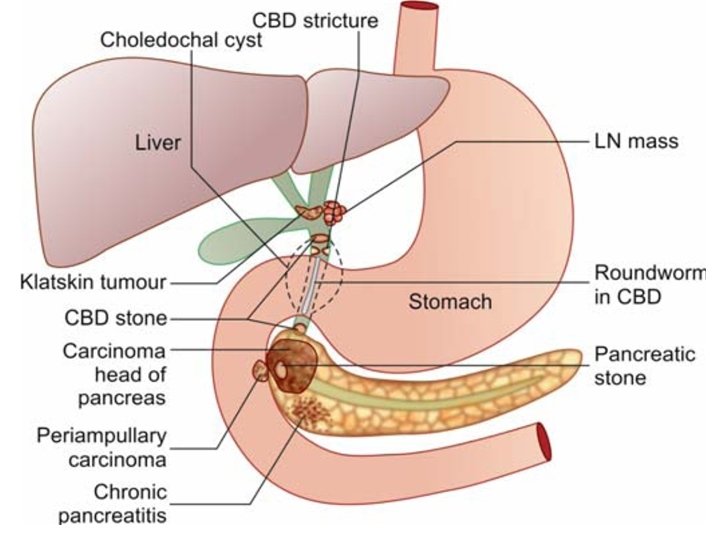
SURGICAL JAUNDICE (Obstructive Jaundice) Definition It is the jaundice that develops due to biliary obstruction, partial or complete or intermittent. It causes conjugated hyperbilirubinaemia. Normal serum bilirubin level is 0. 20. 8 mg%. Scleral icterus is visible when serum bilirubin level exceeds 2. 5 mg% Causes 1. Biliary atresia. 2. Choledochal cyst. 3. CBD stones. 4. Ascending cholangitis. 5. Biliary strictures. 6. Sclerosing cholangitis. 7. Carcinoma of head and periampullary region of the pancreas. 8. Cholangiocarcinoma. 9. Klatskin tumour (Carcinoma at the confluence of hepatic ducts above the level of the cystic duct and so will cause hydrohepatosis without GB enlargement). 10. Extrinsic compression of CBD by lymph nodes or tumours. 11. Parasitic infestations

Clinical Features Severe jaundice. Pruritus, more on the back and forearms. Fever, may or may not be present. Loss of weight. Loss of appetite. Pain in right hypochondrium, palpable gallbladder Courvoisier’s law may suggest inflammatory/neoplastic cause. Charcot’s triad as presentation in cholangitis. Steatorrhoea (more fatty stool) due to improper absorption of fat soluble vitamins

Investigation; 1 -liver function test 2 -US 3 -CT scan 4 -MRCP 5 -PTC 6 -ERCP

Preoperative preparation of patient with obstructive jaundice 1 - Proper diagnosis and assessment 2 -Injection vitamin K IM 10 mg for 5 days 3 -Fresh Frozen plasma—often requires 6 bottles or more 4 -Adequate hydration is most important 5/10% dextrose 5 -Blood transfusion in case of anaemia 6 -Mannitol 100 -200 ml BD IV to prevent hepatorenal syndrome 7 -Antibiotics like third generation cephalosporins.

Treatment of Obstructive Jaundice 1 -CBD stones A-ERCP stone removal, b- choledocholithotomy, C-transduodenal sphincteroplasty, D- choledochojejunostomy or choledochoduodenostomy. 2 - Carcinoma periampullary or head of pancreas A-Whipple’s operation B-triple bypass or ERCP stenting. 3 -Biliary stricture— A-Stenting B- choledochojejunostomy, Rouxen-Y hepaticojejunostomy. 4 --Klatskin tumour—Radical resection or palliative stenting . 5 -Biliary atresia—Kasai’s operation or liver transplantation . 6 -Choledochal cyst—Excision, hepaticojejunostomy, mucosal resection.

Management of pruritus: Pruritus may be due to retention of bile salts which activates the release of histamine in skin, central mechanism or by release of endogenous opioids. It is often diffi cult to treat. Once cause is treated and obstruction is relieved, pruritus will regress. Drugs and therapies used are—cholestyramine (ion exchange resin binds bile salts in intestine inhibiting their absorption), rifampin, ondansetron, gabapentin, sertratine, ursodeoxycholic acid, antioxidants, phototherapy, plasmapheresis
- Slides: 56